
Abstract
BACKGROUND AND PURPOSE: Dandy-Walker malformation, vermian hypoplasia, and Blake pouch remnant represent a continuum of anomalies and are common reasons for referral for fetal MR imaging. This study aimed to determine biometric measurements that quantitatively delineate these 3 posterior fossa phenotypes.
MATERIALS AND METHODS: Our single-center institutional review board approved a retrospective analysis of all fetal MRIs for posterior fossa malformations, including Dandy-Walker malformation, vermian hypoplasia, and Blake pouch remnant. Measurements included the anterior-to-posterior pons, craniocaudal and anterior-to-posterior vermis, lateral ventricle size, and tegmentovermian and posterior fossa angles. Measurements were compared with normal biometry and also between each subgroup.
RESULTS: Thirty-three fetuses met the criteria and were included in the study. Seven were designated as having Dandy-Walker malformation; 16, vermian hypoplasia; and 10, Blake pouch remnant. No significant group interactions with adjusted mean gestational age for tegmentovermian and posterior fossa angles were observed. The tegmentovermian angle was significantly higher in Dandy-Walker malformation (109.5° [SD, 20.2°]) compared with vermian hypoplasia (52.13° [SD, 18.8°]) and Blake pouch remnant (32.1° [SD, 17.9°]), regardless of gestational age. Lateral ventricle sizes were significantly higher in Dandy-Walker malformation at a mean of ≥23.1 weeks’ gestational age compared with vermian hypoplasia and Blake pouch remnant. The anterior-to-posterior and craniocaudal vermes were significantly smaller in Dandy-Walker malformation compared with vermian hypoplasia and Blake pouch remnant at mean of ≥23.1 weeks’ gestational age.
CONCLUSIONS: Dandy-Walker malformation can be described in relation to vermian hypoplasia and Blake pouch remnant by an increased tegmentovermian angle; however, other potential qualifying biometric measurements are more helpful at ≥23.1 weeks’ gestational age. Because they fall along the same spectrum of abnormalities, the difficulty in distinguishing these entities from one another makes precise morphologic and biometric descriptions important.
ABBREVIATIONS:
- AP
- anterior-to-posterior
- BP
- Blake pouch remnant
- CC
- craniocaudal
- DWM
- Dandy-Walker malformation
- GA
- gestational age
- TCD
- transverse cerebellar diameter
- TVA
- tegmentovermian angle
- VH
- vermian hypoplasia
When Walter E. Dandy and A. Earl Walker first described cases of hydrocephalus secondary to congenital obstruction of the foramina of Luschka and Magendie nearly a century ago, they were not referring to a wide spectrum of abnormalities of the posterior fossa ranging from normal vermian size and morphology with no intervention required and normal neurodevelopmental outcomes to in utero obstructive hydrocephalus requiring shunting in the neonatal period, lasting profound neurologic deficits, and underlying genetic disorders. Despite the ongoing inconsistency of this terminology in the literature, the so-called “Dandy-Walker Malformation” (DWM) term persists in clinical practice and is one of the most common reasons for referral for fetal MR imaging.1⇓-3
In the past 20 years, there is greater recognition that Blake pouch remnant (BP), vermian hypoplasia (VH), and classic DWM exist along a continuum of abnormalities resulting from abnormal development of the posterior membranous area during fourth ventricle development.4,5 There is now increased knowledge of normal posterior fossa development and the appearance of the vermis on fetal MR imaging. Thus, evaluation of posterior fossa structures on fetal MR imaging by categorizing these posterior fossa malformations into potentially clinically meaningful groups, including routine measurements, can greatly assist routine clinical practice.6,7 However, there is still a relative paucity of literature describing fetal MR imaging biometric measurements in patients with posterior fossa anomalies along the Dandy-Walker continuum.
In this article, the authors aimed to determine whether posterior fossa biometric measurements on fetal MR imaging can be used to qualify these 3 posterior fossa abnormalities in clinical practice.
