
Abstract
BACKGROUND AND PURPOSE: We present the results of a systematic review and meta-analysis examining outcomes of endovascular coiling of wide-neck and wide-neck bifurcation aneurysms with and without stent assistance. The aim of our study was to assess angiographic and clinical outcomes.
MATERIALS AND METHODS: We performed a comprehensive literature search for all articles on the endovascular coiling of wide-neck and wide-neck bifurcation aneurysms. Studies meeting our inclusion criteria and abstracted data were selected by 2 independent reviewers. Primary outcomes were >6-month complete or near-complete angiographic occlusion, aneurysm recanalization, and aneurysm retreatment. Secondary outcomes included initial complete or near-complete occlusion, long-term good neurologic outcome, procedure-related morbidity, and procedure-related mortality. Data were analyzed by using random-effects meta-analysis.
RESULTS: In total, 38 studies including 2446 patients with 2556 aneurysms were included. For all wide-neck aneurysms, immediate complete or near-complete occlusion rate was 57.4% (95% CI, 48.1%–66.8%). Follow-up near-complete occlusion rate was 74.5% (95% CI, 68.0%–81.0%). Recanalization and retreatment rates were 9.4% (95% CI, 7.1%–11.7%) and 5.8% (95% CI, 4.1%–7.5%), respectively. Long-term good neurologic outcome was 91.4% (95% CI, 88.5%–94.2%). For wide-neck bifurcation aneurysms, initial complete or near-complete occlusion rate was 60.0% (95% CI, 42.7%–77.3%), long-term complete or near-complete occlusion rate was 71.9% (95% CI, 52.6%–91.1%), and the recanalization and retreatment rates were 9.8% (95% CI, 7.1%–12.5%) and 5.2% (95% CI, 1.9%–8.4%), respectively.
CONCLUSIONS: Our study of angiographic and clinical outcomes for patients with wide-neck aneurysms demonstrates that endovascular coiling with or without stent-assisted coiling is safe, with low rates of perioperative morbidity and mortality. Initial and long-term angiographic outcomes were generally satisfactory, but not ideal. These data provide some baseline comparisons against which emergent technologies can be assessed.
With the advent of stent-assisted and balloon-assisted coiling, wide-neck and wide-neck bifurcation intracranial aneurysms are increasingly treated with endovascular techniques to prevent hemorrhage or recurrent bleeding. Both stent-assisted and balloon-assisted coiling have been shown to be safe and effective in the treatment of these aneurysms by allowing for increased packing density and lower rates of parent artery occlusion compared with conventional coiling alone.1⇓⇓⇓–5 Even in the era of endoluminal and intrasaccular flow diverters, many wide-neck and wide-neck bifurcation aneurysms will continue to be treated with conventional coiling, particularly with stent assistance.6⇓–8
We present the results of a systematic review and meta-analysis examining outcomes of endovascular coiling of wide-neck and wide-neck bifurcation aneurysms with and without stent-assisted coiling. The aim of our study was to assess both angiographic and clinical outcomes in order to provide overall data against which current and future emergent techniques can be compared.
Materials and Methods
Literature Search
A comprehensive literature search of the PubMed, Ovid MEDLINE, and Ovid EMBASE data bases was designed and conducted by an experienced librarian with input from the authors. The keywords intracranial aneurysm, cerebral aneurysm, aneurysm, wide-neck, bifurcation, complex, stent, balloon, endovascular, coiling, and coils were used in both “AND” and “OR” combinations. The search was limited to articles published from 1992 to week 18 of 2015 and is summarized in the On-line Table. All studies reporting patients with wide-neck or wide-neck bifurcation aneurysms treated with endovascular coiling with or without stent assistance were included. We used the following inclusion criteria: 1) English language, 2) study reporting a consecutive series of wide-neck and/or wide-neck bifurcation aneurysms treated with coiling, 3) series of at least 10 patients reporting angiographic and/or clinical outcomes, and 4) at least 6 months of angiographic follow-up. Review articles, comments, guidelines, technical notes, and editorials were excluded. The included studies were selected by 2 of the authors (B.Z., R.Y.), both with at least 1 year of experience in meta-analysis. Differences were resolved by a senior author (W.B.) with 5 years of experience in meta-analysis. Patients receiving endovascular treatment with flow diverters and intrasaccular flow diverters such as the Woven EndoBridge (WEB) aneurysm embolization system (Sequent Medical, Aliso Viejo, California) were excluded.
