
Abstract
Summary: The MR finding of an acute spinal epidural hematoma (SEH) can mimic epidural neoplastic or inflammatory lesions, because acute SEH appears hypointense on T1-weighted images and hyperintense on T2-weighted images. We report on two cases of acute SEH with unusual contrast enhancement patterns on MR images. Contrast enhancement can be an MR finding of acute SEH, especially in bleeding diathesis, which indicates an active lesion that needs early diagnosis and management.
Spinal epidural hematoma (SEH) is a rare but important cause of spinal cord compression. Usually, diagnosis of an SEH can be made without difficulty on the basis of specific signal intensity changes and morphologic findings on MR images. However, these can be confused with inflammatory or neoplastic mass lesions (1, 2), especially when a patient is in acute status or when intravenous contrast material has been administered; this confusion could delay diagnosis and patient management.
Case Reports
Case 1
A 69-year-old woman was referred to our hospital for sudden-onset bilateral lower limb weakness and severe back pain that occurred when she was urinating. Five years earlier, she received the diagnosis of hypertension and atrial fibrillation, at which time she began a regimen of aspirin (100 mg q.d.), digoxin (0.5 mg, q.d.), and Warfarin (5 mg q.d.). Neurologic findings showed decreased sensation below the T12 level. The motor grade of the lower limbs was 3. Laboratory findings were: platelet count, 203,000 mm3; prothrombin time, 22.4 seconds (INR, 1.86); and activated partial thromboplastin time, 45 seconds. Blood pressure was recorded at 208/125 mm Hg.
Because clinical findings were suspicious for acute spinal compression, MR imaging of the thoracic and lumbar spine was performed 10 hours after symptom onset. Imaging findings showed a large epidural hematoma in the dorsal aspect of T9–L3, indicated by heterogeneous hyperintensity on sagittal T2-weighted images and isointensity relative to spinal cord on sagittal T1-weighted images (Fig 1A and B). A spotty enhancement within the parenchyma of the hematoma was found on contrast-enhanced sagittal and axial T1-weighted images (Fig 1C–E). Although MR findings indicated acute SEH, the differential diagnosis included vascular malformation because of this spotty enhancement.

Case 1, a 69-year-old woman. MR images of the thoracolumbar spine, obtained 10 hours after sudden-onset severe back pain, show a large SEH in the dorsal area of T9–L3.
A, Sagittal T2-weighted (2000/80/2 [TR/TE/NEX]) image shows the hematoma as a heterogeneously hyperintense area (arrows).
B, Sagittal T1-weighted (400/20/2) image of the lumbar spine shows an isointense hematoma (arrowheads).
C, Contrast-enhanced sagittal T1-weighted image (400/20/2) shows an enhanced area (arrows) within the hematoma (arrowheads) at the level of T12.
D, Axial T1-weighted image (400/20/2), at the level of T12, shows an isointense hematoma (arrowheads).
E, Contrast-enhanced axial T1-weighted image (400/20/2), at the level of T12, shows an enhanced area (arrow) within the hematoma (arrowheads).
Laminectomy of T9–L3 was performed 18 hours after symptom onset. Hematoma was the only finding at surgery. The patient’s neurologic status improved after rehabilitation, and she was discharged with a muscle power grade of 4–5.
Case 2
An 82-year-old diabetic man fell and was sent to our emergency room. He had a history of hypertensive cardiomyopathy and a cerebrovascular accident that had been treated with aspirin (100 mg, q.d.) and Warfarin (5 mg, q.d.) for many years. In the emergency room, he was found to have respiratory failure, quadriplegia, and an esophageal ulcer with bleeding. Neurologic findings showed complete quadriplegia, loss of sensation in the body, and loss of anal tone. Laboratory findings were: platelet count, 85,000 mm3; promthrombin time, 19.2 seconds; and activated partial thromblastin time, 39 seconds. Blood pressure was recorded at 113/52 mm Hg.
After intubation to enable adequate blood oxygen saturation and a blood transfusion to offset upper gastrointestinal bleeding, MR imaging of the cervical spine was performed 4 hours following symptom onset. MR findings showed a large lentiform SEH in the dorsal area of C5–C7. The hematoma was hyperintense relative to spinal cord on sagittal T2-weighted images, slightly hyperintense on sagittal proton density-weighted images, and isointense on T1-weighted images (Fig 2A–C). No abnormal signal intensity change of the spinal cord was found. On postcontrast MR images, multiple areas of spotty enhancement were noted within the SEH (Fig 2D and E). MR confirmed the diagnosis of SEH, which could have been caused by a vascular lesion or tumor bleeding.