MATERIALS AND METHODS
Study Design
This study was a single-center, retrospective review. A list of fetal MRIs performed at Cincinnati Children’s Hospital Medical Center from January 1, 2000, through March 22, 2018, was compiled using Illuminate Insight software (Softek Illuminate, Overland Park, KS) with key words “Dandy-Walker,” “vermian hypoplasia,” and “Blake.” These MRIs were retrospectively reviewed by the study radiologists, and patients who did not clearly have a posterior fossa abnormality along the Dandy-Walker continuum were excluded. Only fetuses with adequate available postnatal clinical follow-up by a neurologist within the institution, with or without postnatal neuroimaging, were included. Determination of diagnostic-quality imaging was made at the neuroradiologists’ discretion. A chart review was performed to obtain relevant clinical data. This study was compliant with the Health Insurance Portability and Accountability Act and approved by the institutional review board. The requirement for informed consent was waived.
Scanning Parameters
All fetuses included in our study were scanned prenatally on a 1.5T magnet at the Cincinnati Children’s Hospital Medical Center using an Ingenia 1.5T (Philips Healthcare) or a Signa HDxt 1.5T (GE Healthcare) system. T2 single-shot FSE images of the brain were obtained in 3 planes: axial, sagittal, and coronal. Three-millimeter section thickness, no-gap interleaved images at 24 weeks’ gestational age (GA) and 4-mm, no-gap interleaved images at 24 weeks were used. Although this imaging protocol did not change during the study period, the TRs and TEs varied between each scanner and were changed at times of scanner upgrades to optimize image quality. At least 2 stacks in each plane were obtained to the radiologist’s satisfaction, including the midline sagittal image required for the biometric measurements in this study. The smallest FOV possible was used. Axial DWI, T1 spoiled gradient recalled, and echo-planar images of the fetal brain were inconsistently implemented at the radiologist’s discretion at the time of imaging before 2016, at which point they became a part of the routine fetal brain malformation protocol.
Image Interpretation
All images were reviewed by 2 board-certified radiologists (U.D.N., B.M.K.-F.), both with added qualifications in pediatric radiology and fellowship training in pediatric neuroradiology, one (B.M.K.-F.) with >15 years of postfellowship attending experience in pediatric neuroradiology in a large academic center, the other (U.D.N.) with >5 years of experience. The images were viewed on a PACS workstation. Only diagnostic-quality MRIs for the assessment of the fetal and postnatal brain were included in our study; image quality was a subjective assessment made by the neuroradiologists.
The radiologists assigned each patient into 1 of 3 categories: classic DWM, VH, or BP. DWM was assigned to fetuses that met 3 imaging criteria: partial or complete absence of the vermis, cystic enlargement of the fourth ventricle, and an enlarged posterior fossa marked by upward displacement of the tentorium and torcular.8 VH was defined as a vermis that was small for GA with an elevated tegmentovermian angle (TVA) (>18°) without posterior fossa enlargement. BP was defined as a vermis that was normal in size for GA; however, the TVA was elevated >18°.7 Differences were resolved by consensus.
Multiple measurements of the posterior fossa were acquired and recorded by the radiologists. These measurements included transverse cerebellar diameter (TCD), vermis craniocaudal (CC) height, anterior-to-posterior (AP) vermis, AP pons, and lateral ventricle size of the largest lateral ventricle. Measurements were acquired using PACS measuring tools and recorded in millimeters, rounding to the nearest millimeter. Methods used to acquire these measurements have been described by Tilea et al.9,10 The TVA and superior posterior fossa angle were measured with values rounded to the nearest degree; the methods are described by Chapman et al.11 The cisterna magna was described as normal or enlarged; this was a subjective assessment by the radiologist because reproducible measurements were not possible, given vermian rotation and distortion. Vermian foliation was described as normal or abnormal. Postnatal brain MRIs, when available, were reviewed in each patient for confirmation of the prenatal diagnosis.
Statistical Analysis
Measurements were compared with normal values published by Kline-Fath et al.12 These data were based on a total of 325 normal fetal brain MRIs 94 of which were between 18 and 22 weeks’ GA. The reference curves for the healthy group were estimated using the methods described by Wan et al,13 with GA as the predictor. The 10th, 50th, and 90th smoothed curves were derived and graphed along with points representing the diagnostic groups. In addition, ANCOVA models were conducted in which a measurement was modeled as a function of the diagnostic group, GA, and their interaction term. To look at diagnostic group differences across time, we compared adjusted means (least square means) to the means at selected GAs for the diagnostic groups being compared. Thus, the mean GA and ages chosen for comparison at the median and lower and upper quartiles examined will depend on whether the healthy cohort is included in that particular model.
