
Abstract
SUMMARY: Using the Medicare Physician-Supplier Procedure Summary Master File, we evaluated the evolving use of fMRI in Medicare fee-for-service beneficiaries from 2007 through 2017. Annual use rates (per 1,000,000 enrollees) increased from 17.7 to 32.8 through 2014 and have remained static since. Radiologists have remained the dominant specialty group from 2007 to 2017 (86.4% and 88.6% of all services, respectively), and the outpatient setting has remained the dominant place of service (65.4% and 65.4%, respectively).
ABBREVIATIONS:
- CPT
- Current Procedural Terminology
- MEG
- magnetoencephalography
First introduced in 1991 for mapping the visual cortex, fMRI relies on detecting small changes in the blood oxygen level–dependent MR imaging signal as a result of neuronal activity following specific tasks.1 Since its introduction, fMRI has been widely used in neuroimaging research and increasingly incorporated into clinical practice. Currently, fMRI has value in the neurosurgical planning of conditions such as brain tumors or epilepsy, diagnosis and management of Alzheimer disease, and better understanding of psychiatric conditions.2
In January 2007, three distinct Current Procedural Terminology (CPT) codes were introduced to report fMRI services.3 Several studies have examined changing use of various radiologic modalities and procedures across various time periods,4,5 but no similar study has been performed to assess the nationwide adoption of fMRI. Given the relatively new translation of fMRI into clinical practice and the possibility that the high costs of fMRI might not be adequately reimbursed by current payor schemes,6 such information could potentially inform clinical practice guidelines and payer-coverage decisions. For these reasons and focusing on Medicare beneficiaries, we aimed to investigate the use patterns of fMRI with regard to both specialty groups and places of service since the introduction of unique CPT codes.
MATERIALS AND METHODS
