Abstract
Summary: Transalar encephaloceles are rare lesions that do not fit the standard classification of basal encephaloceles. Typically, these lesions present in adulthood, with nonspecific symptoms. We report here a case of a patient with Wegener disease in whom a large transalar encephalocele posterior to the sinus was noted when he was preoperative for left maxillary sinus surgery. The encephalocele demonstrated irregular peripheral enhancement along the margin—a very uncommon finding—as well as contrast enhancement of the basal meninges, which can be seen occasionally with Wegener granulomatosis.
Sphenoid basal cephaloceles can be classified as either intrasphenoidal (usually herniation of brain and meninges into the sphenoid sinus) or, rarely, transsphenoidal (through the sphenoid, usually greater wing). The transalar variant is even rarer and does not entirely fit the typical basal cephalocele classification. Few cases of transalar basal cephaloceles have been described in the literature and can be variably associated with symptomatology, but they are more likely to present at a later age relative to the other basal cephaloceles. We report the case of a large transalar sphenoidal encephalocele, with presumed simultaneous involvement by Wegener granulomatosis in the basal meninges of the encephalocele and in the adjacent sphenoid sinus.
Case Report
A 46-year-old man, known to have Wegener granulomatosis, presented with a history of chronic left-sided drainage of thickened and foul-smelling secretions. A maxillofacial CT was obtained, which showed a diffusely opacified left maxillary sinus as well as debris within the inferior left frontal sinus and ethmoid air cells and diffuse thickening of the nasal mucosa. There was no significant fluid or debris noted in the left sphenoid sinus. An approximately 3.2-cm defect of the greater sphenoid wing was seen, with dehiscence or minimal bony wall present of the posterolateral wall of the left sphenoid sinus. The skull base defect was centered in the