
Abstract
SUMMARY: Percutaneous image-guided biopsy currently has a central role in the diagnostic work-up of patients with suspected spondylodiscitis. However, on the basis of recent evidence, the value of routine image-guided biopsy in this disease can be challenged. In this article, we discuss this recent evidence and also share a new diagnostic algorithm for spondylodiscitis that was recently introduced at our institution. Thus, we may move from a rather dogmatic approach in which routine image-guided biopsy is performed in any case to a more individualized use of this procedure.
The incidence of spondylodiscitis is rising in the developed world due to aging of the population with inherent comorbidities that increase the risk of infection and improved diagnosis because of widespread use of MR imaging.1 The diagnosis of spondylodiscitis and the microbiologic culprit can be confirmed by a combination of MR imaging findings with blood cultures or cultures of spinal or paraspinal tissue samples. The guidelines of the Infectious Diseases Society of America recommend performing MR imaging and obtaining blood cultures in all patients with suspected spondylodiscitis. They also recommend image-guided biopsy when the microbiologic diagnosis has not been established by blood cultures or serologic tests.2,3 The same guidelines advise repeat image-guided percutaneous biopsy or proceeding to open biopsy if the initial biopsy result remains negative.2,3 Thus, percutaneous image-guided biopsy currently has a central role in the diagnostic work-up of patients with suspected spondylodiscitis.
Arguments for Routinely Performing Percutaneous Image-Guided Biopsy
Proponents of routinely performing percutaneous image-guided biopsy argue that a microbiologic diagnosis should be established to target antimicrobial treatment and ultimately improve clinical outcome. In addition, antibiotic resistance may potentially be reduced with such an approach because it allows exact targeting of the specific microbe. Furthermore, establishing a microbiologic diagnosis may prevent the need for an open or surgical intervention when infection progresses.2,3 It is also argued that pathologic examination of biopsy specimens may help differentiate an infectious from a malignant or degenerative process.2,3 Finally, the Infectious Diseases Society of America guidelines mention that the sensitivity of image-guided biopsy varies between 30% and 74%, which seems fairly high, though these numbers are based on only 3 studies that were cited in these guidelines.2,3
Practical Issues of Percutaneous Image-Guided Biopsy
Percutaneous image-guided biopsy can be performed using conventional x-ray fluoroscopic or CT guidance, with most previously published studies using CT for this purpose in spondylodiscitis.4 The advantages of CT-guided biopsy over x-ray fluoroscopically guided biopsy are more accurate localization, multiplanar views, the ability to differentiate necrotic bone and solid lesions, and not exposing the operator to ionizing radiation.1 Although CT-guided biopsy is relatively safe, it is still an invasive procedure with a non-negligible risk of complications. Minor complications such as transient paresis, hematoma, postbiopsy fever, pain, bruising, and swelling occur in around 2%.5,6 Major complications such as spinal cord injury are rare but have also been reported.7 Furthermore, lying still during the procedure may be burdensome to some patients who are ill and have severe back pain due to spondylodiscitis, in our experience. The use of potentially harmful ionizing radiation should also be taken into account.8
Culture Yield of Percutaneous Image-Guided Biopsy: The Actual Numbers
A crucial topic is the culture yield of the spinal or paraspinal biopsy samples that have been obtained. According to a meta-analysis that included 33 studies, image-guided biopsy has a positive culture yield of approximately 48%.4 In another more recent meta-analysis that included 10 studies, the positive culture yield of CT-guided biopsy in suspected spinal infection was 33%.9 The latter percentage of 33% corroborates both the results of some more recent original studies investigating the microbiological yield of the first biopsy in suspected spondylodiscitis10,11 and a meta-analysis that included 8 studies on the culture yield of repeat biopsy after an initial biopsy with negative findings.12 This percentage is also considerably lower than the 30%–74% range that was described in the Infectious Diseases Society of America guidelines.2,3 Furthermore, cultures may be positive for possible skin contaminants such as coagulase-negative Staphylococcus species (except Staphylococcus lugdunensis) and Cutibacterium species; thus, the spinal or paraspinal biopsy culture may be inconclusive.2,3
Recent Evidence
The practical disadvantages of percutaneous image-guided biopsy5⇓⇓-8 and the relatively low positive culture yield of 33%9⇓⇓-12 raise the question of whether this procedure should be routinely performed in all patients with suspected spondylodiscitis. Some recent evidence can also be considered supportive of this potential paradigm shift.