Outcomes and Data Extraction
For each study, we extracted the following baseline information: number of patients, aneurysm rupture status, sex, mean age, number of aneurysms treated, mean aneurysm size, mean aneurysm neck size, definition of wide neck, clinical outcome score used, length of clinical follow-up, and length of angiographic follow-up.
The primary outcomes of this study were >6-month follow-up, complete or near-complete angiographic occlusion, aneurysm recanalization, and aneurysm retreatment. Complete occlusion was defined as 100% occlusion or absence of angiographic filling in aneurysm neck or sac. Near-complete occlusion was defined as either 90%–99% occlusion or small residual neck filling without any filling of the sac.
Secondary outcomes included initial complete or near-complete occlusion, long-term good neurologic outcome, procedure-related morbidity, and procedure-related mortality. Good neurologic outcome was defined as an mRS score of 0–2 or Glasgow Outcome Score of 4–5 (good recovery, moderate disability). In cases where these scores were not available, good neurologic outcome was determined if the study used terms such as “no morbidity,” “good recovery,” or “moderate disability.”
In addition to studying overall outcomes of patients with wide-neck aneurysms receiving endovascular coiling, we performed 3 subgroup analyses including patients treated with non–stent-assisted coiling (ie, with or without balloon remodeling), patients treated with stent-assisted coiling, and patients with wide-neck bifurcation aneurysms. Outcomes of ruptured and unruptured aneurysms could not be separated because most studies did not stratify outcomes by rupture status.
Study Risk of Bias
We modified the New Castle Ottawa Quality Assessment Scale for Case Control Studies to assess the risk of bias of the studies included in this meta-analysis. This tool is designed for use in comparative studies; however, because none of the included studies were controlled, we assessed study risk of bias based on selected items from the tool focusing on the following questions: 1) Did the study include all patients or consecutive patients versus a selected sample?; 2) Was the study retrospective or prospective?; 3) Was angiographic and clinical follow-up satisfactory, thus allowing for ascertainment of all outcomes?; 4) Were outcomes clearly reported?; and 5) Were the interventionalists treating the patients the same as those who assessed angiographic and clinical outcomes?
Statistical Analysis
We estimated from each cohort the cumulative incidence (event rate) and 95% CI for each outcome. Event rates for each intervention were pooled in a meta-analysis across studies by using the random-effects model.9 Anticipating heterogeneity between studies, we chose this model a priori because it incorporates within-study variance and between-study variance. Heterogeneity of treatment effect across studies was evaluated by using the I2 statistic, in which I2 >50% suggests substantial heterogeneity.10 A χ2 analysis was used to compare outcomes between the stent-assisted and non–stent-assisted coiling groups. Statistical analysis was performed by using the software program OpenMeta[Analyst] (http://www.cebm.brown.edu/openmeta/).
Results
Study Selection and Characteristics
The initial literature search yielded 900 articles. Upon review of the abstracts and titles, 649 articles were excluded. We selected 239 articles for full-text screening. After screening, we excluded 213 articles, most of which were excluded because they did not separate outcomes of wide-neck versus narrow-neck aneurysms or had insufficient data. In total, we included 38 articles including 2446 patients with 2556 aneurysms. Of these, 656 patients had ruptured aneurysms and 1793 patients had unruptured aneurysms; in 107 aneurysms, the rupture status was not known. Among all aneurysms in the study, 496 were wide-neck bifurcation aneurysms. Regarding interventions, 376 were treated with coiling alone and 2090 were treated with stent-assisted coiling.
