
Abstract
Summary: Herein we describe the technique of CT-guided lumbar or thoracic bone biopsy performed with a larger bore needle and coaxial system. The use of the external sheath cannula as a coaxial system led to an accurate diagnosis in all 19 patients who underwent the procedure. Bleeding at the biopsy site occurred in two patients and was controlled by insertion of Gelfoam. No other complications were encountered. We suggest that our procedure is more effective, reliable, safe, and rapid than the traditional technique.
Modern imaging techniques can depict small and even asymptomatic bone lesions. Open biopsy is a major surgical procedure associated with morbidity and complications. Percutaneous biopsy under fluoroscopic or CT (CT) guidance is a safe and almost painless, and is preferred for lesions that have a soft-tissue component or are located close to vital structures. The reported accuracy of CT-guided spinal bone biopsy is 67–97%, and the complication rate ranges from 0–26% (1–7).
CT-guided bone biopsy can be performed with different types of needles (7, 8). The Ackerman needle (Cook Medical, Bloomington, IN) has the advantage of a coaxial system and has been found to be safe for biopsy retrieval; however, our initial experience with the Ackermann needle was unsatisfactory because of the presence of a crush artifact in a few cases, which made the histologic diagnosis difficult. This prompted us to try a larger bore needle with a newly developed coaxial system. Our aim is to describe our biopsy technique, which led to an accurate diagnosis in 19 consecutive patients.
Description of the Technique
The study group consisted of 19 consecutive patients (seven men, 12 women) aged 25 to 83 years (mean ± SD, 64.1 ± 14.9 years) who underwent CT-guided lumbar (n = 12) or thoracic (n = 7) bone biopsy in our center. Lesions were located in the following regions: one in T7, one in T8, three in T10, two in T11, two in L2, three in L3, five in L4 and two in L5. Indications for biopsy were osteolytic lesions (n = 11), osteoblastic lesions (n = 3), pathologic fracture (n = 3), and sclerotic collapse vertebra (n = 2). Patients with lesions in the sacral bone or those who underwent fine needle aspiration were excluded.
The study was approved by the institutional ethics committee and all patients gave informed consent before undergoing the examination. Aspirin and other non-steroidal, anti-inflammatory medications were discontinued 7 days before the procedure. Immediately before the biopsy, complete blood count, activated partial thromboplastin time, and prothrombin time were measured.
Twelve biopsies were performed with the 8-gauge Jamshidi needle (Manan Medical Products, Inc., Northbrook, IL) and seven with the 8-gauge Waldemar spinal biopsy needle (Link, Hamburg, Germany) (Fig 1). All biopsies were done under CT guidance (Elscint 2400 Elite, Haifa, Israel or Picker International Inc., Cleveland, OH) with the patients in the prone position. Maximum attention was addressed to the patient’s comfort. The lesion was localized, and the point of entry on the skin was marked in accordance with the biopsy technique (4–7). Three approaches were used: posterolateral (n = 2) for the upper lumbar vertebrae; transcostotransversal (n = 6) for the thoracic vertebrae; and transpedicular (n = 11) for the L4-L5 vertebrae and the thoracic spine. At the beginning of the procedure, a local anesthetic (1% Esracaine) was injected subcutaneously with a 25-gauge needle. Thereafter, to anesthetize the tract up to the periosteum, an 18-gauge, 24-cm-long needle (Fig 2) was inserted. When the tip of the needle reached the periosteum, additional Esracaine was injected, and the hub of the needle was cut, transforming it into a guidewire (Fig 2). An external sheath measuring 5.2 mm in diameter was slid over the guidewire by using a rotary motion for deeper penetration, and the wire was removed. The biopsy needle was inserted through the cannula. Before the bone was entered, a scan was obtained to check the location and direction of the needle. The periostium was penetrated by moving the Jamshidi or the Waldemar needle in a clockwise-counterclockwise motion with the sharp pointed stylet. The biopsy needle was then advanced slowly through the cortex to reach the lesion (Fig 3).