First, a recent study from Korea that included 141 patients with pyogenic spondylitis in whom micro-organisms were isolated from both blood and tissue cultures reported that the species of blood and tissue isolates were identical in 135 patients (95.7%, 135/141).13 If one excluded the 4 anaerobic isolates, antibiotic susceptibility patterns were identical in 128 patients (97.7%, 128/131).13 These results suggest that a positive blood culture from patients with pyogenic spondylitis could preclude the need for additional tissue cultures.13 This suggestion is also in line with the Infectious Diseases Society of America guidelines that recommend against obtaining a tissue sample in the setting of positive blood cultures, particularly in patients with Staphylococcus aureus, S lugdunensis, or Brucella species bloodstream infection.2,3 Therefore, an argument can be made to delay any decision about the need for percutaneous image-guided biopsy until blood culture results are available. Broad spectrum antibiotics should be administered until blood cultures are known, covering the most common causative micro-organisms. This approach will save patients with blood cultures with positive findings an unnecessary biopsy.
Second, even when the microbiologic culprit remains unknown, it may still be possible to start an effective empiric treatment in patients with chronic spondylodiscitis without neurologic deficits. A recent study from the Netherlands included 64 patients with MR imaging findings compatible with spondylodiscitis who underwent CT-guided biopsy.10 Sixty-two patients (96.9%, 62/64) would have been adequately treated if a strategy were followed that would subject all patients with negative blood cultures to empiric antibiotics (i.e., clindamycin for coverage of Gram-positive bacteria) without using biopsy results to determine the optimal antibiotic regimen, provided that there are no clinical findings suspicious for “atypical” microorganisms.10 Refraining from routine biopsy and initiating empiric treatment when blood cultures have negative findings may be considered in patients with a nonacute chronic presentation and typical MR imaging findings of spondylodiscitis10 (ie, T2 hyperintensity and/or contrast enhancement of 2 consecutive vertebrae and the intervening disc after administration of a gadolinium-based contrast agent14). Patients who are immunocompromised and in whom atypical micro-organisms can be expected such as Candida species and patients with clinical and/or MR imaging findings that may suggest tuberculous spondylodiscitis (including relative sparing of the intervertebral disc early in the stage of infection, involvement of the anterior vertebral body corner, subligamentous spread, multiple vertebral body involvement, extensive paraspinal abscess formation, abscess calcification, and vertebral destruction15) should be exempt from this strategy.10
Third, the final aim of a percutaneous image-guided biopsy is to improve patient outcome in terms of quality-adjusted life years gained. A study in 64 patients with suspected spondylodiscitis did not show any significant difference in outcome (defined as either development of severe vertebral height loss, hyperkyphosis, neurologic deficits, or the need for an operation within 6 months after CT-guided biopsy, and/or death during hospitalization) between patients with CT-guided biopsy cultures with positive findings (6/25 patients with poor outcome) and CT-guided biopsy cultures with negative findings (7/39 patients with poor outcome) (P = .751).10 In another study, there were no significant differences in treatment success (defined as survival and absence of signs of infection at the end of the therapy) either between 75 patients with microbiologically confirmed spondylodiscitis (whether by means of blood or biopsy cultures) and 76 patients without microbiologically confirmed spondylodiscitis (P = .157).16 Randomized studies in which the outcome of patients who underwent percutaneous image-guided biopsy were compared with those who did not undergo this procedure are lacking. Therefore, there is currently no evidence that routine percutaneous image-guided biopsy improves outcomes in patients with suspected spondylodiscitis and blood cultures with negative findings.
