
Abstract
Summary: We report a case of a 45-year-old woman known to have a familial form of blue rubber-bleb nevus syndrome (BRBNS). The patient developed severe occipital headaches and bilateral retroauricular bruits. Cerebral angiography showed a large dural arteriovenous fistula in the torcular region. Central nervous system involvement in BRBNS is not often reported, and most cases of BRBNS are sporadic.
Blue rubber-bleb nevus syndrome (BRBNS) is a rare disease characterized by cavernous angiomas of the skin and gastrointestinal tract. Bean described the condition in 1958 (1), and more than 200 cases have been reported since then. The lesions are usually present at birth or appear in early childhood, and they tend to increase in size and frequency with age. Vascular malformations may be present in other locations, and a few reports describe associated involvement of the central nervous system. Most cases are sporadic, but dominant autosomal or sex-linked transmission has been reported in some families.
We report a case of BRBNS associated with a dural arteriovenous fistula (DAVF). We wish to emphasize the possibility of brain involvement in BRBNS and also the familial incidence of the disease.
Case Report
A 45-year-old woman with a confirmed diagnosis of BRBNS was referred for neurologic consultation (V.B.) because of a 6-month history of severe occipital headaches provoked by physical stress. Complaints of bilateral retroauricular bruit were also noted.
BRBNS had been diagnosed when the patient was aged 39 years on the basis of the typical appearance and histologic features of cutaneous and digestive lesions. Multiple bluish masses of various sizes had been present on the patient’s trunk, limbs, upper lip, and tongue for several years. These masses increased in size and number as the patient aged. The lesions were soft, compressible, and painless. The skin biopsy specimen of a cutaneous lesion demonstrated a cavernous angioma. Upper gastrointestinal tract endoscopy performed at the age of 39 years revealed esophageal and gastric cavernous angiomas, and results of tests for occult blood in the stool were positive. Four years later, the patient had to be treated for severe microcytic and hypochromic anemia.
The patient’s two daughters, aged 25 and 21 years, were said to have similar skin lesions, as did her father and two sisters. In fact, her daughters had skin lesions typical of BRBNS.
Neurologic examination showed right enophthalmos and ptosis, which had been present from early childhood. Motor and sensory findings were normal. The patient had no abnormal eye movements, and the results of a funduscopic examination were unremarkable. Cranial CT revealed some dilated intracranial veins, cerebral edema, and a lacunar stroke involving the left caudate nucleus.
The patient was admitted to the neurology department for additional studies and treatment. Results of routine blood chemistry and coagulation tests were normal. MR imaging of the brain demonstrated enlarged cortical veins in the cerebral hemispheres and posterior fossa (Fig 1A), enlarged torcular herophili, straight and falcine sinuses, and tonsillar prolapse (Fig 1B). Images also demonstrated thrombosis of the left sigmoid sinus. Cerebral angiography demonstrated a large DAVF in the torcular region. The lesion was supplied by several enlarged branches of the right and left occipital, middle meningeal (Fig 2A), and ascending pharyngeal arteries, as well as by branches of the right meningohypophyseal trunk. Additional supply originated from dural branches of both vertebral arteries and from a transarachnoid anastomosis from the superior cerebellar arteries. The left sigmoid sinus was occluded, and severe right jugular bulb stenosis caused insufficient drainage through the right sigmoid and lateral sinuses, resulting in retrograde flow into the straight and superior sagittal sinuses. The cerebral veins opened into the diploic and facial veins and toward the cavernous sinus, whereas the posterior fossa venous system opened into the suboccipital venous plexus and medullary veins (Fig 2B).

MR images obtained on admission.
A, Axialproton density-weighted image (2530/25 [TR/TE]) shows enlarged veins in the posterior fossa.
B, Sagittal T1-weighted image (450/15) shows an enlarged straight sinus and the presence of a falcine sinus. Note the tonsillar prolapse.