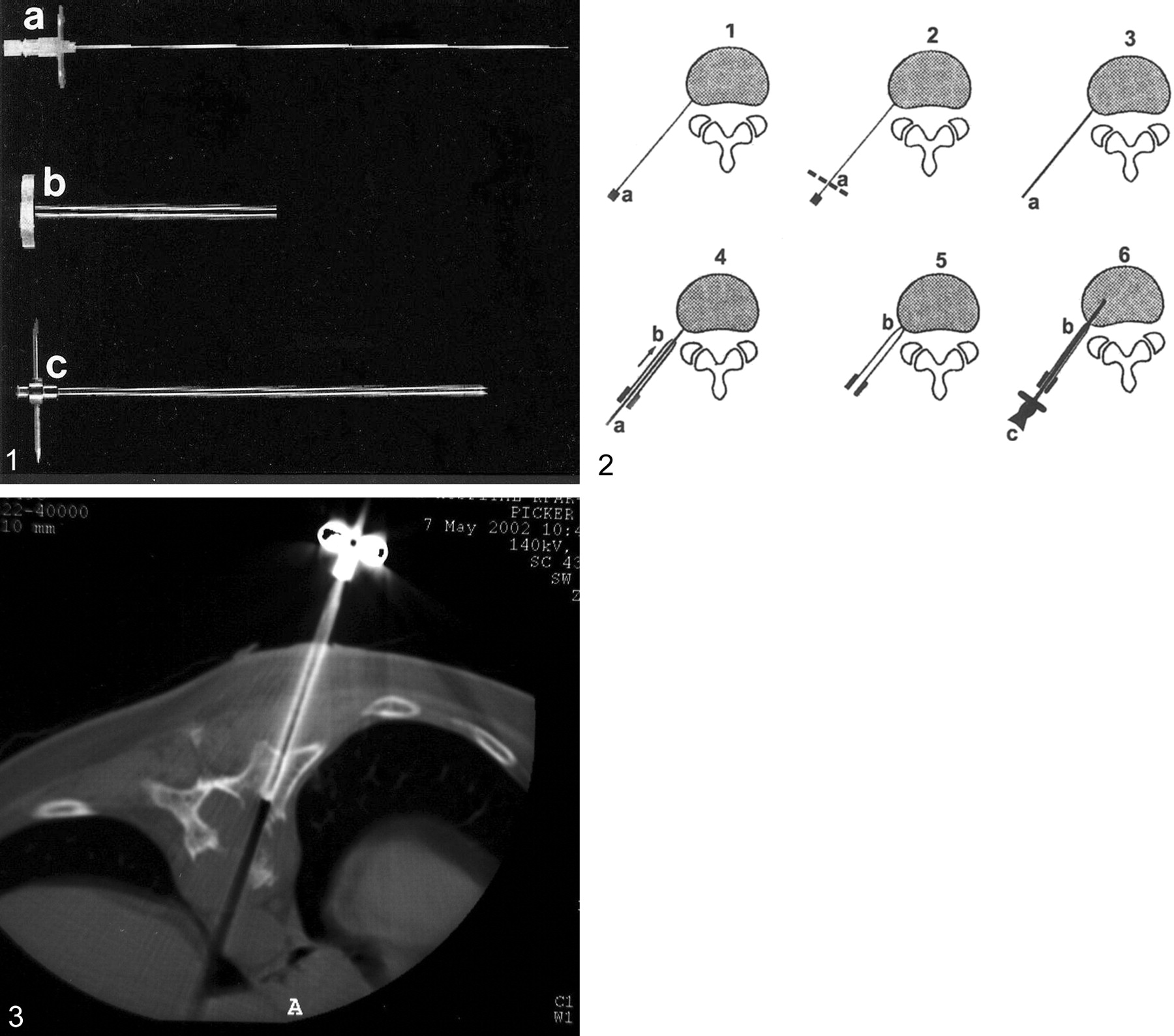
Equipment for coaxial vertebral biopsy.
A, An 18-gauge, 24-cm-long anesthetic needle.
B, external sheath cannula 5.2 mm in diameter.
C, Waldemar spine biopsy needle.