The Annual Medicare Physician-Supplier Procedure Summary Master File from 2007 through 2017 was obtained from the Centers for Medicare & Medicaid Services. These files contain aggregated, submitted national Part B Medicare claims for all beneficiaries in the traditional Medicare fee-for-service program. These data are classified by codes for procedures, places of service, and provider specialties, along with the number of services both billed and denied. Physician-Supplier Procedure Summary files include no individual patient, diagnosis, or other encounter-specific information. Thus, their use does not constitute human subject research, and no institutional review board oversight was required for this study.
For this study, fMRIs were identified using the following service-specific CPT codes: 70554, 70555, and 96020 (Table 1).3 Analysis was performed as previously described using SPSS Statistics 25.0 (IBM) and Excel 2016 (Microsoft).4,5,7 fMRI use rates were calculated per 1,000,000 Medicare enrollees per year. Provider specialties and sites of service were grouped using relevant Medicare codes (Table 2).
CPT Codes for fMRI
Site of service and specialty groups studied with the corresponding codes
RESULTS
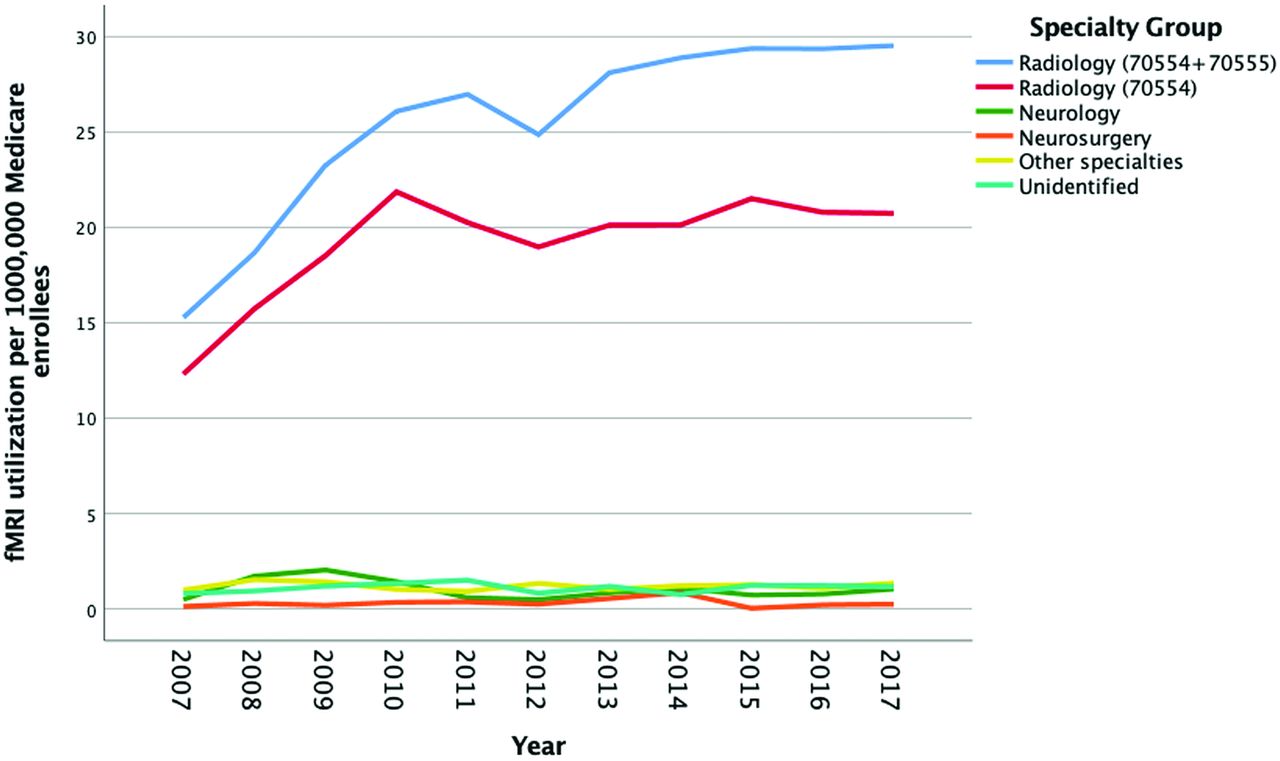
Between 2007 and 2014, use rates for fMRI studies performed on Medicare fee-for-service beneficiaries increased 85% (from 17.7 to 32.8) but have since stabilized (32.8, 32.6, 32.7, and 33.3 from 2014 to 2017, respectively). In 2007, radiology was the dominant specialty group, with a rate of 15.3 (versus 2.4 for all other specialties), which has continued to be the case since (Fig 1). The specialties with the second and the third highest rates were neurology and neurosurgery, respectively, with considerable year-to-year variability. Radiology, neurology, and neurosurgery accounted for overall use rates of 280.4, 11.2, and 3.4, respectively, during the entire time period.
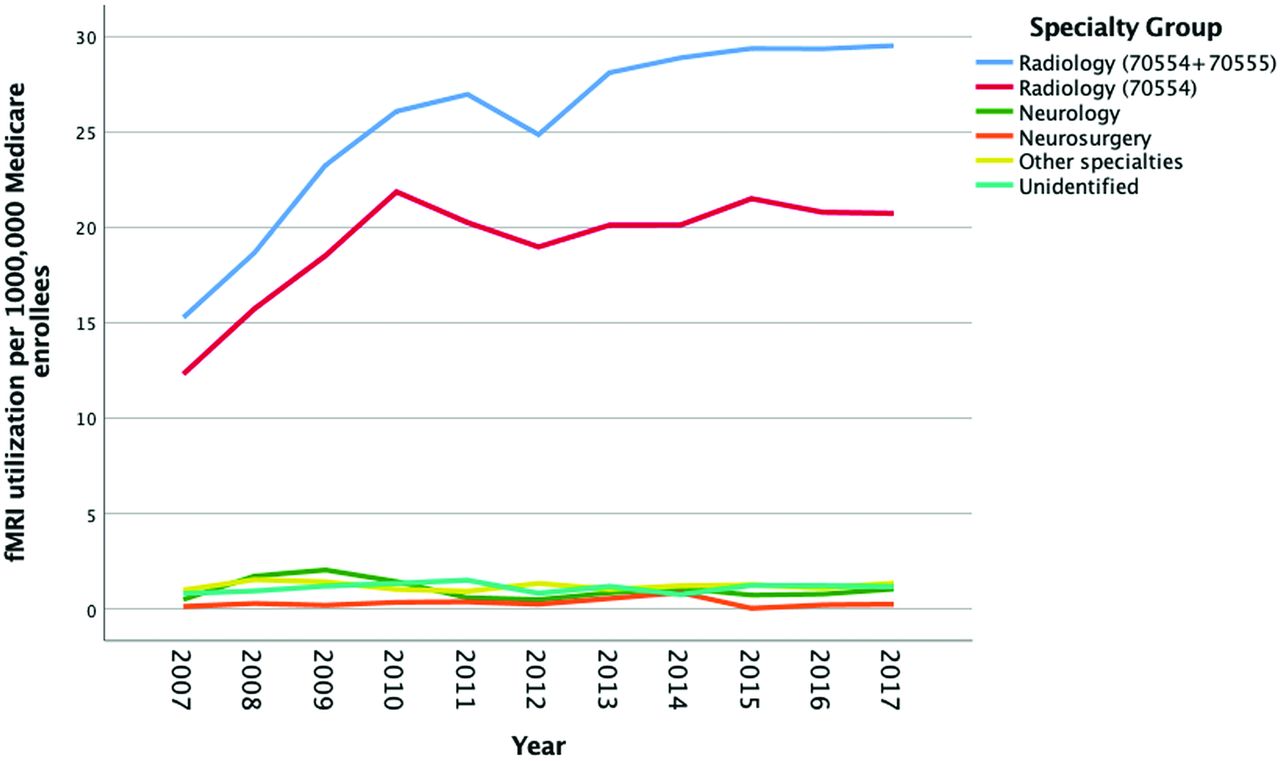
Functional MR imaging use in Part B Medicare beneficiaries from 2007 to 2017 by physician specialty group. Radiology (70554 + 70555) refers to the total billing of fMRI by this specialty. Radiology (70554) refers only to the 70554 CPT code. All other specialties reflect total billing.