Of the 38 studies, 4 had a low risk of bias, 11 had a high risk of bias, and 23 had a medium risk of bias. The most commonly used definition for wide-neck aneurysm was a neck size of ≥4 mm and/or a dome-to-neck ratio of ≤2 (17 studies). In 5 studies, wide-neck aneurysms were defined as those with a neck size of ≥4 mm and/or a dome-to-neck ratio of ≤1.5. All included studies had at least 6 months of angiographic follow-up. The smallest study had 10 patients with 10 aneurysms, and the largest study had 468 patients with 500 aneurysms. A summary of included studies is provided in the On-line Table. The flow chart for study selection is provided in Fig 1.

Flow chart of literature search.
Angiographic Outcomes
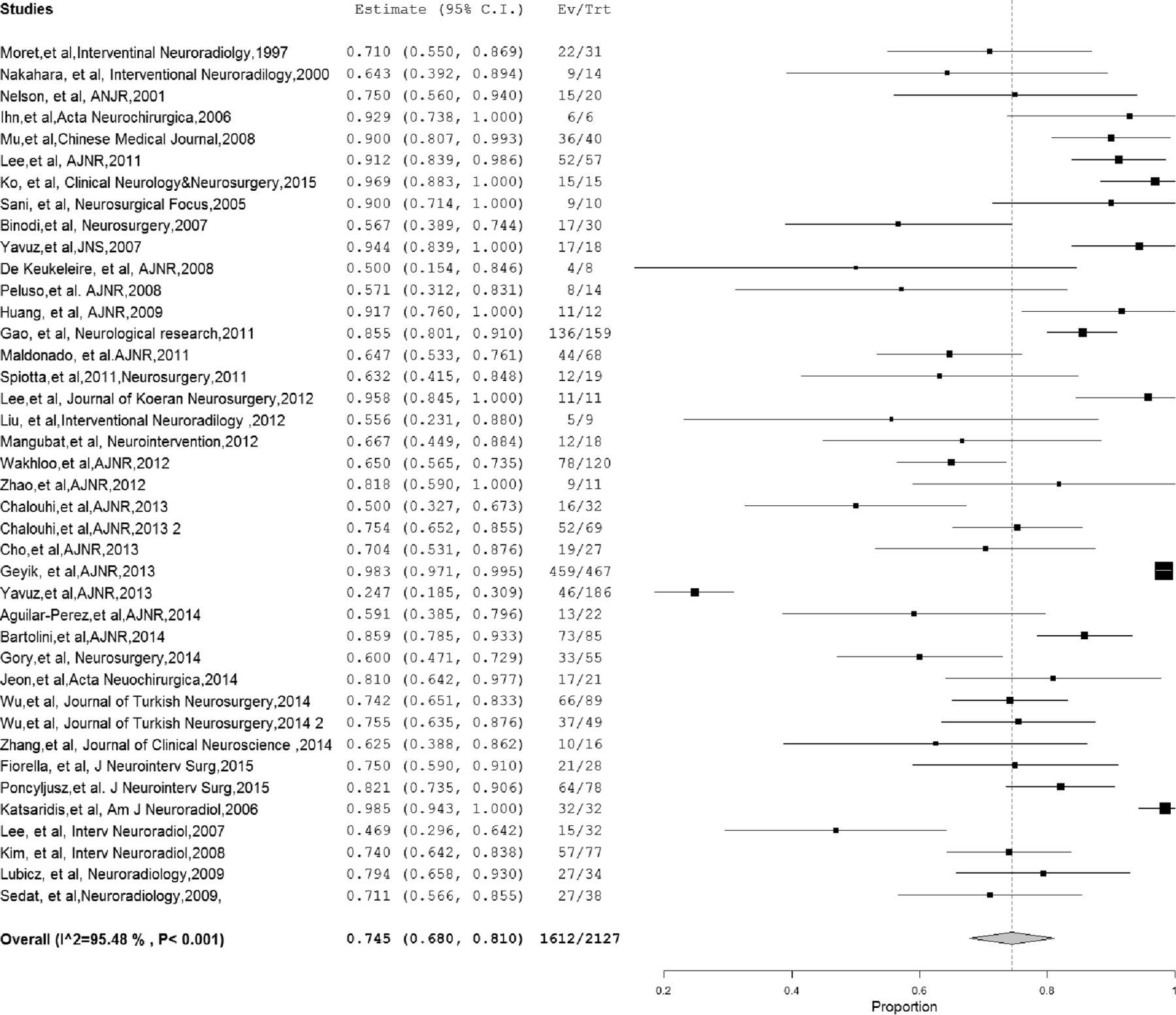
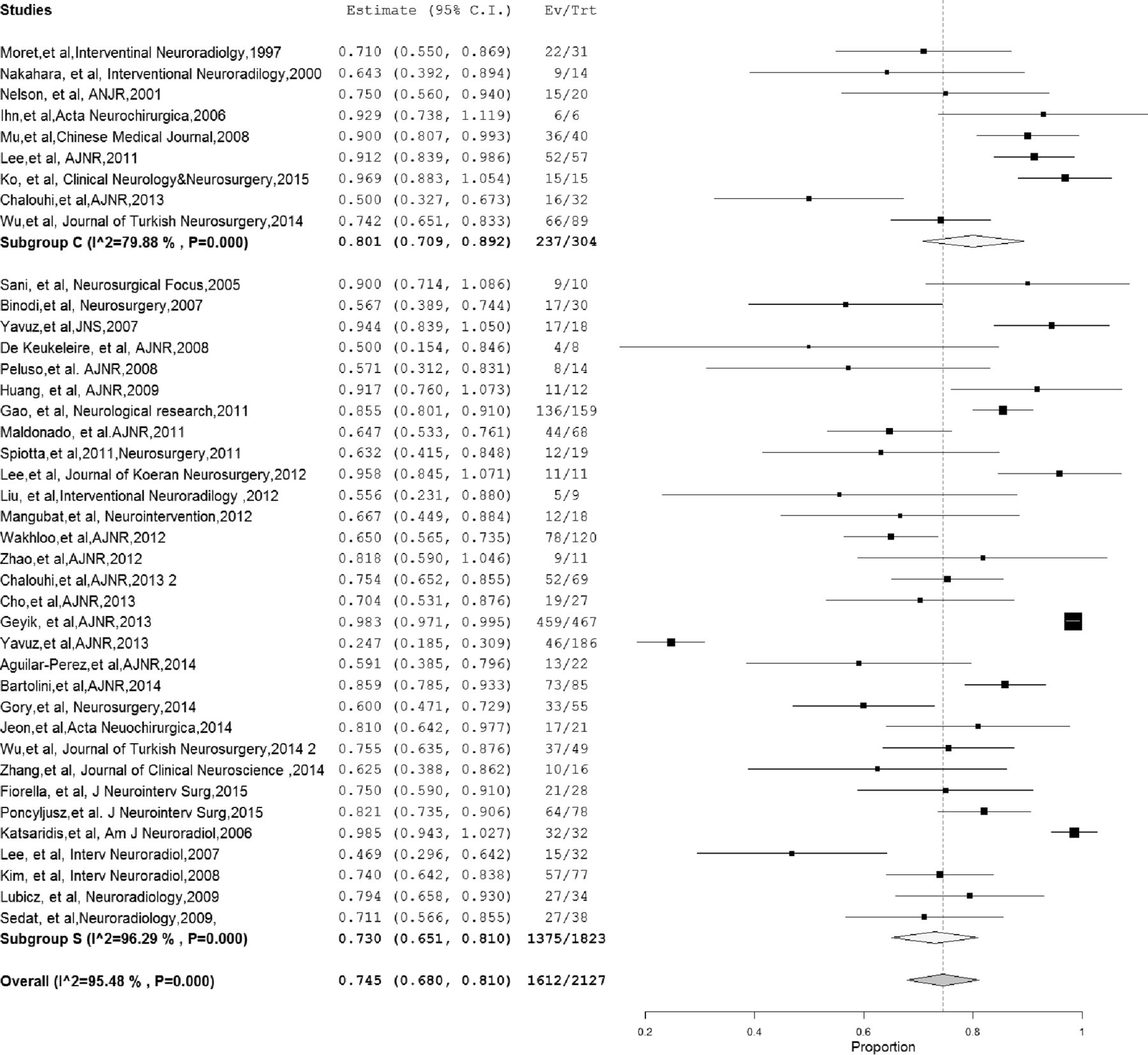
Overall, the rate of initial complete or near-complete occlusion was 57.4% (95% CI, 48.1%–66.8%) (Fig 2). Follow-up complete occlusion rates were 74.5% (95% CI, 68.0%–81.0%) overall, 80.1% (95% CI, 70.9%–89.2%) for coiling alone, and 73.0% (95% CI, 65.1%–81.0%) for stent-assisted coiling (P = .38) (Fig 3). Wide-neck bifurcation aneurysms had long-term complete occlusion rates of 71.9% (95% CI, 52.6%–91.1%).