Proposal of a New Diagnostic Algorithm
On the basis of the previously mentioned underpinnings (key findings of the main studies discussed in this review article are shown in the Table) and our own 9-year single-center experience,10 we have reconsidered the role of percutaneous image-guided biopsy in the diagnostic work-up of patients with suspected spondylodiscitis at our institution. First, we classify patients as either those with (suspicion of) acute spondylodiscitis or chronic spondylodiscitis. Patients with acute spondylodiscitis present with a sudden onset of pain, most often associated with fever and high serum inflammatory markers. Patients with chronic spondylodiscitis have long-standing pain for which the exact time of onset often cannot be determined, fever is frequently absent, and serum inflammatory markers are often only mildly increased. Rather than subjecting all patients with (suspicion of) acute spondylodiscitis to this procedure, only those with blood cultures with negative findings are now eligible for CT-guided biopsy. Biopsy is not performed in patients in whom the results of blood cultures are positive or still unknown within 48 hours. In the group of patients with (suspicion of) chronic spondylodiscitis, biopsy is withheld and empiric treatment with clindamycin is started, provided that the patient is not immunocompromised, no clinical suspicion of a Gram-negative infection is present, and there is no suspicion of tuberculosis or doubt about the diagnosis of spondylodiscitis based on clinical and imaging grounds. If there is no improvement at the end of therapy (ie, 6 weeks after completion of antibiotic therapy), CT-guided biopsy will be performed. We also advise performing percutaneous image-guided biopsy at least 2 weeks after stopping antibiotics to reduce the chance of false-negative cultures.
Key findings of main studies discussed in this article