All statistical analyses were conducted using SAS statistical software, Version 9.4 (SAS Institute). Comparisons were considered statistically significant with P < .05. No adjustments were made for multiple comparisons.
RESULTS
Description of Cohort
A total of 240 fetal MRIs (108 VH, 90 DWM, and 42 BP) were identified by keyword search. Those without documented postnatal clinical follow-up in the Cincinnati Children’s Hospital medical records were excluded, leaving a total of 48 patients. Images were reviewed by the study radiologists, and 4 additional patients were excluded on the basis of imaging characteristics (prenatal or postnatal) that were consistent with other congenital brain abnormalities (2 Chiari II, 1 Joubert syndrome and related disorders, and 1 aqueductal stenosis). An additional 11 patients with a small vermis and a normal TVA (<18°) were also excluded before analysis, leaving a total of 33 patients. Average maternal age at fetal MR imaging was 29.15 (SD, 6.6) years. Average GA at fetal MR imaging was 24.66 (SD, 4.8) weeks, with 1 patient having a second fetal MR imaging at 32 weeks 3 days’ GA. Ninety-seven percent (32/33) of patients had postnatal brain MR imaging available for review, all confirming the prenatal evaluation of the posterior fossa malformation described. The average age at postnatal brain MR imaging was 49.06 (SD, 93.45) days.
Posterior Fossa Measurements
Of the 33 patients included, 7 were considered to have DWM; 16, VH; and 10, BP (Fig 1). The average measurements in each category, regardless of GA, are summarized in the Table. The vermis could not be seen in 1 patient with DWM so that the vermis height, AP vermis, TVA, and vermian foliation could not be assessed. The cisterna magna was considered enlarged in 100% (7/7) of patients with DWM, which was greater than in the other 2 groups (68.75% [11/16] in VH, 50% [5/10] in BP), though it was not statistically significant (P = .08). Abnormal vermian foliation was observed in a significantly larger portion of the patients with DWM and VH than in those with BP (P = .004).

Examples from cohort of Dandy-Walker continuum with TVAs. Sagittal (A) and axial (D) T2 single-shot FSE images from fetal MR imaging at 30 weeks’ GA demonstrate a BP with elevated TVA at 24°; however, the vermis is normal in size and morphology. Sagittal (B) and axial (E) T2 single-shot FSE images from fetal MR imaging at 32 weeks’ GA with VH. There is a coexisting BP marked by an elevated TVA; however, the tentorium is not considered elevated. Sagittal (C) and axial (F) T2 single-shot FSE images from fetal MR imaging at 24 weeks’ GA with classic DWM. The vermis is very small and rotated, and the tentorium is elevated with upward displacement. There is also separation and flattening of the cerebellar hemispheres (F, arrows).
Average measurements in each category
After adjusting for GA, we made group comparisons from the measurements. The AP vermis, AP pons, and TCD were all significantly affected by the adjusted mean GA (P < .05). The AP vermis, CC vermis, and AP pons were significantly smaller in the DWM group compared with the BP and VH groups at ≥23.1 weeks’ mean GA. No significant differences in the TCD were seen among groups when adjusted for GA. No significant group differences were seen with the AP vermis, CC vermis, AP pons, and TCD at ≤21.1 weeks’ mean GA. The TVA and posterior fossa angles were not significantly affected by the adjusted mean GA. The TVA was significantly higher in patients with DWM than in those with VH and BP, regardless of GA. Lateral ventricle size was significantly affected by the adjusted mean GA (P = .045) and also significantly larger in the DWM group than in the BP and VH groups at ≥23.1 weeks’ mean GA. No significant differences in ventricle size were observed between BP and VH regardless of GA. P values from the ANCOVA by adjusted mean GA are summarized in the Online Supplemental Data. P values from the ANCOVA by GA quartiles are summarized in the Online Supplemental Data.