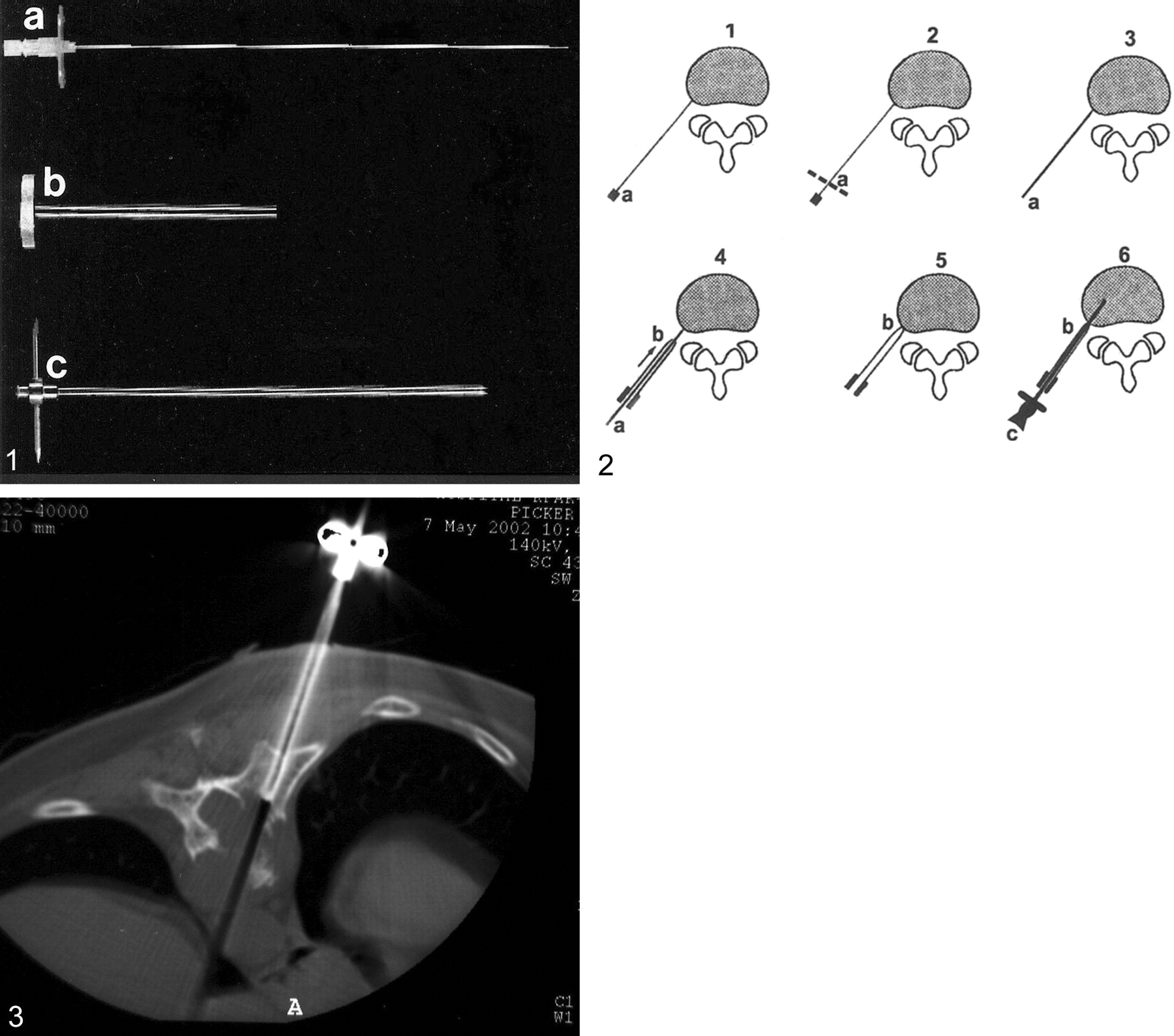
Percutaneous vertebral biopsy with the coaxial system. Parts shown in Figure 1 are labeled.

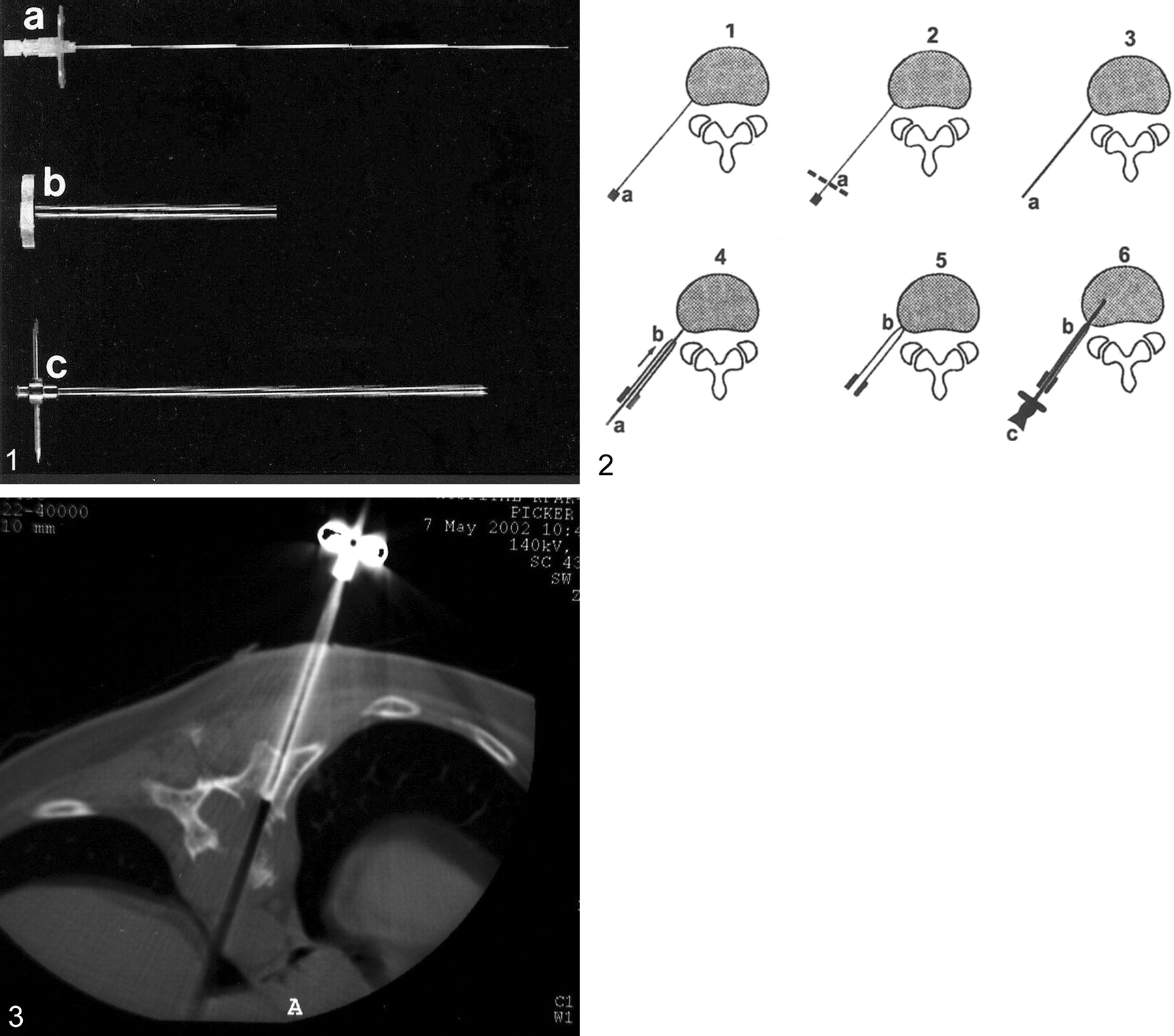
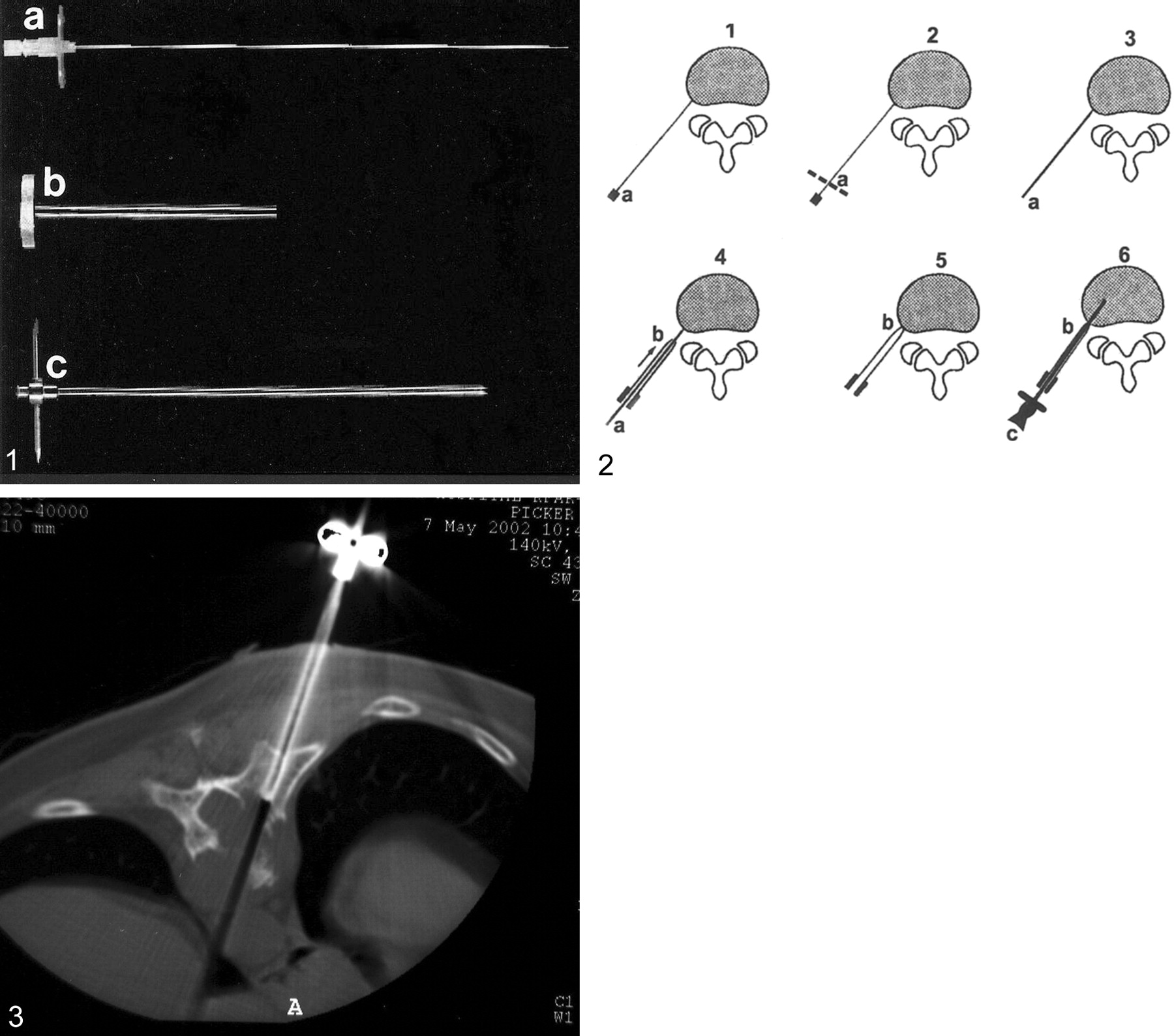
A 35-year-old patient with lytic lesion (plasmocytoma) involving the body of T10. Percutanous trans costal-transverse approach: the tip of the biopsy needle is visible at the margin of the mass.
An effort was made to obtain several specimens from the same tract, by using the external cannula in the coaxial system. The needle was retracted under continuous suction.
Biopsy material was obtained in all cases. None of the biopsy findings were falsely negative. The use of the external sheath cannula as a coaxial system led to an accurate diagnosis in all 19 cases (100%). The final diagnosis was osteoporotic fracture in two patients, multiple myeloma or plasmocytoma in five, metastasis in three, B cell lymphoma in three, and diskopathy in one. No malignancy was found on the basis of biopsy study in five patients, including three patients with a lytic lesion with a sclerotic border on CT scans and two with sclerotic collapse. In all