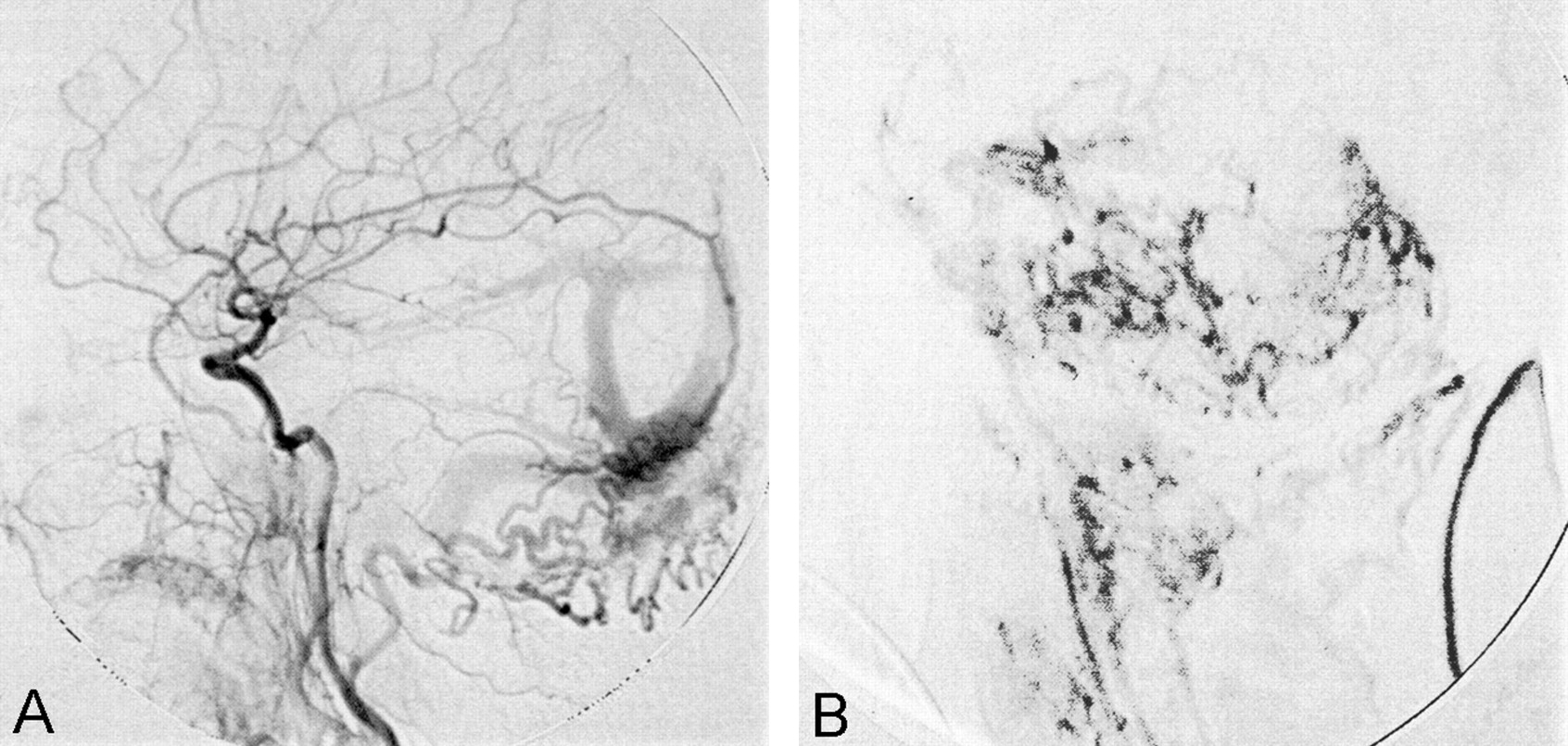
Carotid and vertebral angiograms.
A, Left common carotid artery angiogram demonstrates a DAVF in the torcular region. It is supplied by both the occipital and middle meningeal arteries and drains in a retrograde fashion in the superior sagittal and straight sinuses. Note the presence of a falcine sinus.
B, Venous phase of a left vertebral angiogram shows substantial venous stagnation in the posterior fossa. Note the dilated premedullary and retromedullary veins.