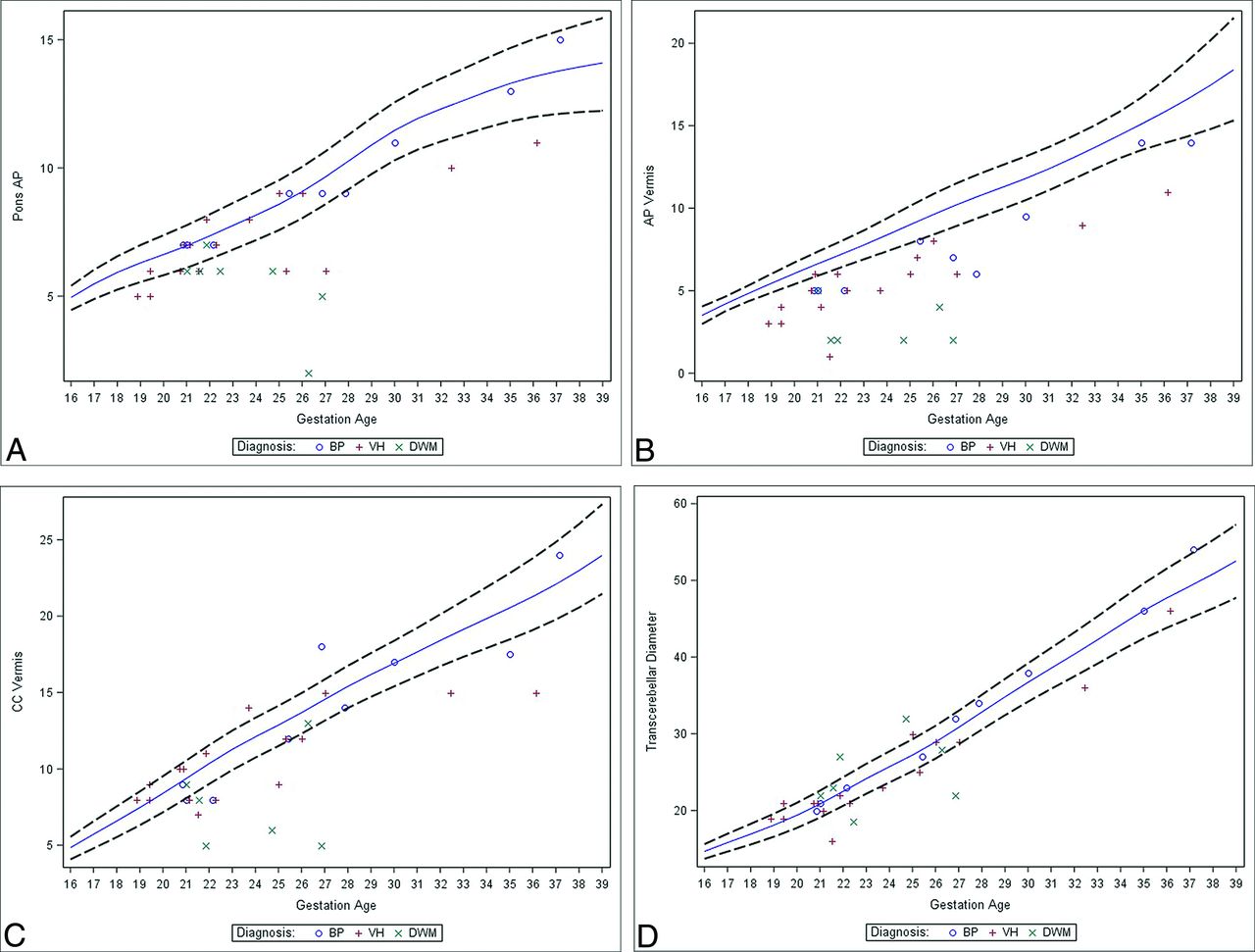
After adjusting for GA, we made comparisons with normal values. AP vermis, CC vermis, AP pons, and TCD all were significantly affected by the adjusted GA (P < .05). The AP vermis was significantly smaller than normal values for BP, DWM, and VH regardless of the GA. The CC vermis was significantly smaller than normal values in patients with DWM and VH at ≥25 weeks’ mean GA. No significant differences among the CC vermis, AP pons, or TCD were noted when BP was compared with normal values, regardless of the GA. Graphs illustrating values compared with normative data are shown in Fig 2. P values from the ANCOVA by adjusted mean GA are summarized in the Online Supplemental Data. P values from the ANCOVA by GA quartiles are summarized in the Online Supplemental Data.

Measurements of the patients included in this cohort for AP pons (A), AP vermis (B), CC vermis (C), and TCD (D) plotted in relation to the normal growth curves by GA.
