Abstract
Summary: We report an unusual case of granulocytic sarcoma involving the temporal bone. The occurrence of this tumor usually heralds acute myelogenous leukemia or the onset of the blastic phase of chronic myelogenous leukemia. Recognition of this rare entity is important, because early aggressive chemotherapy can cause regression of the tumor, as in our case, and thus improve patient longevity.
Granulocytic sarcoma is a rare extramedullary collection of immature cells with myelogenous differentiation. This tumor was first described in 1811 (1), but its association with leukemia was not recognized until 1893 (2). It occurs most commonly in bone, periosteum, soft tissue, lymph nodes, and skin, although it can occur anywhere throughout the body (3). When located in bone, leukemic cells are thought to originate in the bone marrow and travel via haversian systems to collect in the subperiosteum (4, 5). Symptoms are secondary to the mass effect of the tumor. Granulocytic sarcomas occur most frequently in the pediatric population and in 3% to 5% of all patients with acute myelogenous leukemia, without sex predilection (6). The discovery of this tumor may represent the first sign of acute myelogenous leukemia or relapse in cases of acute myelogenous leukemia or may herald the onset of the blastic phase of chronic myelogenous leukemia (6, 7). Although no standard treatment protocol has been established, early aggressive chemotherapy may represent the best chance for remission. However, the long-term prognosis for these patients remains poor.
Case Report
A 30-year-old Caucasian man with a history of acute myelogenous leukemia (subtype M2 with an 8:21 translocation) that was in remission presented to an otolaryngologist with an acute left-sided facial palsy and postauricular pain. The patient denied any recent trauma or upper respiratory tract infections. He denied history of facial palsy, hearing loss, or vertigo and felt otherwise healthy. An examination revealed a mild left-sided facial paresis with complete eye closure and movement of the angle of the mouth (House-Brackmann grade II). The results of an otoscopic examination of the left ear were grossly normal, and the ossicles were well visualized. The external auditory canal had no erosions, and no mastoid tenderness was present. MR imaging performed 1 week later (Fig 1) showed a well-defined mass extending along the upper anterior left petrous apex. This mass was isointense to brain parenchyma on the T1-weighted images and hyperintense on the T2-weighted images. On T1-weighted fat-suppressed contrast-enhanced images, nearly homogeneous enhancement of the lesion was noted. Contiguous enhancement was seen anteriorly toward the cavernous sinus and posteriorly to the region of the geniculate ganglion, with associated enhancement of the tympanic and mastoid segments of the left facial nerve. A course of orally administered steroids was begun, and within 1 week, complete resolution of the facial weakness and postauricular pain was achieved.
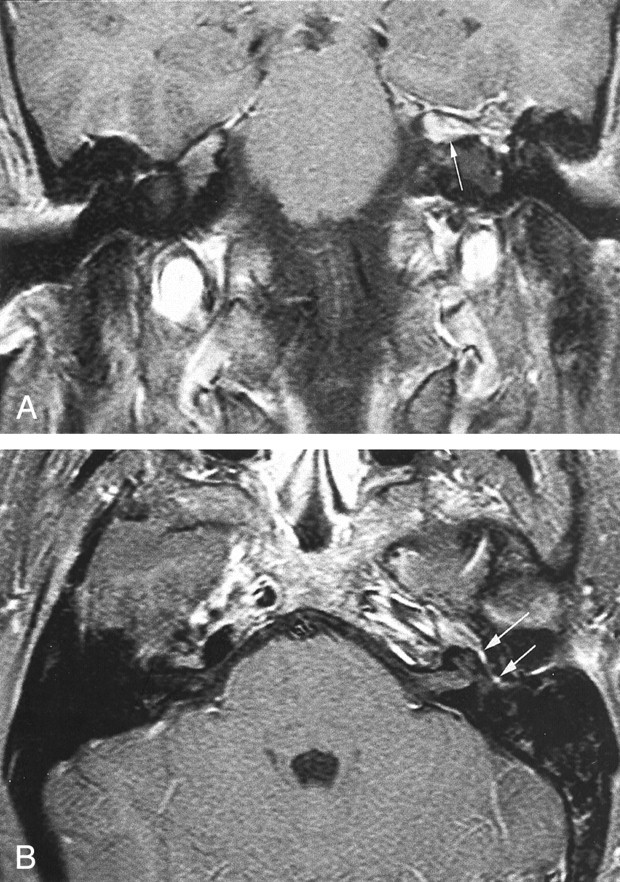
Initial MR images (600/10 [TR/TE]) obtained at presentation.
A, Contrast-enhanced fat-suppressed coronal T1-weighted image shows focal area of enhancement along the anterosuperior surface of the left petrous pyramid (arrow).
B, Contrast-enhanced fat-suppressed axial T1-weighted image shows enhancement along the anterosuperior surface of the left petrous pyramid with extension into the geniculate ganglion (long arrow) and the tympanic segment (short arrow) of the left facial nerve. On an adjacent image (not shown), the mass extended into the posterior left cavernous sinus.