Separate analysis of the CPT codes billed by radiology showed that the code 70554 (test selection/administration not requiring physician or psychologist administration) billing rate increased from 12.3 in 2007 to 20.7 in 2017 (Fig 1). Code 70555 (requiring physician or psychologist administration) radiology billing also increased from 3.0 in 2007 to 8.8 in 2017 (Fig 1). Code 96020 must always be accompanied by code 70555 during billing, though 96020 may be billed by a separate provider. For radiology, the rate of billing 96020 was 0.25 in 2007 and 5.18 in 2017. From 2007 through 2017, the rate of billing 96020 for radiology was always lower than for code 70555. However, the percentage of cases in which code 70555 was billed with 96020 by radiology has increased from 2007 to 2017.
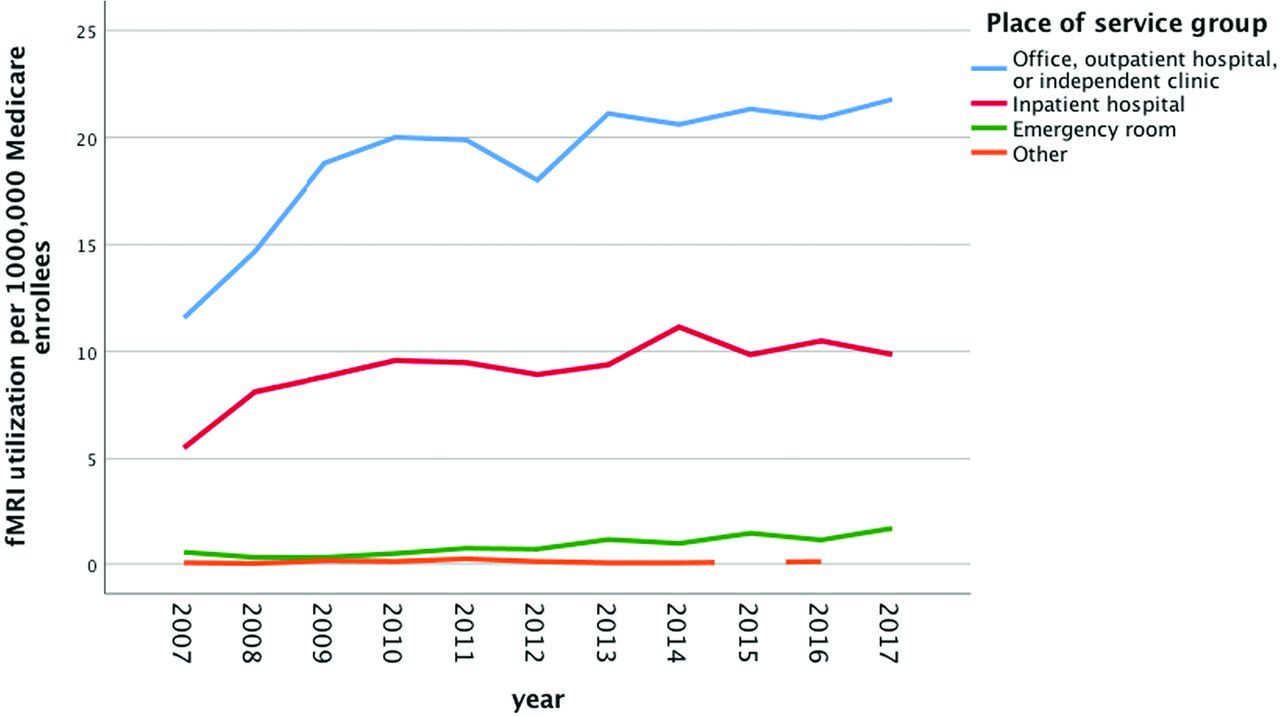
Most of the fMRI studies were performed in the outpatient (office, outpatient hospital, or independent clinic) setting, accounting for 65.4% in 2007 and 65.4% in 2017. The second and the third most common sites were inpatient hospital (31.1 in 2007 and 29.6 in 2017) and emergency department (3.1% in 2007, and 5.0% in 2017). fMRI use with regard to place of service is illustrated in Fig 2.

Functional MR imaging use in Part B Medicare beneficiaries from 2007 to 2017 by place of a service group.
DISCUSSION
Using annual aggregate Medicare fee-for-service claims files for all years for which unique CPT code data were currently available, we studied nationwide use of fMRI and found an increased adoption in the first 7 years after CPT codes became available, with a plateau in use thereafter. fMRI has consistently been performed predominantly by radiologists and predominantly in the outpatient setting, not dissimilar to patterns previously described for nonfunctional brain CT and MR imaging.8