DISCUSSION
We examined fetal MR imaging findings along the Dandy-Walker continuum to include classic DWM, VH, and BP. We used commonly used metrics in fetal imaging and compared values with normative data. We observed that the AP vermis, CC vermis, AP pons, and TCD were not significantly different among the diagnostic groups at ≤21.1 weeks’ mean GA. We also found that the TVA was significantly larger in DWM than the VH and BP groups regardless of GA, and in our series, it ranged from 79° to 130°. Finally, we observed a decreased AP vermis in all 3 groups compared with data of healthy fetuses regardless of GA and a decreased CC vermis in those with DWM and VH compared with values of normal fetal brains at ≥25 weeks’ mean GA.
The initial descriptions of Dandy-Walker malformation were based on observations made before cross-sectional neuroimaging were widely available and were largely based on intraoperative findings, pathologic specimens, and pneumocephalography.1-3 These observations resulted in the selection of the most severe cases in the pathologic spectrum, and torcular-lambdoid inversion was a description based on the anatomic landmarks that could be reliably identified radiographically. Once CT and MR imaging were routinely used in clinical practice, abnormalities ranging from classic DWM to mega cisterna magna, a normal variant, were described along the same pathologic spectrum, believed to all originate from defects in development of the posterior membranous area.4,5,14
During the past decade, fetal MR imaging has become a crucial part of the evaluation of the brain prenatally and often plays a key role in counseling patients and postnatal management.15⇓-17 Prenatal identification of a posterior fossa anomaly along the Dandy-Walker continuum does not have the same clinical implications as postnatally diagnosed classic DWM, making counseling and perinatal management challenging. Prenatally diagnosed isolated BP, in which the vermis is normal in size with an elevated TVA, generally portends a good prognosis; however, close follow-up is suggested because postnatal obstructive hydrocephalus can develop.18⇓⇓-21 Isolated vermian hypoplasia also can portend a good prognosis.22 However, prenatally diagnosed classic DWM can portend a worse prognosis, with an increased incidence of chromosomal and associated structural anomalies described.23⇓-25
Our study adds to the existing literature by providing posterior fossa biometric measurements on fetal MR imaging in patients with posterior fossa malformations along the Dandy-Walker continuum in a relatively large group of patients with postnatal imaging confirmation of diagnoses and clinical follow-up. While 1 recent large series examined quantitative data of vermian lobulation and brain stem areas in healthy patients and those with Dandy-Walker continuum on fetal MR imaging, a very important area of work, these metrics can be challenging to use in routine clinical practice, depending on the available PACS measuring tools, and may require postprocessing in a separate software package.26 This study, along with other studies describing advanced imaging analysis of volumetric data of the posterior fossa structures, will likely prove valuable in future studies.27 Our study also observed that the TVA can be a helpful descriptive tool in differentiating classic DWM from the other posterior fossa abnormalities along the spectrum of a TVA of ≥80° (range, 79°–130° in our study), regardless of GA. This is valuable information, particularly in the context of descriptions of the clinical outcomes in this patient population based on their grouping. Finally, our study illustrates the limitations of other fetal biometric measures (posterior fossa angle, AP vermis, CC vermis, AP Pons, and TCD) in differentiating these entities along the spectrum at ≤21.1 weeks’ mean GA. Understanding the limitations of fetal brain biometric measurements early in the second trimester is important in counseling and can help guide the appropriate timing of fetal MR imaging in a given patient with a suspected posterior fossa malformation. These limitations may change with continued advances in MR imaging technology, improving spatial resolution in fetal MR imaging along with more detailed robust reference data for clinical use in the future.
