
Abstract
SUMMARY: We describe a novel patient-positioning device for dynamic CT myelography. Dynamic CT myelography requires angling the patient’s spine to distribute dense contrast along the dependent thecal sac. The proposed device is constructed of a low-density reinforced polymer frame and can be raised or lowered to various heights with a hand-operated mechanism, allowing precise adjustment of the spinal angle and control of the contrast bolus, increasing the safety, reproducibility, and sensitivity of dynamic CT myelography.
ABBREVIATION:
- dCTM
- dynamic CT myelography
Dynamic CT myelography (dCTM) is an effective technique for the localization of CSF leaks and the detection of CSF venous fistulas.1 Unlike conventional CT myelography, in which the goal is the even diffusion of contrast material throughout the subarachnoid space, in dCTM, the goal is to distribute dense, unmixed contrast along the dependent thecal sac.2 When one looks for a CSF venous fistula or a ruptured meningeal diverticulum, the patient is in a decubitus position so that dense contrast fills the nerve root sleeves and meningeal diverticula. When a ventral dural defect is suspected, the patient is positioned prone with the hips elevated to localize the site of subarachnoid contrast extravasation into the ventral epidural space.3 Unlike digital subtraction myelography, which can use a tilt table to facilitate gravity-dependent egress of contrast from the lumbar puncture site toward the craniocervical junction, patient positioning in CT typically relies on the use of either a foam wedge or an inflatable mattress device positioned under the patient’s hips to angle the spine.4 A foam wedge can lead to a predictable, constant movement of contrast, but positioning a patient on top of the wedge from the beginning of the procedure precludes the accurate measurement of spinal opening pressure, and the prone position can often require additional pillows or other material to elevate the hips sufficiently to overcome a patient’s lumbar lordosis (Fig 1).Additionally, beginning the patient in the angled position can often result in decreased tension of the thecal sac, causing difficulty achieving a subarachnoid puncture. An inflatable mattress allows the patient to begin the examination in the horizontal position, followed by temporary inflation and deflation before scanning. However, the time required for inflation can be variable, and patient positioning can be unstable, often requiring assistants to secure the patient while the device is in the inflated position. In the case of type 1 or 2 CSF leaks, misjudging the timing of the contrast bolus or delays due to needing to reposition a patient after contrast injection can lead to poorer visualization of a dural defect and decreased diagnostic accuracy (Fig 2). To overcome the drawbacks of each commonly used technique, we designed a unique patient-positioning device to accurately and safely manipulate the spinal angle during dCTM, to increase the safety, reproducibility, and sensitivity of the examination.
Spine angulation using a foam wedge versus using the elevation device in suspected ventral dural defects. A, A patient with a suspected ventral dural defect, positioned on top of a foam wedge for dCTM. CT image obtained after contrast injection shows pooling of contrast at the patient’s lumbar lordosis (arrows) due to insufficient hip elevation. B, A separate patient with a suspected ventral dural defect on top of the novel positioning device. CT image obtained after contrast injection demonstrates egress of contrast from the puncture site to the craniocervical junction. Smaller FOV image demonstrates extravasation of contrast from the subarachnoid space into the ventral epidural space at C7–T1 (arrow), consistent with a ventral dural defect.

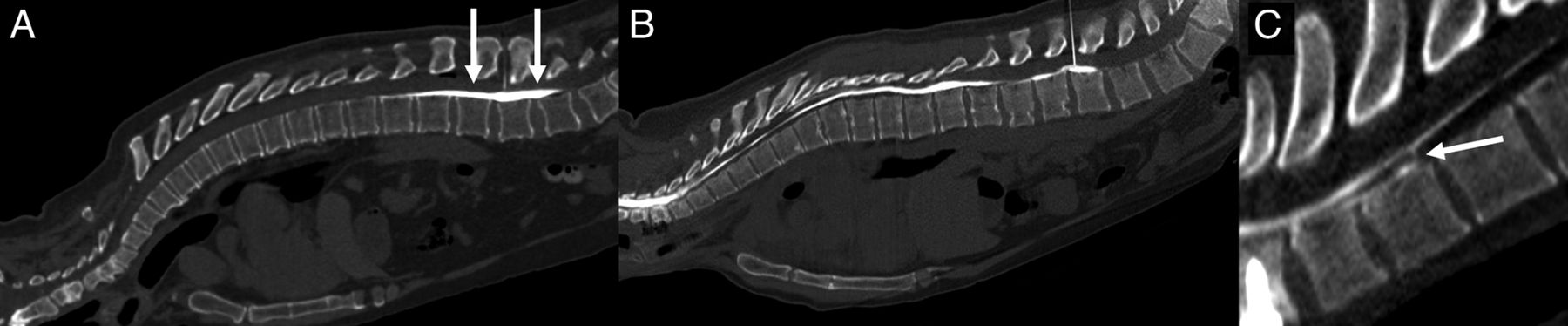
A ventral dural defect at T2–T3. A, Image obtained immediately after contrast injection demonstrates clear extravasation of contrast (arrow) from the subarachnoid space into the ventral epidural space, precisely localizing this patient’s dural defect. B, A second image obtained 38 seconds after the first demonstrates rapid diffusion of contrast throughout the ventral epidural fluid collection (arrows), obscuring the precise site of the dural defect.