Two months later, the patient had recurrent severe left-sided otalgia, with hearing loss. An otoscopic examination performed at that time was significant for mass in the external auditory canal, and biopsies were obtained. CT of the head revealed a well-defined 2-cm enhancing nodule along the superior surface of the petrous pyramid (Fig 2), which was not noted on the previously obtained MR images. The lesion extended into the left middle ear cavity and the external auditory canal. Biopsy showed granulocytic sarcoma.
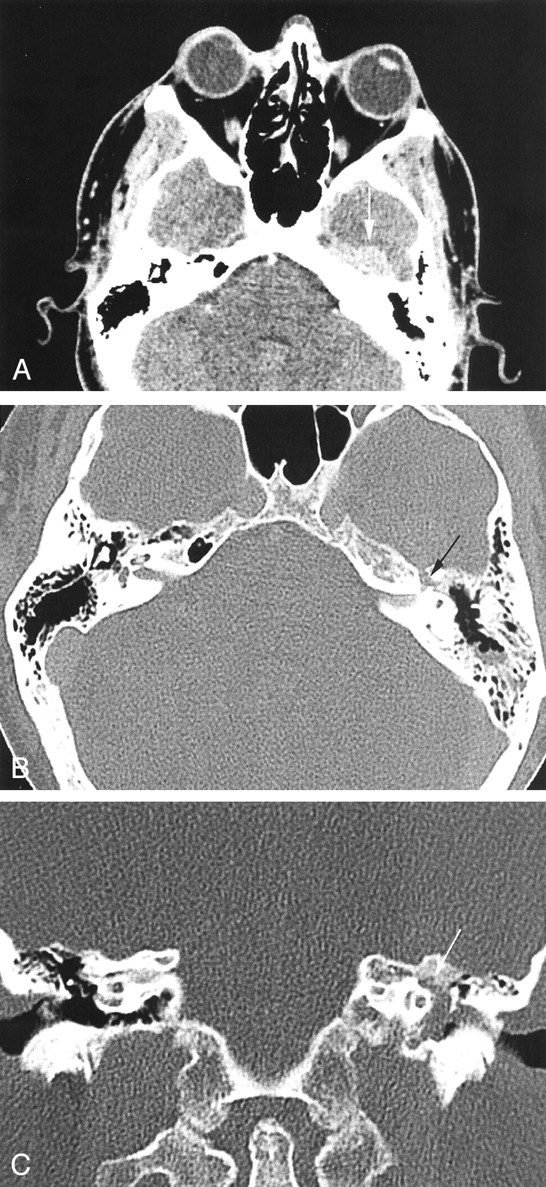
CT scans obtained 2 months later.
A, Contrast-enhanced axial CT scan shows a well-defined approximately 2-cm mass (arrow) along the anterosuperior aspect of the left petrous pyramid. Anteriorly, it is in continuity with the cavernous sinus.
B, High-spatial-resolution axial CT scan (bone window) shows widening of the left facial nerve canal in the region of the geniculate ganglion (arrow). Opacification of the mastoid air cells by serous fluid is also noted, probably secondary to blockage of the eustachian tube by the petrous apex mass.
C, Coronal CT scan, obtained at the level of the cochlea, shows extension of the soft tissue mass into the left middle ear cavity. Erosion of the facial nerve canal at the geniculate ganglion (arrow) is seen.
A bone marrow aspirate was obtained and showed relapsed acute myelogenous leukemia. Cytogenetics revealed a recurrence of the 8:21 translocation. The patient received high dose Ara C chemotherapy and entered into bone marrow remission. Repeat CT performed 1 month later (Fig 3) showed virtually complete resolution of the previously identified enhancing soft-tissue mass. Persistent widening of the facial canal was noted in the region of the geniculate ganglion and was thought to be secondary to previous disease. No new areas of bone erosion were identified.

{kind=link}
{kind=link}
{kind=link}
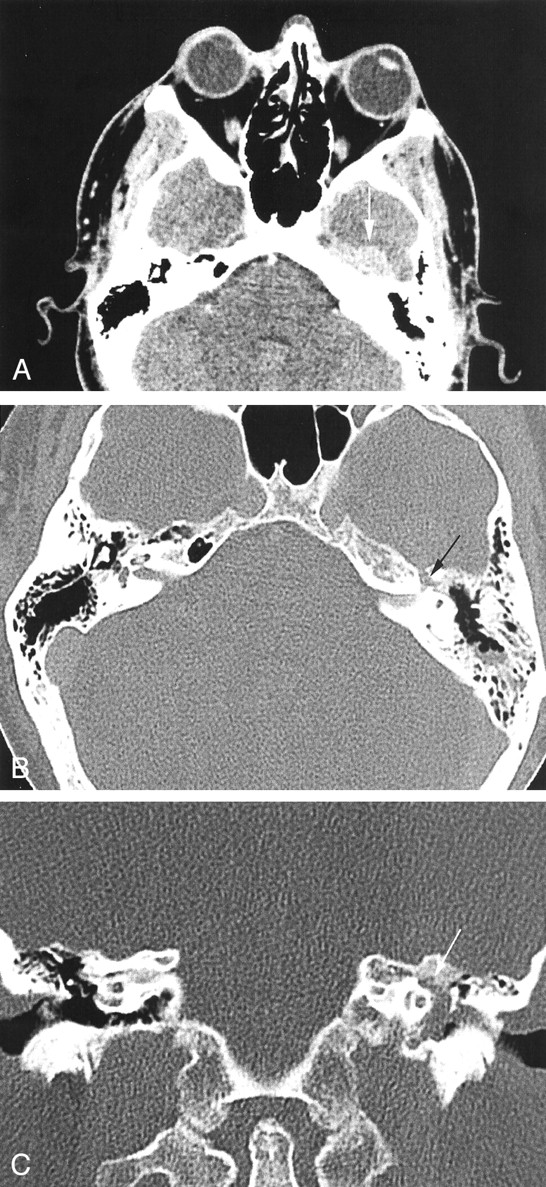
CT scans obtained after chemotherapy and resolution of symptoms.