Preoperative planning is one of the widely accepted applications of fMRI, which is commonly used in brain tumor surgery and in surgical resection of epileptic foci for certain patients.2 A recent study on national trends in brain tumor management during a relatively similar time period to our study (2004 to 2015) reported a total of 464,856 brain and other nervous system cancers among patients with a median age of 60 years, with an overall 56% rate of surgical procedures performed.9 In that study, 260,317 surgical procedures were performed on patients with brain cancer during the 11-year period. Not every neurosurgical procedure for brain cancer requires preoperative fMRI. However, given the benefit of fMRI in selected patients10⇓-12 and the difference between this number of surgical studies performed and the 10,056 fMRI studies billed during the similar 10-year period of our study, there may be a gap between potential ideal and actual fMRI use rates. Moreover, the prevalence and incidence of primary brain tumors in the United States are thought to be rising due to a combination of an aging population and improved diagnosis and therapies.9,13 Thus, it may be expected that the rate of brain surgery for these tumors will increase as well, particularly because the extent of tumor resection positively correlates with improved patient outcomes,14 and the need for preoperative fMRI should also increase.
Despite the increase in the use rates of fMRI, it is possible that barriers exist to furthering expansion of fMRI services and that current levels of fMRI use among Medicare beneficiaries might not be meeting the population-level clinical needs. Decreasing Medicare reimbursement ($618 in 2007 to $455 in 2017 for CPT code 7055415) is potentially a factor leading to the slowing of fMRI adoption. In addition, competing technologies for presurgical evaluation of refractory focal epilepsy and functional brain mapping, such as magnetoencephalography (MEG), have also grown.16 Increased expertise in the field of clinical MEG might also contribute to blunting the curve of fMRI use in recent years. However, despite the accepted clinical value of MEG,17,18 its accessibility is still low, with only 21 clinical MEG sites in 14 states listed by the American Clinical MEG Society.19 Future comparisons of MEG use with fMRI trends as well as regional use of MEG and fMRI are warranted.