Device Description
The device consists of a reinforced polymer frame covered with heavy duty canvas fabric and supportive foam cushioning, secured to the CT table at the end distal to the gantry by straps and 3D-printed plastic inserts. The inserts are specific to the channel along the length of the patient’s bed, which can vary among manufacturers. The device was initially designed for a Somatom Alpha CT table (Siemens). This CT table uses a channel size of 0.219 inches (5.6 mm) in diameter with a 0.129-inch (3.3-mm) slot opening. If the channel diameter and opening on the patient bed are within ±0.010 inches (± 0.25 mm) of the dimensions above, then the straps will be compatible with other CT tables. If the channel diameters vary more than these dimensions, new inserts may be 3D-printed at minimal cost. The device is bisected by a pivot point. At the fixed end, there is a hand-operated winch, which connects to the other end of the device by a polyester strap that runs beneath the frame (Fig 3). Underneath the mobile end proximal to the gantry, there are polyurethane wheels that allow translation along the Z-axis of the bore, depending on the length of the strap, which is controlled by the hand winch. The portion of the device that is included in the FOV is constructed of reinforced polymer and engineered polymers to minimize streak artifacts and the patient dose (Fig 4). The only metallic components present are along the most distal and proximal ends of the device, which remain outside of the FOV.

Device schematic.
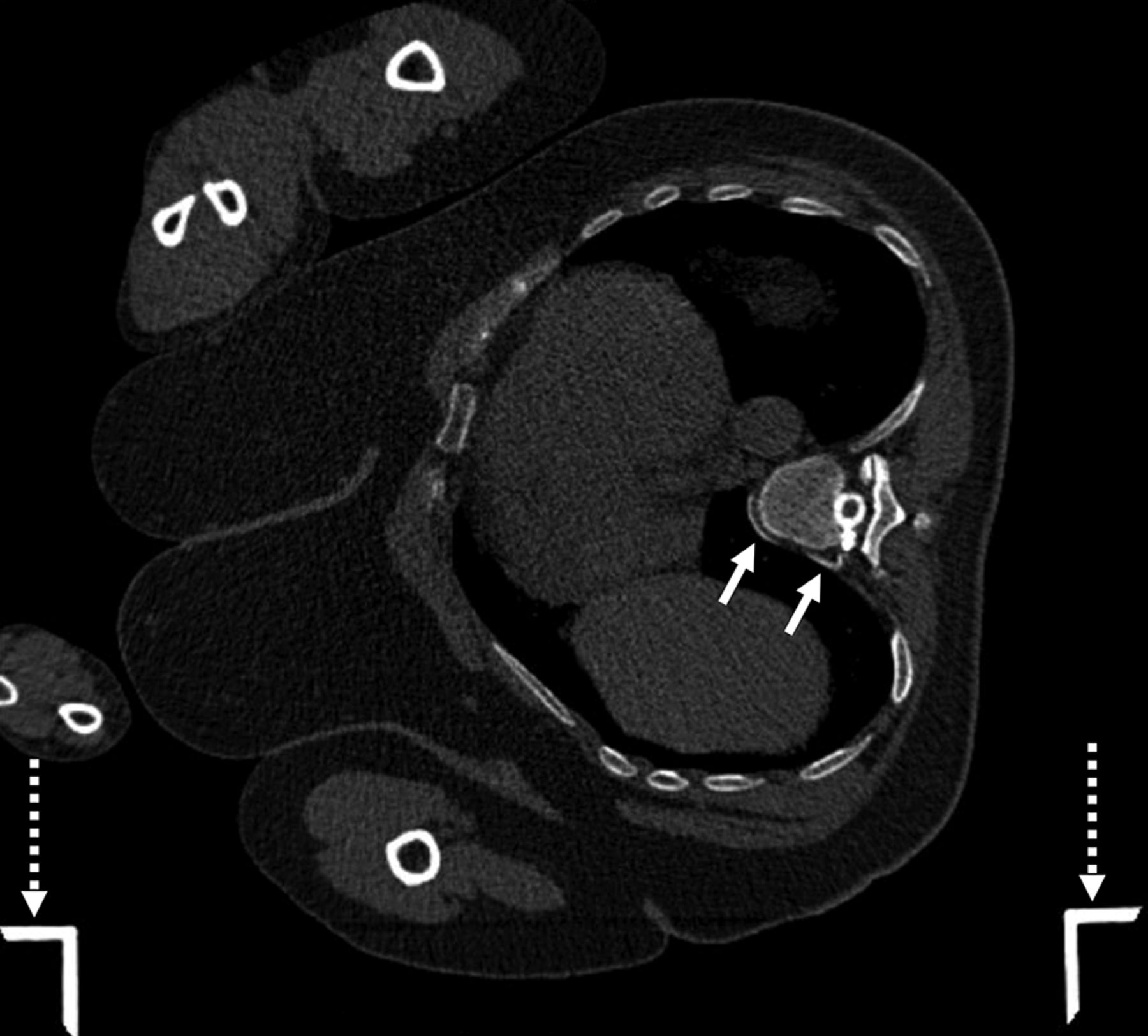
Localization of a CSF venous fistula using the positioning device. Axial CT image with a wide FOV demonstrates a patient in the right lateral decubitus position on top of the positioning device during dCTM with a CSF venous fistula (solid arrows) arising from a right T8–T9 meningeal diverticulum. The device frame (dashed arrows) generates no streak artifacts.
The overall device measures 91 inches long × 21 inches wide × 9 inches tall (231 × 54 × 23 cm), with the bed portion measuring 77 inches long × 20 inches wide (196 × 51 cm). It can support a patient weighing up to 300 pounds (136 kg) and up to 76 inches (193 cm) in height. Initially designed for the Somatom Alpha CT machine, the fixation straps can accommodate multiple CT machine types as long as the CT table uses a patient bed that is 17–19 inches wide with a minimum length of 91 inches and a curvature height of 2 inches from the edges to the bottom of the bed.
Device Use