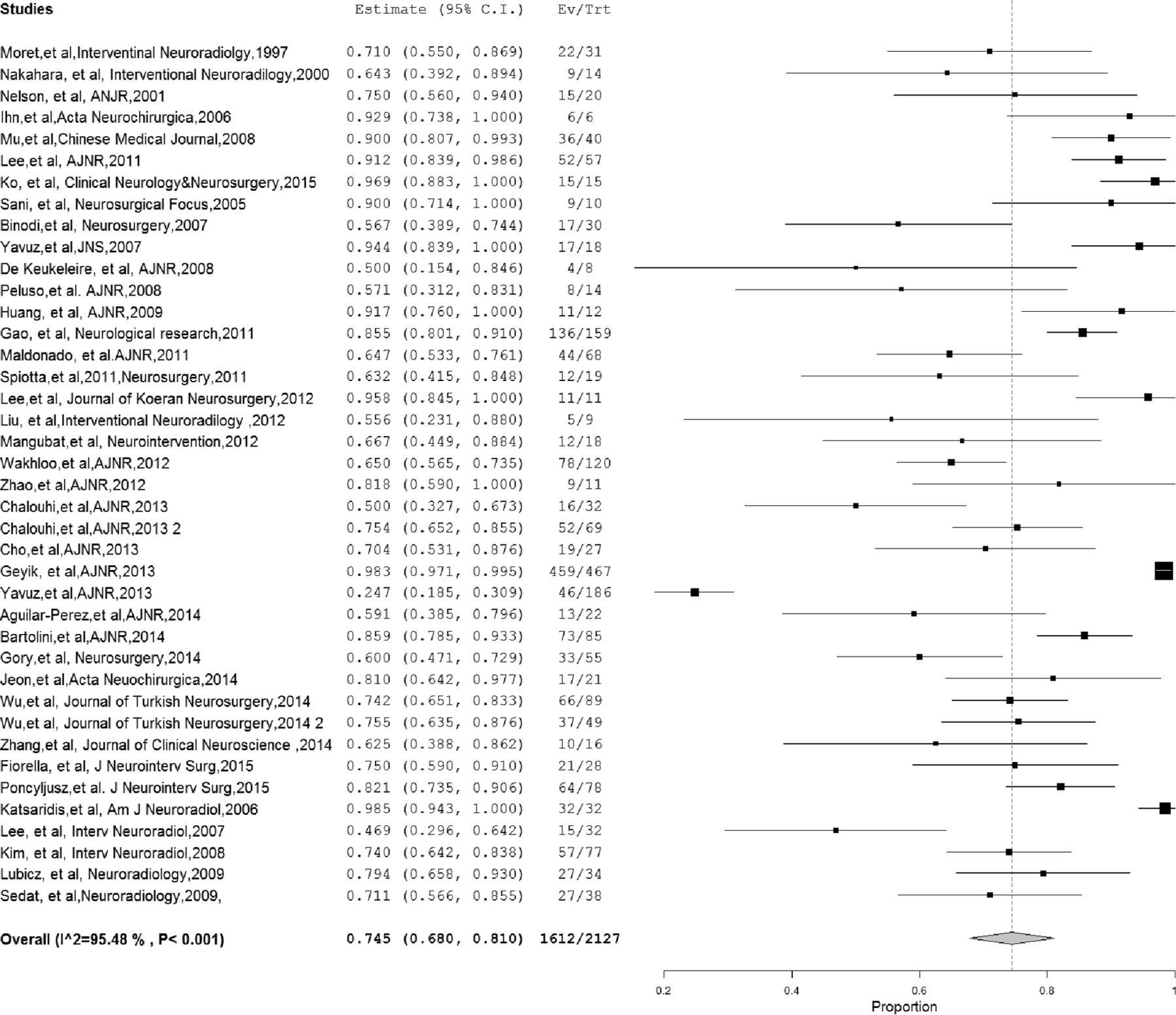
Forest plot for long-term complete or near-complete angiographic occlusion rates.