A, Axial CT scan shows resolution of mass, previously noted along the anterosuperior aspect of the left petrous pyramid.
B, Axial CT scan (bone window), obtained at the level of the cochlea, shows no mass within the middle ear cavity and clear mastoid air cells. The anterior portion of the left carotid canal is faintly seen, and this could represent a residual (erosive) change from the previously noted mass.
Discussion
Granulocytic sarcoma is a rare extramedullary collection of granulocytic cells, also known as chloroma. The tumor was given this colorful name because of its greenish hue secondary to the presence of intracellular myeloperoxidase. However, as reported elsewhere, this phenomenon is variably seen and the proper name for the tumor should remain granulocytic sarcoma (3, 7). This unusual clustering of immature myelocytes has been observed among patients with or without history of leukemia. It is found in 3% to 8% of all patients with acute myelogenous leukemia and is most frequently associated with acute myelogenous leukemia, particularly with subtypes M2, but has also been described in association with other myeloproliferative diseases, such as chronic myelogenous leukemia, polycythemia vera, hypereosinophilia, and myeloid metaplasia (3, 5). In those patients with history of leukemia, the discovery of a granulocytic sarcoma heralds an imminent downturn in clinical course. This aggregation of cells may be the first sign of relapse after bone marrow transplant or may be a signal of the progression of disease from chronic myelogenous leukemia to blastic crisis. In patients without a history of myeloproliferative disorders, granulocytic sarcoma is usually an ominous sign. Most cases proceed to overt leukemia within 2 to 4 years (3, 7). However, uncommonly, cases without progression have also been described.
Recognition of granulocytic sarcoma is important, because aggressive induction chemotherapy or radiation therapy can induce complete remission. When granulocytic sarcomas are clinically symptomatic, the skeleton is the usual site affected. A propensity for ligamentous or periosteal involvement exists, and a predilection for the orbit and epidural spaces has been described in cases of CNS and skull involvement (8). On CT scans, a well-defined area of increased attenuation with a peripheral zone of enhancement mimicking meningioma or lymphoma has been described (9). When the bone is affected, granulocytic sarcoma lesions appear lytic rather than sclerotic (5, 10). On MR images, granulocytic sarcomas have signal intensities similar to those of marrow on T1- and T2-weighted sequences, and they enhance after the administration of contrast material (11). It is, however, not possible to distinguish granulocytic sarcoma from lymphoma, meningioma, or pseudotumor solely on the basis of imaging findings (12). Although the pathologist remains the final arbiter, the clinical findings often suggest the diagnosis of granulocytic sarcoma.
In the head and neck, granulocytic sarcoma has been reported to occur in the maxilla, soft palate, nasopharynx, lip, salivary glands, mandible, and temporal bone (13). Although leukemic infiltration into the middle and inner ears was found to occur in 20% of patients with leukemia, frank granulocytic sarcoma of the temporal bone is rare (14, 15). As in our case, these patients often complain of postauricular pain or fullness and a constellation of symptoms resembling acute otomastoiditis (16). Acute facial nerve palsy is uncommon. There is no role for surgery beyond biopsy, except possibly for the placement of a myringotomy tube if eustachian tube function is compromised. Aggressive treatment of facial palsy with surgical decompression does not seem to be indicated. Our case supports the recent literature that suggests that early, aggressive induction chemotherapy may prolong survival or lead to complete remission (3, 17). The mean survival time has been reported to be from 2.5 to 22 months (3, 6, 17, 18).
Conclusion
Granulocytic sarcoma affecting the facial and cochlear-vestibular nerves can occur in patients with hematogenous disorders. These patients may complain of decreased hearing, otalgia, or facial nerve weakness, and these symptoms may be the first manifestations of recurrent disease. A high level of suspicion is necessary, because early, accurate diagnosis is important to avoid delaying appropriate chemotherapy.
References
- Received March 7, 2002.
- Accepted after revision May 30, 2002.
- Copyright © American Society of Neuroradiology