The device can be unpacked and secured to the CT table in <5 minutes, best achieved with 2 operators. The patient can be positioned either decubitus or prone and is secured to the device with 2 fabric straps (Fig 5). At the mobile end proximal to the gantry, there are 2 fixed handles that can be held by the patient in the prone position. The patient can begin the examination in the horizontal or elevated position, depending on the preference of the operator. The height of the device can be adjusted depending on the size of the patient and is limited only by the width of his or her hips to allow the maximal elevation possible without obstructing movement into the gantry. Patient elevation takes approximately 8–12 seconds (Supplementary Online Video). Because the patient’s elevation is controlled and predictable, the needle may be left in the patient during height adjustment to allow additional contrast administration during the examination if necessary. If the patient is too large to fit in the gantry in the elevated position, the device can be elevated and subsequently lowered with the patient outside the gantry before scanning. Because the device is secured to the CT table, the patient may rotate to the contralateral decubitus position while remaining on the device if desired. Additionally, the patient may remain on the device during patching or other CT-guided procedures. Angling the patient, if desired, may allow needle trajectories that would otherwise require tilting of the CT gantry.

Example of the device in use in decubitus (A, Flat. B, Elevated) and prone (C, Flat, D, Elevated) patient positions.
CONCLUSIONS
We describe a dCTM patient-positioning device that offers several practical advantages over current commonly used methods for angling the spine on the CT table. By providing accurate and safe manipulation of the spinal angle, the device has the potential to increase diagnostic accuracy and procedural reproducibility and can accommodate patients of varying sizes. Patients can be positioned decubitus or prone and can start the examination in a horizontal or angled position. Because elevation is smooth and controlled, height can be adjusted while leaving the needle in place if needed. We believe that the incorporation of this device in clinical practice will improve patient outcomes and streamline the dCTM procedure for radiologists. Further studies are warranted to validate its effectiveness, assess patient and provider satisfaction as well as explore potential applications for manipulating the spinal angle in other CT-guided procedures. To date, we have performed 32 dCTM examinations using the device, all of which have been executed without compromised image quality. A patent is pending for the device, and it is our hope that it will be commercially available soon.
Acknowledgments
We acknowledge Ashesh A. Thaker, MD, Vincent M. Timpone, MD, and Josh Grip for input early in the design process.
Footnotes
Grant support from the Considine Family Foundation was used for the development of this device.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
- Received August 2, 2023.
- Accepted after revision September 3, 2023.
- © 2023 by American Journal of Neuroradiology








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.