The patient underwent endovascular embolization of dural branches of the right occipital and right middle meningeal arteries with Histoacryl (Enbucrilate; Braun, Tuttlingen, Germany). Her headaches resolved after embolization, and she was discharged home from the hospital. Eight months later, the patient still complained of a retroauricular bruit, which was more intense on the left side. Therefore, the dural branches of the left occipital and left middle meningeal arteries supplying the fistula were embolized with Histoacryl. About 1 year later, after a subacute onset of seizures and a deterioration of consciousness, the patient was admitted with a diagnosis of intracranial hypertension. Further embolization of branches of the right occipital artery, the left middle meningeal artery, both vertebral arteries, and the posterior meningeal artery arising from left posteroinferior cerebellar artery was performed. The patient improved. When this report was written, the patient was being followed up as an outpatient, and she no longer reported cranial bruit or headaches.
The patient’s daughters also underwent cerebral MR imaging to look for cerebral vascular malformations. One of them had a developmental venous anomaly (DVA) in the cerebellum, and the other had a cavernous angioma of the orbit.
Discussion
As usual, the main clinical features leading to the diagnosis of BRBNS in our patient were vascular malformations of the skin and gastrointestinal tract. The vascular malformations of the skin are usually bluish, soft, and easily compressible, leaving an empty sac that refills slowly (2). Blue rubber-bleb nevi typically show cavernous spaces lined by a single layer of endothelial cells and separated by varying amounts of collagenous and fibrous tissue (3, 4). Unlike the cutaneous lesions, intestinal angiomas commonly bleed, producing anemia (2). Many other locations may be involved: the oronasopharynx, liver, spleen, heart, lung, pleura, peritoneum, kidney, thyroid, parotid, skeletal muscle, bone, bladder, brain, penis, vulva and eyes (2, 5, 6). Systemic complications, particularly chronic disseminated intravascular coagulation, can occur (7–9).
Central nervous system involvement is rarely described in cases of definite or possible BRBNS. Most cases are associated with cerebral vascular malformations, which have been designated hemangiomas or angiomas; these may correspond to cavernous malformations (7, 8, 10–13). In 1978, Waybright et al (4) described a patient with BRBNS who presented with focal seizures and focal neurologic signs. That patient had various cerebral vascular malformations, including thrombosis of a vein-of-Galen malformation, cavernous angiomas, and arteriovenous malformations. Some then suggested that the pathologic features in BRBNS could be more varied than previously recognized (4, 5). BRBNS was found to be associated with different conditions, including sinus pericranii and a giant venous angioma (14), vertebral hemangioma causing spinal cord compression and vertebral collapse (15), vascular dementia due to chronic disseminated intravascular coagulation, and multiple cerebral infractions (16). BRBNS has also been associated with a cerebellar medulloblastoma in a patient with no vascular malformations in the central nervous system (16).
Among the reports of nervous-system involvement in BRBNS, ours may be the first case that describes an association of BRBNS with DAVFs. Intracranial DAVFs are arteriovenous shunts imbedded in the dura mater and consist of abnormal direct communications from a dural arterial supply to a dural venous drainage. They account for 10–15% of all intracranial arteriovenous malformations, and more than one-half of them occur in the posterior fossa. DAVFs clearly seem to be acquired lesions preceded by dural venous obstruction. Our patient had evidence of sinus thrombosis, which may have predisposed her to the formation of the arteriovenous fistula.
Hematologic disturbances, such as chronic disseminated intravascular coagulation, have been reported in a few cases of BRBNS (7–9), but they were not found in our patient.
One patient’s daughter had BRBNS in association with a cerebral DVA. In a series of 40 patients (17), the frequency of DVAs with extensive superficial cervicofacial venous malformations was found to be 20%, in contrast with the frequency of 0.05–0.25% in the general population. Because most cerebral DVAs are asymptomatic and incidentally discovered during autopsy or imaging studies, they may be more frequently associated with BRBNS than the reports of BRBNS suggest.
The presence of cutaneous lesions typical of BRBNS should alert the clinician to the potential for intracranial vascular malformations. Furthermore, dural arteriovenous shunts should be added to the list of vascular malformations associated with BRBNS.
The present case is also relevant because of the familial history. Although most cases of BRBNS are sporadic, dominant autosomal transmission has been reported in a few families (18–21), as in ours. A gene for familial venous malformations has been mapped to chromosome arm 9p in large kindreds (22, 23), and some have suggested that the gene for autosomal dominantly inherited venous malformations might be identical to that of BRBNS (23).
References
- Received December 3, 2002.
- Accepted after revision March 25, 2003.
- Accepted after revision March 25, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}