Abstract
SUMMARY: The association between the formation of intracranial aneurysms and situations of increased blood flow in certain areas of the brain is well accepted today. It has been seen in association with arteriovenous malformations of the brain, carotid occlusion, and Moyamoya disease. The occurrence of aneurysms in small arteries of the skull base, with the exception of the intracavernous carotid artery, however, is rare. We report a case of a 55-year-old woman who presented with an intracerebral hemorrhage caused by a ruptured anterior ethmoidal artery aneurysm. To the best of our knowledge, this is only the second case of documented intracranial bleeding from such a lesion.
This patient, a 55-year-old woman, was transferred to our hospital after a diagnosis of a brain hemorrhage at an outside emergency department. She was alert, obeyed commands, and complained of a strong headache. A slight left hemiparesis was noted as a sequela of a stroke 8 years earlier. At that time, she was diagnosed as having a complete occlusion of the right internal carotid artery in the neck and was treated with antiplatelets. There was no history of any other medical problems. A CT scan of the head showed a right frontobasal hemorrhage, in the region of the gyrus rectus, extending from the anterior cranial fossa (Fig. 1). MR imaging/MR angiogram showed a circular lesion in the anterior skull base, which suggested an aneurysm, but with no relationship with the arteries of the circle of Willis (Fig. 2). An angiogram was then performed, and the diagnosis of an intracranial aneurysm arising from the anterior ethmoidal artery was confirmed, as was occlusion of the right carotid artery. The small lesion had the appearance of a mycotic aneurysm—rounded, with no defined neck, located in a vessel unrelated to the circle of Willis, and large in relation to the parent artery. The right hemisphere was supplied from the contralateral carotid artery through the anterior communicating artery and from the posterior circulation through the posterior communicating artery. Deep collaterals as with Moyamoya disease were present in the right hemisphere (Fig. 3). An orbital “blush” was seen after injection of the right external carotid artery, and, because there was no filling of the ophthalmic artery in the right side, endovascular occlusion was considered unsafe on the basis of our suspicion that the blood supply to the right eye depended on the same artery whose proximal branch fed the aneurysm.

CT showing the hemorrhage in the right gyrus rectus.

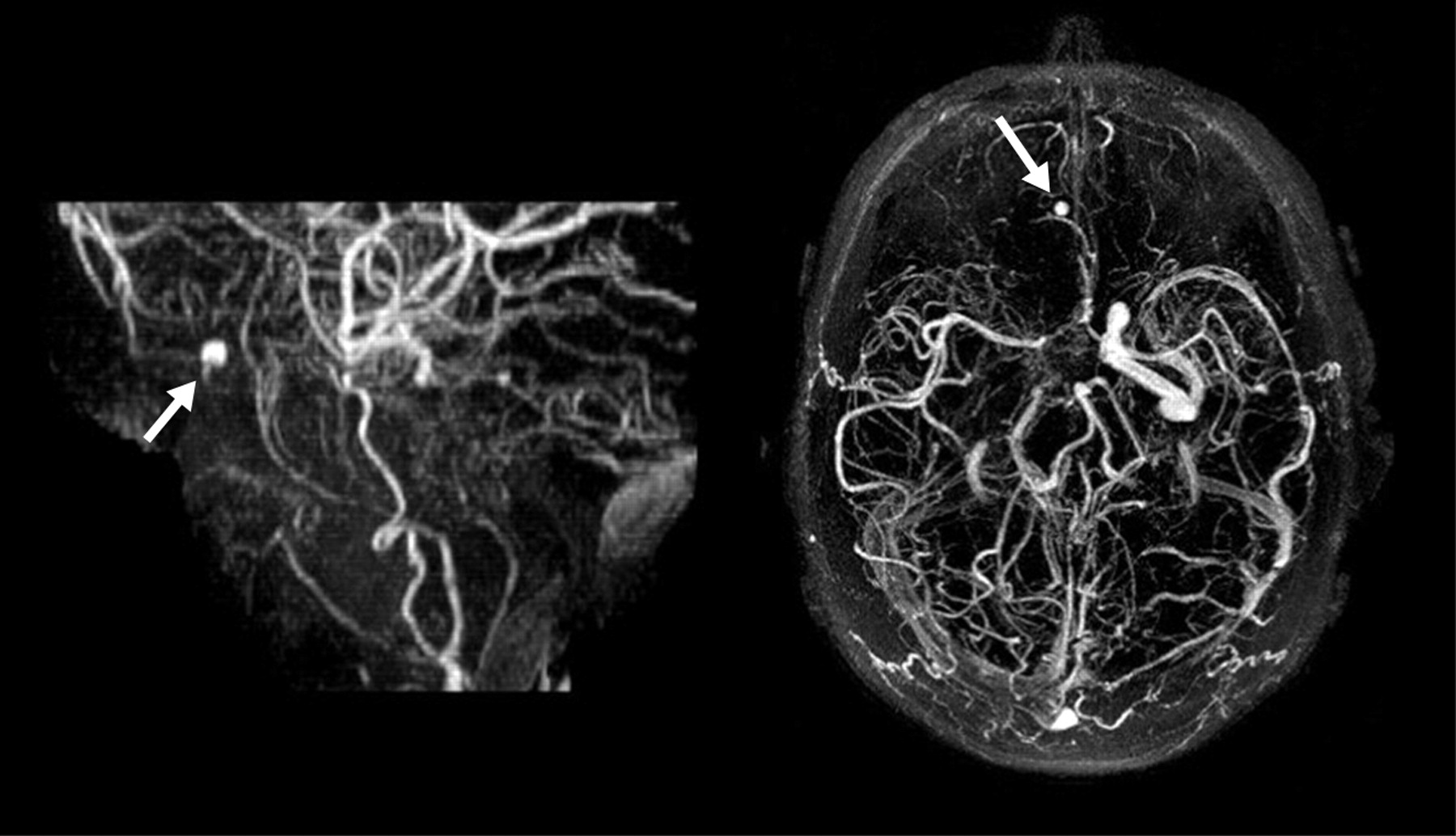
AngioMRI showing the occluded right internal carotid artery and the presence of an aneurysmal dilation in the anterior cranial fossa (arrows).