Forest plot for long-term complete or near-complete angiographic occlusion by treatment type.
Aneurysm recanalization rates were 9.4% (95% CI, 7.1%–11.7%) overall, 10.3% (95% CI, 4.3%–16.4%) for coiling alone, 9.2% (95% CI, 6.7%–11.7%) for stent-assisted coiling, and 9.8% (95% CI, 7.1%–12.5%) for wide-neck bifurcation aneurysms (P = .17). Aneurysm retreatment rates were 5.8% (95% CI, 4.1%–7.5%) overall, 5.5% (95% CI, 1.7%–9.2%) for coiling alone, 5.7% (95% CI, 3.8%–7.7%) for stent-assisted coiling, and 5.2% (95% CI, 1.9%–8.4%) for wide-neck bifurcation aneurysms (P = .47).
Clinical Outcomes
Overall procedure-related permanent morbidity rate for coiling with and without stent-assistance was 2.6% (95% CI, 1.7%–3.4%). Stent-coil procedure-related permanent morbidity rate was 1.9% (95% CI, 0.0%–3.7%), and wide-neck bifurcation procedure-related permanent morbidity rate was 4.4% (95% CI, 1.9%–7.0%). Procedure-related mortality rate was 1.0% (95% CI, 0.6%–1.5%).
The overall rate of good neurologic outcome for coiling with and without stent assistance was 91.4% (95% CI, 88.5%–94.2%). Stent-coil long-term good neurologic outcome rate was 89.0% (95% CI, 82.0%–96.1%), and the rate of good neurologic outcome for wide-neck bifurcation aneurysms was 86.3% (95% CI, 78.1%–93.4%). These data are summarized in the Table.
Results of meta-analysis
Heterogeneity
Heterogeneity of treatment effect across studies was evaluated by using the I2 statistic, in which I2 > 50% suggests substantial heterogeneity.10 There was no substantial heterogeneity for procedure-related morbidity and mortality for any of the groups. There was substantial heterogeneity for initial and long-term angiographic outcomes, long-term good neurologic outcome, and aneurysm recanalization rates for all study groups. I2 values were approximately 50% for retreatment for all groups.
Discussion
Our meta-analysis including 38 studies and over 2000 patients with wide-neck aneurysms treated with coiling and stent-assisted coiling demonstrated that though these techniques are generally safe, initial and long-term complete and near complete occlusion rates are not ideal. Overall, approximately 75% of aneurysms had complete or near-complete occlusion at last angiographic follow-up, and approximately 6% of aneurysms were retreated. Wide-neck aneurysms located at bifurcation points such as the MCA and basilar artery had complete occlusion rates of 72% and retreatment rates of approximately 5%. These findings are important because they suggest that the continued development of newer devices and techniques aimed at treating these complex lesions is needed to improve angiographic outcomes.