Our study has several limitations. First, the retrospective nature of this study limits its internal validity. Second, given that this is a single-institution study performed within a certain timeframe, the external validity may be limited as well. The use of the diagnostic categories in this study may come under scrutiny, given the overlap in imaging findings and the inconsistent use of terminology in the literature. We chose to use an 18° TVA cutoff for BP based on fetal sonography literature by Volpe et al,18 though more recent literature in healthy fetuses on MR imaging described the average TVA as 2.5° (SD, 2.3°).11 This was the case for our review based on the interpretations of fetal MRIs during the study period, though it is possible that patients with smaller BPs may have been inadvertently excluded, particularly given the variation in the existing sonography literature.28⇓-30 Also, because patients included in our VH group had coexisting BP, which explains vermis rotation in VH, there may be some unintended overlap in patients with mild VH and BP, which can be explained, at least in part, by the inherent limitations in the reproducibility in PACS measuring tools.5
We excluded patients with VH in the context of a clear pathologic diagnosis outside the Dandy Walker continuum (Joubert syndrome and related disorders, Chiari II). In addition, we excluded patients with a small vermis that did not have an elevated TVA because these patients may not fall within the same pathologic spectrum of posterior fossa malformations and may be derived from another cause such as an encephaloclastic etiology; however, we realize that there are inherent limitations to this approach as well.31 Also of note, patients with BP have classically been described as having a normal vermis size and morphology; however, 30% (3/10) of patients with BP in our series were described as having abnormal vermian foliation.7 We attribute this to mass effect on the vermis related to the BP rather than a true intrinsic abnormality of the vermis, and because the vermis was normal in size, we kept the current categorization. However, BP can be mistaken for mild VH due to the associated mass effect.6,32
Finally, given the heterogeneity of the terminology used in relation to the Dandy-Walker continuum, the applicability to general clinical practice outside our institution is uncertain at this point. Given the relatively good outcomes reported in BP and isolated VH, some fetal imagers discourage the term “Dandy-Walker variant” because it may give the false impression of a worse prognosis than expected.33 One group of authors described the “tail sign” as a method of differentiating DWM from other posterior fossa malformations; however, this finding has also been seen in other posterior fossa anomalies.34,35 Others advocate that all patients with a small and rotated vermis be considered as having DWM, which serves as an imaging phenotype rather than a primary diagnosis, particularly in the setting of genetic abnormalities. In 1 relatively large study examining large-exome sequencing results, genetic mutations involving 27 different genes were identified and were more frequently encountered in patients with cerebellar hypoplasia (51%) than in those who were classified as having DWM by the authors (16%). This study also reported that many DWMs may be the result of in utero vascular insult, and the severity of imaging findings in the posterior fossa alone has not been reliably shown to correlate with the severity of clinical phenotype.36 Our focus in describing the presence of VH with coexisting BP (elevated TVA) and describing those with a “large” BP as having DWM is a way of approaching this patient population in a systematic fashion. Because the terminology of DWM and Dandy Walker continuum is confusing, it may be more worthwhile to describe this pathology along the spectrum of abnormality related to the enlargement of the Blake pouch, the severity of which is illustrated by the TVA. Severe enlargement would coincide with a TVA of >80°, and milder forms, to >18°. In addition, vermian abnormalities may be best described on the basis of imaging findings of foliation and size.
Despite being one of the largest fetal MR imaging programs in the country, the relatively small number of patients in our cohort, particularly when analyzing subgroups, limits its generalizability. We also chose not to include patients without postnatal follow-up, to help elucidate the clinical implications of the prenatal imaging findings, the value of which will be more evident in future work. In addition, imaging descriptions alone do have inherent limitations, and evaluation of the postnatal clinical outcomes in this patient population, and ultimately large multicenter data collection and analysis, will be necessary to understand the true value of prenatal imaging in this patient population.
CONCLUSIONS
We describe fetal MR imaging findings in patients with posterior fossa anomalies focused on the presence or absence of VH with coexisting BP, also known as the Dandy-Walker continuum. We observed that the TVA can be helpful in the description of classic DWM when distinguishing it from VH and BP, with a TVA ≥80°. We also observed that other posterior fossa measurements, including posterior fossa angles, AP vermis, CC vermis, AP pons, and TCD are not significantly different among fetuses at ≤21.1 weeks’ mean GA in our cohort, which may affect the timing of fetal MR imaging scheduling in this patient population. Given the challenges and inherent limitations in assigning a particular category to these patients and considering the heterogeneity of terminology in the current literature, precise morphologic descriptions and biometric measurements have become increasingly important in prenatal evaluation and, ultimately with future studies, counseling and perinatal management of this patient population.
Footnotes
Disclosures: Usha D. Nagaraj—UNRELATED: Royalties: Elsevier, Comments: I write book chapters on topics in pediatric neuroradiology for Elsevier.
References
- Received January 22, 2021.
- Accepted after revision April 19, 2021.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}