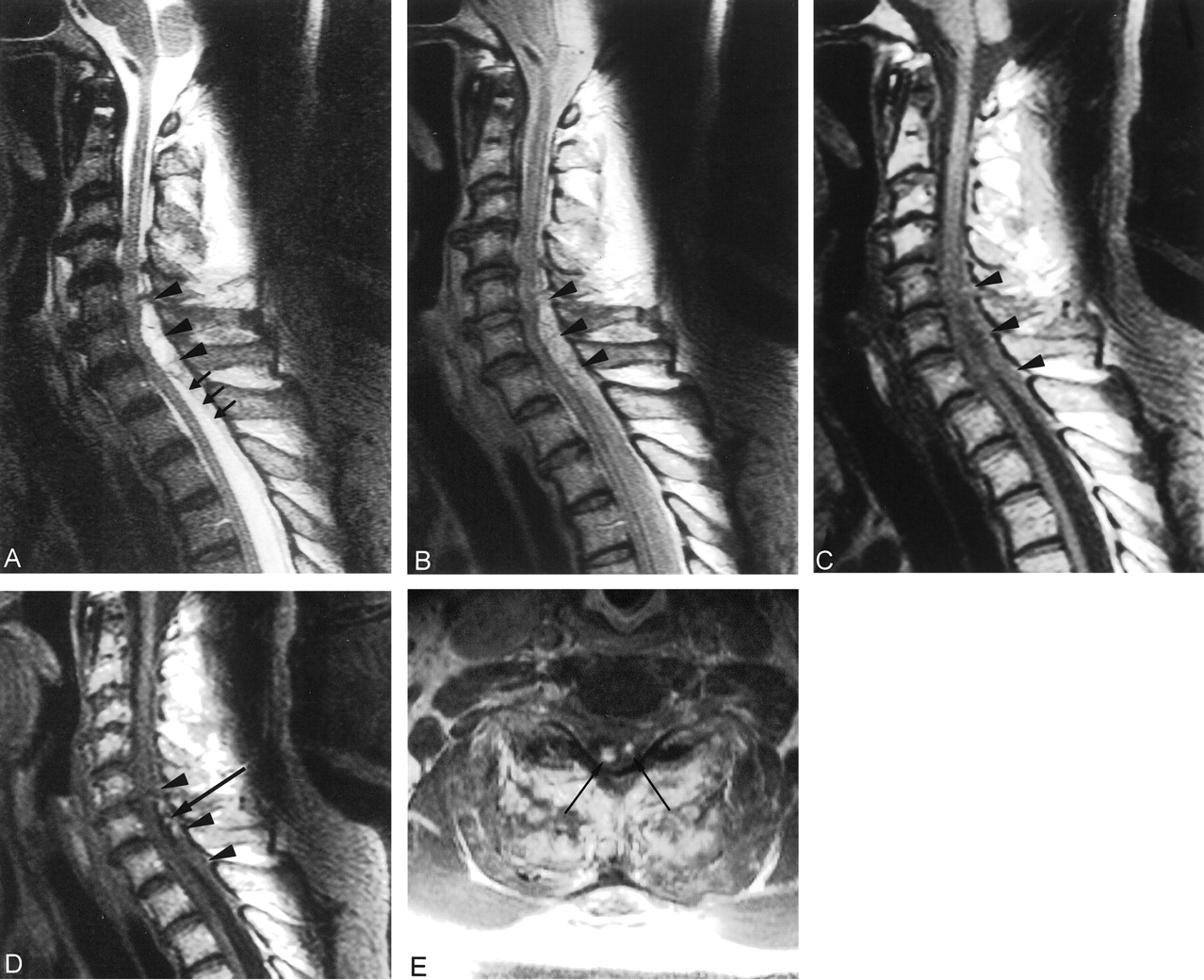
Case 2, an 82-year-old man. MR images of the cervical spine, obtained 4 hours after a fall, reveal a large SEH in the dorsal area of C5–C7.
A, Sagittal T2-weighted (2000/80/2) image shows a hyperintense epidural hematoma (arrowheads). A hypointense displaced dura (arrows) indicates the epidural location of the hematoma.
B, Sagittal proton density-weighted (2000/20/2) image shows a slightly hyperintense SEH (arrowheads).
C, Sagittal T1-weighted (400/20/2) image reveals the isointense SEH (arrowheads).
D, Contrast-enhanced sagittal T1-weighted (400/20/2) image shows multiple, enhanced spots (arrow) within the hematoma (arrowheads).
E, Contrast-enhanced axial T1-weighted (400/20/2) image shows spotty enhancement (arrows) at the level of C6.
Emergent laminectomy at C3–C7 was performed, which revealed a recently formed hematoma in the epidural space. No tumor growth or vascular lesion was found. The patient showed no clinical improvement after decompression of the SEH. He was transferred to a rehabilitation center in bed-ridden status. The patient could not be weaned from a ventilator because of spontaneous impaired respiratory function.