In general, treatment of wide-neck and wide-neck bifurcation aneurysms by using endovascular techniques is challenging. Embolization of these aneurysms without the use of adjunctive devices is difficult because of instability of the coil mass leading to the risk of coil protrusion into the parent artery. The risk of coil protrusion often makes attenuated packing of the aneurysm difficult or impossible to achieve, which can lead to lower rates of complete occlusion.11 Neurovascular stents act as a scaffold to prevent coil protrusion into the parent artery. Over the past 2 decades, a number of improvements to flexibility and delivery have been made to neurovascular stents, and as a result, these devices are increasingly used in the treatment of complex intracranial aneurysms.11,12 A recently published systematic review of stent-assisted coiling of wide-neck aneurysms including 702 aneurysms treated through 2011 demonstrated initial and long-term complete occlusion rates of 46% and 72%, respectively, and recanalization rates of 13%.11 However, improvements in the design of neurovascular stents and the advent of newer neurovascular stents will likely result in improvements in angiographic outcomes for stent-assisted coiling of wide-neck aneurysms. In fact, a recently published multicenter registry on the use of the LVIS stent (MicroVention, Tustin, California) in treating wide-neck aneurysms found complete and near-complete occlusion rates of 82% and 6%, respectively.13
Flow diverters such as the Pipeline Embolization Device (Covidien, Irvine, California) and Silk Device (Balt Extrusion, Montmorency, France) are increasingly being used in the treatment of complex, wide-neck intracranial aneurysms, particularly aneurysms of the ICA. In the Pipeline for Uncoilable or Failed Aneurysms clinical trial including over 100 patients with large and giant wide-neck ICA aneurysms, the rate of complete angiographic occlusion at 12 months was 87%, with only 5.5% of patients having residual aneurysm.14 There was even improvement in angiographic results with time; more than 95% of patients had complete angiographic occlusion at 5 years.15 However, it is important to note that flow-diverter treatment of bifurcation aneurysms can be challenging and is associated with higher morbidity rates and lower occlusion rates that those reported for aneurysms of the ICA. In a study of 14 patients with MCA bifurcation aneurysms treated with flow diverters, Caroff et al16 found complete occlusion rates of 62% and procedure-related morbidity rates of over 20%. Gawlitza et al17 found occlusion rates of just 33% after treatment of MCA and anterior communicating artery aneurysms with flow-diverter stents. The challenging factors for treating bifurcation aneurysms with flow diverters include the need to cover branch vessels and perforators with the flow-diverter stent and technical challenges with device delivery.
Over the past several years, intrasaccular flow diverters such as the Woven EndoBridge system have emerged as effective techniques for the treatment of wide-neck bifurcation aneurysms. These devices function by disrupting intra-aneurysmal flow and creating intra-aneurysmal thrombosis.18 The devices are designed to essentially plug the neck of the aneurysm sac and prevent inward blood flow. One advantage of the Woven EndoBridge device is the lack of a need for dual antiplatelet therapy, which is especially important in the setting of treating ruptured aneurysms. The Woven EndoBridge has been the subject of numerous clinical studies designed to investigate the efficacy of treating intracranial, wide-neck bifurcation aneurysms. Thus far, early small studies suggest that the Woven EndoBridge device is associated with higher angiographic occlusion rates than stent-assisted coiling in the treatment of wide-neck bifurcation aneurysms with similar low rates of procedure-related morbidity and mortality. In a study of 52 patients with 55 aneurysms, Behme et al19 found favorable angiographic outcomes in 75% of cases, with all patients experiencing good neurologic outcomes on long-term follow-up. In a multicenter study of 45 patients with 45 aneurysms, Lubicz et al20 found complete or near complete occlusion in 90% of cases, with good long-term neurologic outcome rates of 93%. The WEB Clinical Assessment of IntraSaccular Aneurysm Therapy (WEBCAST) study, which examined outcomes for treatment of wide-neck bifurcation aneurysms in 51 patients, found complete and near-complete occlusion rates of 85% and procedure-related morbidity and mortality rates of 2% and 0%, respectively.21
Limitations
Although data in this meta-analysis were derived from a strictly defined patient population with at least 6 months of follow-up, our study has limitations. Almost all studies were retrospective case series; thus, our study undoubtedly suffers from selection bias. In our assessment of study risk of bias, most of the studies had a medium to high risk of bias. I2 values were above 50% for most outcomes, indicating substantial heterogeneity. In addition, most studies did not have neurologic outcomes assessed by an independent physician, and these assessments were not blinded to the aneurysm treatment used. Publication bias is also possible because centers with better outcomes may have been more prone to report their results. We did not have access to individual patient data and, consequently, could not investigate the effect of important factors (including age, aneurysm size and location, medical comorbidities, etc) on angiographic and clinical outcomes. We were unable to stratify outcomes by aneurysm rupture status; however, most aneurysms included in this study were unruptured. Overall, the quality of evidence (confidence in estimates) is low because of imprecision, heterogeneity, and methodologic limitations of the included studies.22,23 Nevertheless, this systematic review and meta-analysis provides useful data to share with families when discussing the possible outcomes of stent-assisted coiling of wide-neck and wide-neck bifurcation aneurysms. In addition, this study could serve as a benchmark for which to compare results of newer stents, flow diverters, and intrasaccular flow diverters.