expected location of the left foramen ovale. There was no definite erosion of the bony posterior wall of the maxillary sinus. The foramen spinosum and foramen rotundum were intact. On the basis of CT findings, a congenital defect versus a skull base mass was suspected, and MR imaging was ordered by the otolaryngologist for further evaluation, particularly because a mass in this location could have had preoperative importance.
Subsequent MR imaging of the skull base demonstrated a transalar cephalocele protruding approximately 2.5 cm inferiorly through the left greater sphenoid defect. This cephalocele was bounded superiorly and posteriorly by the carotid canal and inferiorly by the pharyngeal recess and anteriorly by the left maxillary sinus. The cephalocele contained meninges as well as brain tissue. There was associated widening of the left temporal horn and the inferior temporal sulcus, with protrusion of a portion of the inferior aspect of the left temporal lobe through the sphenoid defect. On postcontrast images, there was irregular peripheral enhancement of the meningoencephalocele along its margins (Fig 1). Contrast enhancement along the pachymeninges of the posterior fossa on the right was also noted. The patient subsequently underwent successful endoscopic ethmoidectomy and middle meatal antrostomy.
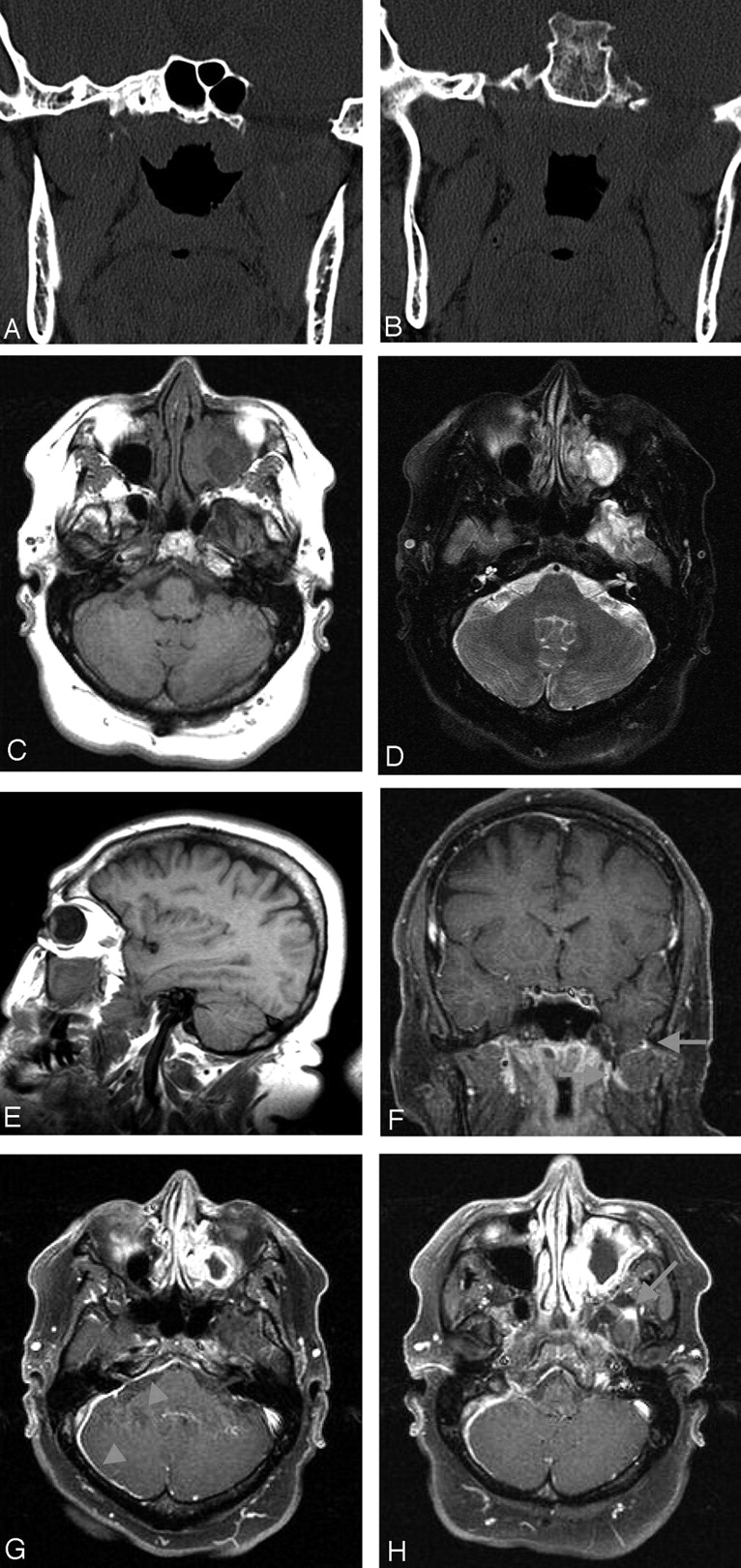
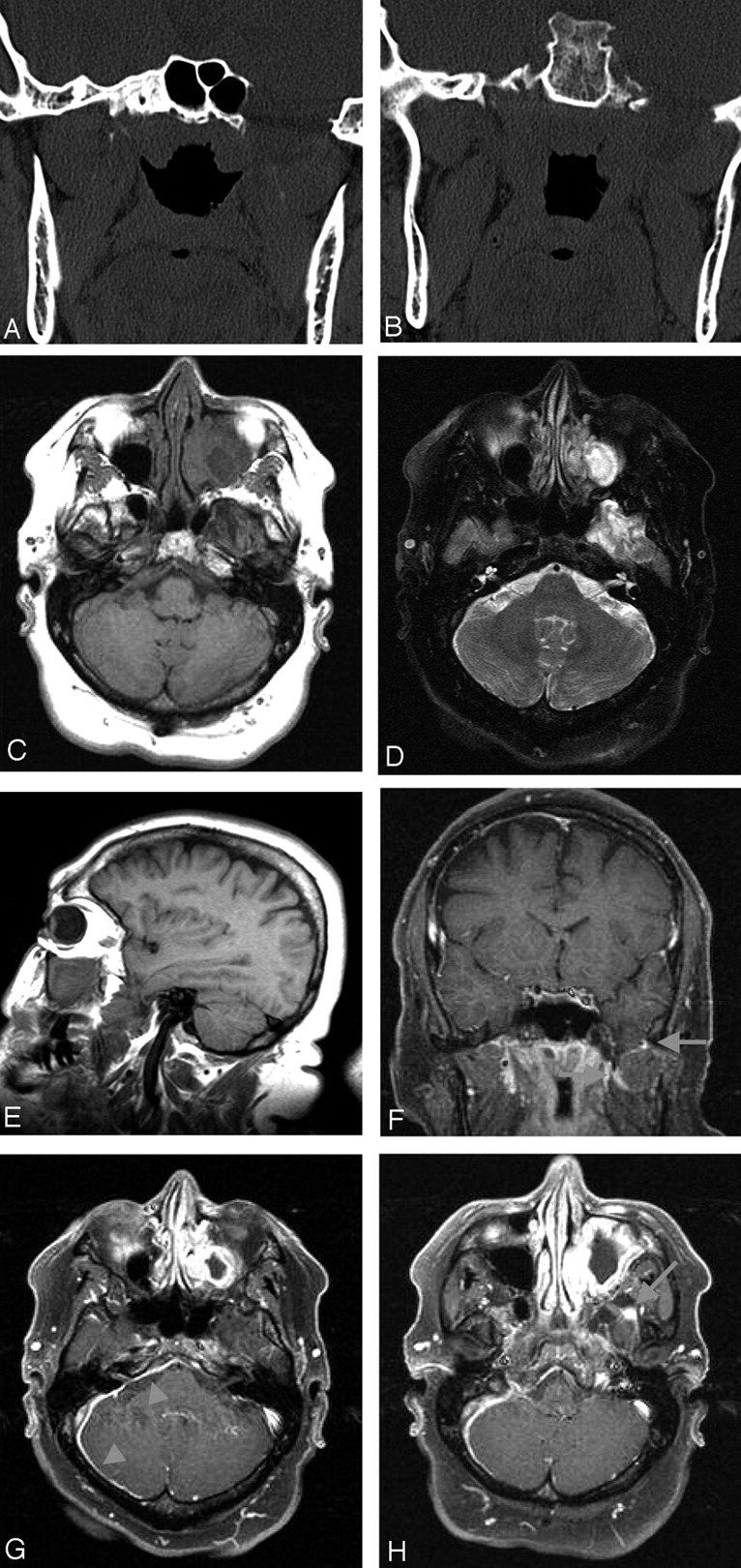{kind=link}
Coronal CT images (A and B) disclose the large bony defect encompassing the region of the foramen ovale and most of the left greater sphenoid wing. Axial T1- and T2-weighted images at the level of the internal auditory canal (C and D) demonstrate the transalar encephalocele presenting prolonged T1 and T2 signals and a heterogeneous lesion centered on the left maxillary antrum presumably related to the known history of Wegener granulomatosis. Sagittal T1-weighted image (E) better shows the left temporal lobe tip insinuating through the bony defect into the masticatory space. Coronal T1-weighted contrast-enhanced