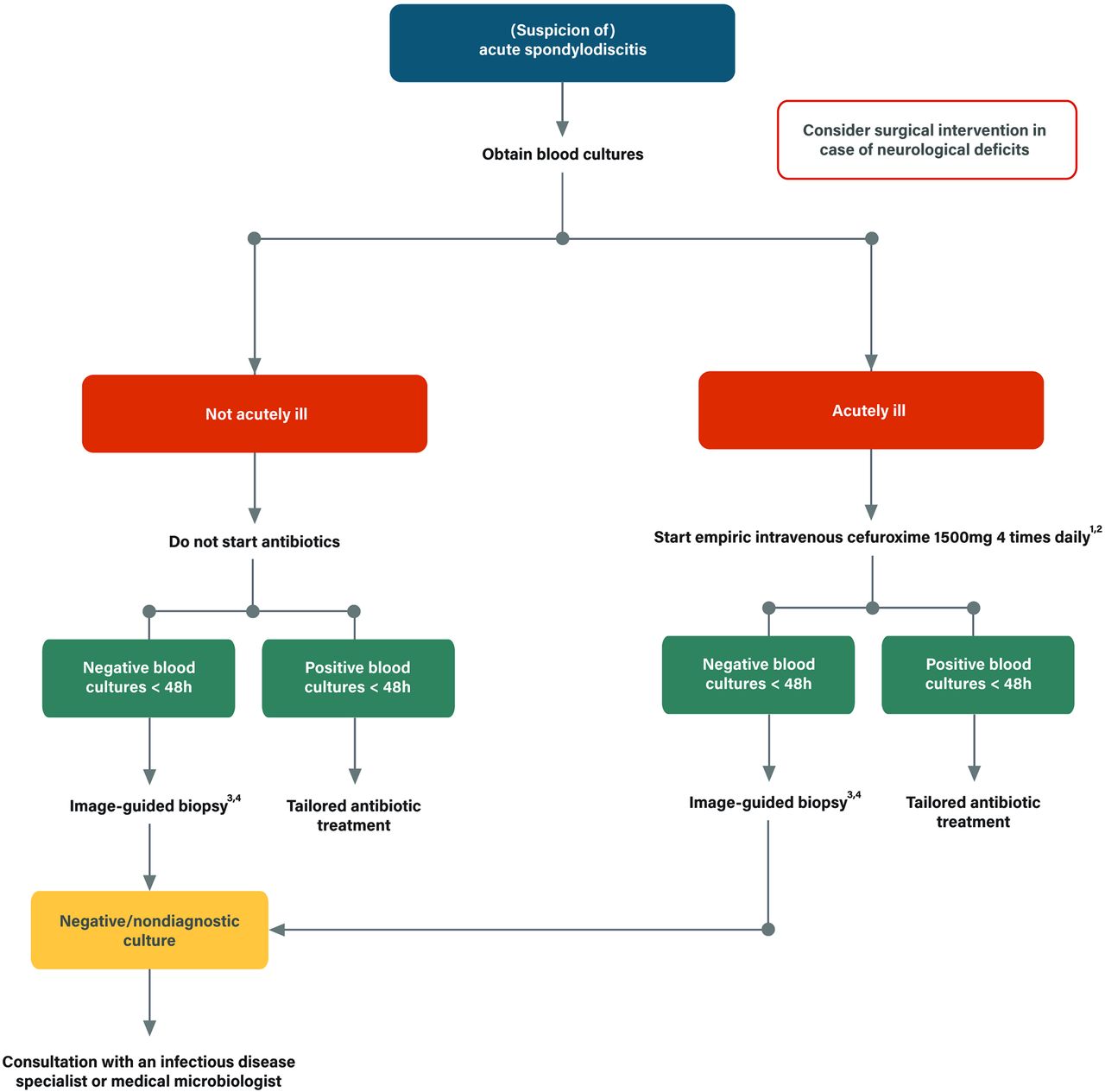
The proposed diagnostic algorithm is shown in Fig 1 (acute spondylodiscitis) and Fig 2 (chronic spondylodiscitis). With this new approach, the number of unnecessary percutaneous image-guided biopsies can potentially be reduced. Our institution is located in a region where the prevalence of both tuberculosis and antibiotic resistance is low. Whether the shift from a routine to a more conditional role of percutaneous image-guided biopsy in spondylodiscitis can be implemented in other institutions is probably dependent on these 2 important conditions. Although the proposed diagnostic algorithm requires clinical validation, it can be considered as an important first step to open the debate on this topic and to initiate research to further refine the role of percutaneous image-guided biopsy in spondylodiscitis.
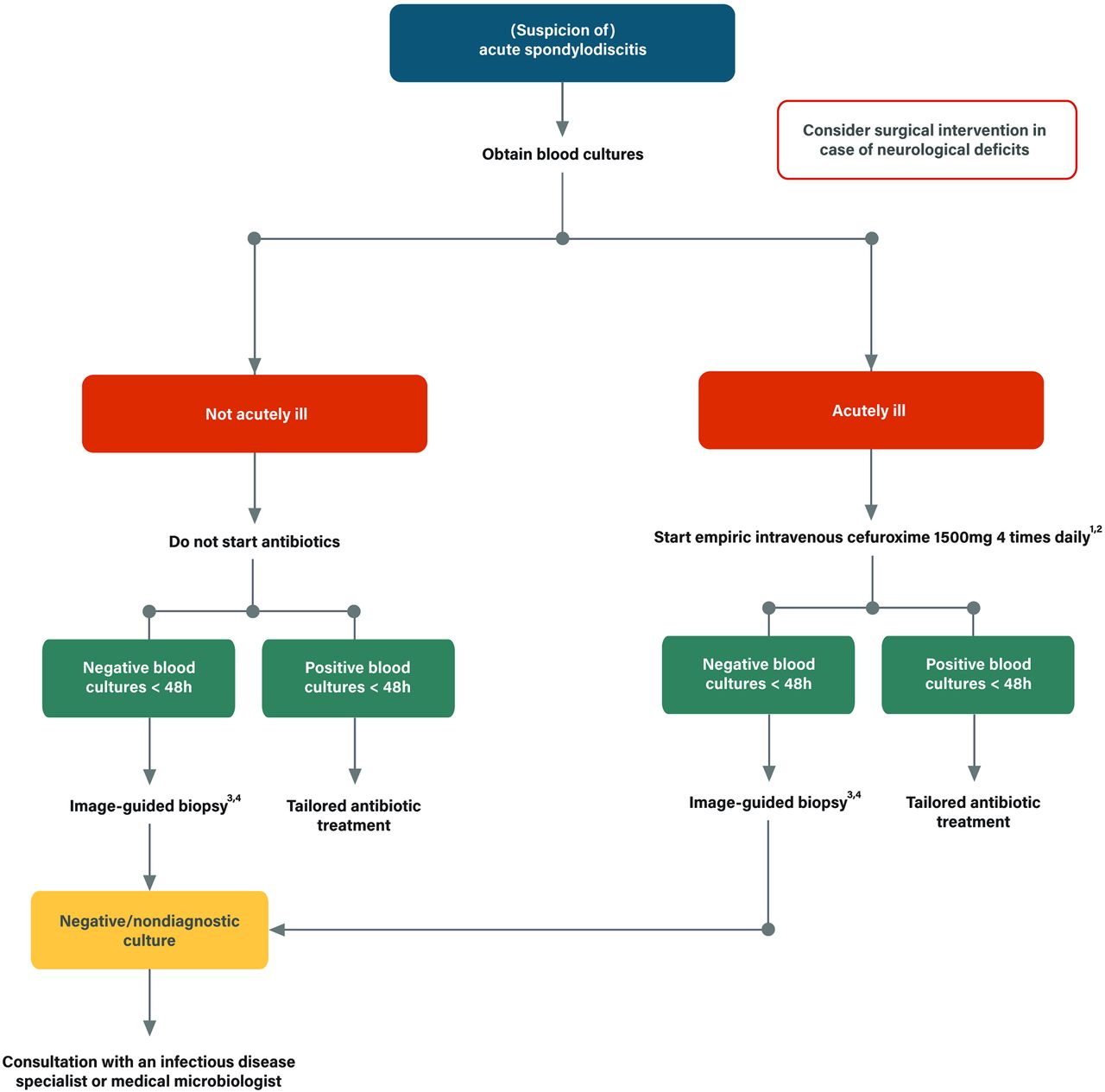
Proposed diagnostic algorithm for (suspected) acute spondylodiscitis. Acute spondylodiscitis is defined as acute pain in back or neck, fever and/or increased C-reactive protein levels, and characteristic imaging findings of spondylodiscitis on MR imaging or FDG-PET/CT (FDG-PET/CT should be considered when MR imaging cannot be performed). Explanation of annotations in this figure: 1) Addition of tobramycin 7 mg/kg once daily in case of sepsis, adjustment according to cultures; 2) Empiric antibiotics should be aimed at both Gram-positive and Gram-negative bacteria, and the most common pathogens of spondylodiscitis, with the final choice based on local antibiotics resistance data (in countries with a high prevalence of methicillin-resistant S. aureus, cefuroxim is not sufficient); 3) If sufficient material can be obtained, then biopsy samples should be sent in for both microbiological and pathological examination; 4) Additional diagnostics for atypical pathogens should be performed when clinically indicated, in consultation with an infectious disease specialist or medical microbiologist.