Left intracranial carotid artery angiogram, showing the contralateral blood supply to the right hemisphere, and the deep collaterals supplying the right hemisphere (A) and left vertebral angiogram showing the contribution of the posterior circulation to the blood supply in the supratentorial circulation (B).
Because of the small size of the vessel, the likelihood of both branches being occluded during the endovascular treatment was considered high. A frontotemporal craniotomy was performed, and the aneurysm was found in close relation to the anterior skull base and the hematoma. There was no defined neck, and proximal control was not possible because the proximal parent vessel was below the aneurysm, surrounded by bone. There was no surgical means to occlude the aneurysm and preserve the anterior ethmoidal artery branch that continued toward the inferior aspect of the right frontal lobe, which was then coagulated just after the aneurysm. The aneurysm was then excised and its parent artery coagulated in its foramina at the anterior cranial fossa bone. The patient recovered well from the procedure and was discharged with no additional deficits. A postoperative angiogram confirmed the exclusion of the aneurysm (Fig. 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Preoperative angiogram showing the small aneurysmal dilation related to a branch of the right anterior ethmoidal artery. The aneurysm is much bigger than the parent vessel, making it difficult to define the neck size. After the removal of the aneurysm the very small branch proceeded to the inferior aspect of the frontal lobe, as also seen during the surgery (A). Postoperative angiogram of the right external carotid artery showing the exclusion of the aneurysm (arrow). Preservation of the parent branch was not possible, because of its small size in relation with the aneurysm, but the branch of the anterior ethmoidal artery thought to be responsible for some supply to the right eye was preserved (arrowhead, B).
Discussion
Saccular aneurysms associated with situations of increased regional cerebral blood flow are well described in the literature. Their presence is reported in patients with Moyamoya disease, carotid artery occlusion, and arteriovenous malformations of the brain. The most accepted theory is that these lesions are formed by an increased stress in the wall related to the high flow imposed by either occlusive disease in the contralateral circulation or an anomalous arteriovenous shunt. Aneurysms located in the arteries of the anterior skull base, however, are extremely rare. We are aware of 5 reported cases, one associated with cerebrovascular occlusive disease,1 another with an abnormal connection between the fronto-orbital artery and the anterior ethmoidal artery,2 one with an anterior fossa meningioma,3 and 2 cases with apparently no associated abnormalities.4,5
Our patient presented with an intracerebral hemorrhage in the anterior cranial fossa. The natural history of those aneurysms is obviously unknown, because of the very small number of cases, and we were compelled to use the known natural history data of the berry aneurysms when considering the management of our case, so treatment was indicated. We are aware that it was impossible to classify this aneurysm as a “berry” aneurysm, and there were no signs of infection (mycotic) or trauma. It was our impression that the aneurysm was due to the increased flow through this small artery, secondary to the right internal carotid occlusion. Consideration may be given to the possible effect of revascularization procedures in the natural history of these aneurysms, but there is no clear evidence that restoration of flow (external carotid-internal carotid bypass) would have any influence on it. The location of the aneurysm in a branch of the external carotid artery directly associated with most of the orbital and ocular blood flow precluded endovascular treatment. The aneurysm was then treated surgically, with removal of the lesion and coagulation of the ostium of the anterior ethmoidal artery in the anterior skull base. The patient made an uneventful recovery.
Our report illustrates an intracranial hemorrhage from an aneurysm of a branch of the external carotid artery, the right ethmoidal artery, probably secondary to increased blood flow. To the best of our knowledge, this is the sixth case reported in the literature. MR imaging and a complete angiographic study with inclusion of the external carotid circulation have proved to be important diagnostic tools in cases of unusual intracranial hemorrhages.
References
- Received May 30, 2005.
- Accepted after revision October 6, 2005.
- Copyright © American Society of Neuroradiology