image with fat saturation (F) demonstrates again the encephalocele and irregular foci of contrast enhancement along the peripheral portion of the encephalocele (arrows). Axial T1-weighted contrast-enhanced images with fat saturation (G and H) show intense enhancement of the mucosa of the inspissated and inflamed left maxillary sinus. There is also linear dural thickening and enhancement of the dura within the posterior fossa along the medial aspect of the right temporal and occipital bones extending posterior to the clivus (arrowheads), possibly also related to Wegener granulomatosis. A focus of enhancement in the anterior and inferior portion of the encephalocele is again appreciated (arrow).
Discussion
Basal encephaloceles are rare, with an estimated incidence of 1/40,000. They have traditionally been divided into 5 types (1): (1) sphenopharyngeal, (2) spheno-orbital, (3) sphenoethmoidal, (4) transethmoidal, and (5) sphenomaxillary. Regarding the sphenopharyngeal type, the encephalocele protrudes through the floor of the sella. This category includes both the transphenoidal, in which there is protrusion of the cephalocele through the sphenoid sinus into the epipharynx, and the intrasphenoidal type, in which the cephalocele protrudes into the sphenoid sinus. The spheno-orbital cephalocele protrudes through the superior orbital fissure into the posterior orbit. The sphenoethmoidal variant protrudes through the sphenoid and ethmoid bones into the posterior nasal cavity. The transethmoidal cephalocele protrudes through the cribriform plate into the anterior nasal cavity or ethmoid sinuses. A sphenomaxillary cephalocele protrudes through the inferior orbital fissure into the pterygopalatine fossa. These encephaloceles may become progressively less clinically prominent because they occur more posteriorly, and surgical treatment of the more posteriorly located basal encephaloceles has generally been discouraged, particularly for those that may contain hypothalamus, pituitary, or optic nerve/chiasm (2).