Conclusions
Our study of angiographic and clinical outcomes for patients with wide-neck aneurysms demonstrates that endovascular coiling, with or without stent-assisted coiling, is generally safe, with low rates of perioperative morbidity and mortality. Initial and long-term angiographic outcomes were satisfactory, but not ideal, and lower than those reported for treatment of similar aneurysms with newer technologies such as intraluminal and intrasaccular flow diverters. Future comparative clinical trials could be considered to identify the best treatments for wide-neck and wide-neck bifurcation aneurysms.
Footnotes
Disclosures: Giuseppe Lanzino—UNRELATED: Consultancy: Covidien/Medtronic.* David F. Kallmes—UNRELATED: Board Membership: GE Healthcare,* Comments: Cost effectiveness board; Consultancy: Medtronic,* Comments: Planning and implementing clinical trials; Grants/Grants Pending: MicroVention,* Medtronic,* Codman,* Surmodics,* Sequent,* NeuroSigma,* Comments: Preclinical research and clinical trials. *Money paid to the institution.
References
- Received October 22, 2015.
- Accepted after revision March 1, 2016.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Large Single-Center Experience with Short-Term Follow-up of Neqstent-Assisted Coiling
- Endovascular treatment of wide-necked intracranial aneurysms using the Nautilus Intrasaccular System: initial case series of 41 patients at a single center
- Improving visualization of three-dimensional aneurysm features via segmentation with upsampled resolution and gradient enhancement (SURGE)
- Use of the Woven EndoBridge Device for Sidewall Aneurysms: Systematic Review and Meta-analysis
- A mini-review of intrasaccular flow diverters
- Multi-centric European post-market follow-up study of the Neuroform Atlas Stent System: primary results
- Pivotal trial of the Neuroform Atlas stent for treatment of posterior circulation aneurysms: one-year outcomes
- eCLIPs bifurcation remodeling system for treatment of wide neck bifurcation aneurysms with extremely low dome-to-neck and aspect ratios: a multicenter experience
- Endovascular treatment of wide-necked intracranial aneurysms using the novel Contour Neurovascular System: a single-center safety and feasibility study
- Long-Term Outcomes of the WEB Device for Treatment of Wide-Neck Bifurcation Aneurysms
- A systematic review of non-trunk basilar perforator aneurysms: is it worth chasing the small fish?
- Flow diversion treatment of aneurysms of the complex region of the anterior communicating artery: which stent placement strategy should 'I use? A single center experience
- Stent-assisted coiling of cerebral aneurysms using the Y-stenting technique: a systematic review and meta-analysis
- Evaluating the safety and technical effectiveness of a newly developed intravascular flow isolator' stent for the treatment of intracranial aneurysms: study protocol for a first-in-human single-arm multiple-site clinical trial in Japan
- Treatment of Wide-Neck Intracranial Aneurysms with the Woven EndoBridge Device Associated with Stenting: A Single-Center Experience
- A new method to statistically describe microcatheter tip position in patient-specific aneurysm models
- Y-Stent-Assisted Coiling of Wide-Neck Bifurcation Intracranial Aneurysms: A Meta-Analysis
- Long term follow-up of bifurcation aneurysms treated with braided stent assisted coiling and complex T- and Y- stent constructs
- Two-Center Experience in the Endovascular Treatment of Ruptured and Unruptured Intracranial Aneurysms Using the WEB Device: A Retrospective Analysis
- Efficacy and Safety of the Woven EndoBridge (WEB) Device for the Treatment of Intracranial Aneurysms: A Systematic Review and Meta-Analysis