Another potential barrier to fMRI adoption is likely related to the hardware, software, level of experience, and dedicated time required for acquisition, postprocessing, and interpretation of this study. Not surprisingly, radiologists have consistently performed the major share of the fMRIs for Medicare beneficiaries, and have experienced the largest growth since the introduction of dedicated CPT codes. In contrast, other specialties billed a relatively small number of fMRI services and showed no increases in use with time. Considering that 3 of the 4 main applications of fMRI concern neurology and neurosurgery (presurgical planning in brain tumors and epilepsy, more precise study of the level of consciousness in altered level of consciousness, and in follow-up of patients with traumatic brain injury and stroke), it is expected that those specialists participated as well in the provision of fMRI services. A secondary clinical application of fMRI is in diagnosis and efficacy assessment of certain psychiatric disease treatments.20 We identified no cases of fMRI billed by psychiatrists, possibly reflecting the low rate at which psychiatrists perform any imaging services.
A separate analysis of the CPT codes in this study showed that for radiology, both the number of billings for 96020 and the percentage of cases of simultaneous billing of codes 70555 and 96020 have increased from 2007 to 2017. This increase suggests that radiologists have become more comfortable across time acting as the physician who selects and administers fMRI paradigms, in addition to interpreting these studies. Alternatively, this may reflect an increased awareness of correct CPT billing practices. Regardless, despite the overall increase in radiology billing of 96020, the rate of billing of this code has always been lower than the rate of 70555, indicating that other specialties continue to perform and bill fMRI in conjunction with radiologists. Another possibility is that radiologists are performing both roles but incorrectly billing Medicare for this service.
The clinical use of resting-state fMRI, which is performed without an explicit task, has been advocated recently.21⇓-23 Once standardized clinical protocols are established, the use of resting-state fMRI may drive increased overall use of fMRI. The currently available fMRI CPT codes assume that a task is administered and there is no separate CPT code for isolated resting-state fMRI at this time. Therefore, it is not currently possible to assess the use of resting-state fMRI using national databases, so the impact of resting-state fMRI on overall fMRI use cannot be determined at this time.
Our study has limitations similar to those in other studies investigating the changing use of physician services. Most important, we studied only Medicare fee-for-service enrollees. Thus, our findings cannot necessarily be generalized to the population more broadly. However, considering that on the basis of the Surveillance, Epidemiology, and End Results Program data, approximately 40% of new national cases of brain and central nervous system cancers are associated with the older-than-65-year age group,24 our findings are, nonetheless, quite relevant. Additionally, we were constrained because certain Medicare provider codes did not allow identification of specific provider specialties (these were grouped as “unidentified specialty”). Moreover, we were not able to compare our findings on fMRI use trends with those of other advanced imaging techniques such as diffusion tensor imaging because there are no separate CPT codes for them. Future studies would benefit from the inclusion of both private and public payers as well as a larger age range of patients, particularly because presurgical fMRI is also used in the pediatric population.
In summary, fMRI use among the Medicare beneficiary population has markedly increased between 2007 and 2014 but has since plateaued. In this population, fMRI is primarily performed by radiologists in the outpatient setting.
Footnotes
Disclosures: Richard Duszak—RELATED: Grant: Harvey L. Neiman Health Policy Institute.* Danny R. Hughes—RELATED: Grant: Harvey L. Neiman Health Policy Institute.* Jason W. Allen—UNRELATED: Grants/Grants Pending: NIH R21 NS114603 (PI); NIH R01 MH111682 (Co-I); Radiological Society of North America Resident Grant (Mentor/Co-I), Comments: Hemodynamics, Thrombosis, and Stroke Risk in Patients With Carotid Webs, Impact of Trauma Exposure on Critical Periods in Brain Development, Functional and Structural Brain Connectivity Alterations in Visual Vertigo Syndrome: A prospective MRI Study of Central Vestibular Impairment in Mild Traumatic Brain Injury.* *Money paid to the institution.
References
- Received April 9, 2020.
- Accepted after revision June 22, 2020.
- © 2020 by American Journal of Neuroradiology




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.