Discussion
Epidural hematoma in the spinal canal is unusual; however, with the advent of MR imaging, diagnosis of SEH has been made more frequently. Usually, hematoma sites are found in the cervical and thoracic spine (1–4). Most SEHs are located dorsal to the dural sac because of the firm adherence of the dural sac to the posterior longitudinal ligament in the ventral aspect of the spinal canal. In contrast, spinal subdural hematomas are mostly located ventral to the spinal cord (5, 6). An SEH may occur spontaneously, unrelated to iatrogenic procedures and major trauma, or it may be associated with anticoagulant therapy, bleeding diathesis, use of aspirin, or minor trauma (1–4, 7). SEHs are venous in nature, because the venous plexus lacks valves; therefore, the venous plexus permits a reversal in blood flow during pressure increase from physical activity (4, 5).
Clinical findings of SEH usually comprise neurologic deficit during the acute stage, including motor and sensory deficits that rapidly develop into paraplegia, quadriplegia, or autonomic dysfunction. Prognosis for neurologic recovery depends on the patient’s preoperative neurologic status and duration of neurologic dysfunction (5, 6, 8).
MR imaging is effective in the diagnosis of SEH because of its sensitivity in depicting soft-tissue lesions and its ability to survey and cover the full extent of hematomas (1–6). Sagittal MR imaging usually shows, in the dorsal epidural space, the biconvex hematoma with well-defined contours and tapering superior and inferior margins. On the axial section, an SEH appears as a concave or convex mass. The signal intensity of an SEH varies over time. During the acute stage, the hematoma is isointense relative to spinal cord on T1-weighted images and hyperintense relative to spinal cord on T2-weighted images. During the subacute stage, such as 30 hours after symptom onset, the hematoma usually has a heterogeneous hyperintensity on both T1- and T2-weighted images. The increased heterogeneity of the hematomas results from degradation products of hemoglobin. A ventrally displaced curvilinear dura, seen as hypointensity on sagittal T1- and T2-weighted images, is continuous with adjacent dura and is easily seen when the hematomas are dorsally located (Fig 2A). The displaced dura on sagittal or axial MR images is an important finding, because it indicates that the hematoma is epidurally located. Displacement of the epidural fat with a cupping appearance is another such important finding.
In our two patients, contrast enhancement of the hematomas associated with hyperacute status had similar presentations of bleeding diathesis. We could not determine the cause of the enhancement, but speculate it might have been a continuous extravasation of contrast medium from the torn epidural venous plexus to the hematomas or an engulfed epidural vascular soft tissue within the acutely enlarging hematomas (9). Nevertheless, contrast enhancement in SEH indicates the lesion is active, and aggressive treatment, such as surgery, is needed. In our search of the literature, we found only three cases describing enhancement patterns of SEH on postcontrast MR images (9–11). One was a case of hemophilia A and AIDS; the other two were spontaneous SEH (Table). We believe that contrast enhancement is an MR sign of acute SEH, especially in patients with a bleeding diathesis. Perhaps few reports exist regarding the contrast enhancement characteristics associated with SEH because diagnoses were made on the basis of signal intensity changes and morphology shown on MR images obtained without contrast medium or because MR imaging was performed too soon after symptom onset.
Reported cases of contrast enhancement of SEH diagnosed on the basis of MR findings
SEH can be confused with neoplastic lesions, because metastasis are isointense or hypointense relative to spinal cord on T1-weighted images and hyperintense relative to spinal cord on T2-weighted images. It is usually associated with vertebral infiltration and a pathologic fracture that spares the disk and surrounding soft-tissue lesion (1). SEH is commonly located in the dorsal portion of the spinal canal. It rarely surrounds the spinal cord but compresses it from one side. Epidural abscesses usually lie ventrally and involve disk and adjacent vertebral bodies. These lesions may extend continuously on multiple levels and are continuous with the infected disk spaces. Necrotic areas often appear on MR images as ring or marginal enhancement (4). Patients with spinal epidural abscess may show clinically infectious signs. Spinal subdural hematomas are mostly located ventral to the spinal cord and occur far less frequently than do SEHs (12). An SEH never surrounds the dural sac, but subdural fluid collections, not restricted in extent, may surround the spinal cord or cauda equine. Because no displaced dura exists between the subdural hematoma and spinal cord, the surface of the subdural hematoma can be irregular.
Conclusion
We report on two cases of SEH that manifested contrast enhancement at MR imaging. In both cases, patients had been on long-term anticoagulant therapy and agreed to undergo MR imaging of the spine soon after symptom onset. The MR finding of contrast enhancement may be attributed to continuous extravasation from a torn epidural venous plexus or to an enlargement of an existing hematoma that engulfs the epidural vascular soft tissue. The MR finding of contrast enhancement in the presence of an SEH indicates an active lesion that should not be confused with an inflammatory or neoplastic process; doing so could delay diagnosis and therapeutic intervention.
Footnotes
Presented at the 39th annual meeting of the American Society of Neuroradiology, Boston, Massachusetts, May 2001.
- Received April 2, 2002.
- Accepted after revision July 22, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.