Proposed diagnostic algorithm for (suspected) chronic spondylodiscitis. Chronic spondylodiscitis is defined as chronic pain (weeks to months) in back or neck, and characteristic imaging findings of spondylodiscitis on MR imaging or FDG-PET/CT (FDG-PET/CT should be considered when MR imaging cannot be performed). Explanation of annotations in this figure: 1) If there is a suspicion of tuberculous spondylodiscitis or doubt about the diagnosis of spondylodiscitis, image-guided biopsy is recommended; 2) If sufficient material can be obtained, then biopsy samples should be sent in for both microbiological and pathological examination; 3) Additional diagnostics for atypical pathogens should be performed when clinically indicated, in consultation with an infectious disease specialist or medical microbiologist.
CONCLUSIONS
Percutaneous image-guided biopsy is a valuable tool in the diagnostic arsenal for spondylodiscitis. However, it is an invasive procedure, and recent evidence has shown rather disappointing positive microbiologic culture yields of around 33%. Recent evidence also has shown that percutaneous image-guided biopsy rarely adds any new information when blood cultures have positive findings and that an effective empiric treatment can be started in the far most of cases even when the microbiologic culprit remains unknown. Finally, there is currently no evidence that percutaneous image-guided biopsy improves patient outcome. On the basis of these underpinnings, it may be time to consider a shift from a routine to a more conditional role of percutaneous image-guided biopsy in spondylodiscitis.
References
- Received October 14, 2020.
- Accepted after revision November 9, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.