The transalar basal encephalocele, which does not quite fit into the above classification, is rare, with only 5 previously reported cases (3–7). This is a lesion in which there is protrusion of an encephalocele directly through the greater wing of the sphenoid bone. In 4 of the previously reported cases, patients presented as adults, usually with nonspecific symptoms (trigeminal neuralgia and angioma of the soft palate [4, 5], headaches and worsening speech and ambulation [6], partial seizures [3], and headaches [3]). The fifth patient presented as an infant with respiratory distress (7).
The sphenoid bone consists of 4 major components: the alisphenoid, which forms the greater wings; the orbitosphenoid, which forms the lesser wings and part of the anterior clinoids; the presphenoid, which will become pneumatized to form the sphenoid sinuses; and the basisphenoid, which will form the posterior sphenoid and sella turcica as well as portions of the anterior clinoids (8–11) The greater wing is composed of both membranous and cartilaginous bone, with the anterior and medial roots being of cartilaginous origin and the remainder composed of membranous bone. The lesion reported here, as in all 5 of the previous cases, is considered to arise within the membranous portion of the alisphenoid.
Etiology of the transalar encephalocele is uncertain, and it is most likely that cephaloceles can be the end result of several developmental disorders (12). There are several theories concerning the development of encephaloceles in general, which are reviewed in Pollock et al (1); some of these are plausible etiologies for the formation of transalar encephaloceles. Failure of separation of ectodermal elements during closure of the neural tube, or failure of closure of the anterior neuropore, may prevent the appropriate migration of mesodermal elements. A primary ossification defect may occur, either singly or as part of a generalized syndrome. Alternatively, an increase in intraventicular pressure during development may extrude developing brain through patent embryologic openings.
This case is important because of the relatively large size of the encephalocele and the concern of the surgeon for a potential skull base mass in this location. Also, the presence of this encephalocele and the particular location were of particular significance, because this patient was known to have Wegener granulomatosis and was preoperative for left maxillary sinus surgery because of the advanced sinus involvement. The inferior portion of the encephalocele (within the pterygopalatine fossa) was posterior to the sinus, and this information was required by the surgeon. Also, the lateral edge of the encephalocele was noted to abut the lateral wall of the sphenoid sinus with erosion or poor development of the bony sinus wall, which also could have been potentially significant preoperative knowledge.
The clinical significance of distinguishing encephaloceles passing through the sphenoid ala is that these patients may present with nonspecific symptoms (3) or can be apparently relatively asymptomatic as demonstrated in our case. This is in contradistinction to the other forms of basal cephaloceles, which are usually more symptomatic at an earlier age, particularly in the anterior forms (2).
Furthermore, there was noted to be moderate irregular contrast enhancement of the margin of the encephalocele posterior to the sinus, which is of uncertain significance. There are reports of intrasphenoid encephaloceles associated with peripheral and central enhancement after the intravenous use of gadolinium. This finding could be related to the chronic inflammatory changes evident on histopathology of these cases (13).
Another possible explanation for the contrast enhancement of the cephalocele observed in this case could be related to the patient’s known associated illness of Wegener granulomatosis, which may involve the brain and meninges, although this is relatively uncommon. When present, this involvement more frequently is associated with meningeal thickening and enhancement and is observed either in the dura or in the leptomeninges (14). This is a plausible explanation in this case because the basal meninges were also noted to have abnormal contrast enhancement, which was thought to be related to Wegener inflammation.
Conclusion
Although an extremely rare congenital lesion, a transalar basal cephalocele should be familiar to the radiologist as the possibility of coexistence with other illnesses exists, as pointed out by the present case. Failure to recognize this entity can have serious implications in management of a patient, particularly if this very uncommon location for a cephalocele is not recognized and mistaken for a mass.
References
- Received July 31, 2004.
- Accepted after revision September 24, 2004.
- Copyright © American Society of Neuroradiology