five cases, clinical follow-up confirmed that the lesions were benign. Bleeding at the biopsy site occurred in two patients with a vascular lesion and was controlled by insertion of Gelfoam through the cannula. No other complications were encountered. Neurologic examinations showed no change after the biopsy procedure. The procedure was well tolerated by all patients and no patient complained of radicular pain either immediately after the procedure or during the next few postoperative days.
Discussion
Percutaneous biopsy performed with local anesthesia is a safe and highly accurate (1, 4, 5, 6, 8–11). Kornblum et al (1) reported a 71% accuracy rate in a series of 103 biopsies, and Murphy et al (9), who used a combination of aspiration and trephine technique, reported a 94% accuracy rate. Armstrong and Chalmers (10) reported a diagnostic yield of 68% in their aspiration biopsy series. DeSantos et al (11) achieved a 93% accuracy of biopsy findings of skeletal neoplasms. In a review of 120 bone biopsies Tehranzadeh et al (8) found an overall success rate of 72%. There were 70 (58%) true-positive results, 17 (14%) true-negative results, and 17 (14%) false-negative results; in 16 cases, the tissue was considered inadequate for diagnosis.
The major limitations of vertebral lesion biopsy are crushing and insufficent sample size. Intraprocedural trauma to the biopsy specimen was also the reason for our initial unsatisfactory results with the Ackermann needle. Although it was possible to identify malignant cells, tumor morphology was unrecognizable. Therefore, in the present series, we applied the larger bore (8-gauge) Jamshidi or Waldemar needle, which has a core cut of 3 mm compared with that of 1.5 mm for the Ackermann. This needle was sufficent to avoid crushing injury to the tissue. We were able to collect a precisely cut bone specimen within the lumen of the needle. The needle could be used for both lytic and sclerotic lesions. The transformation of the long anesthesia needle into a guidewire shortened the procedure and prevented the need for several insertion trials. To obtain two or three biopsies from a single lesion, we used a cannula of 5.2-mm diameter, so several biopsies could be retrieved via a single tract. This procedure proved to be practical and safe with both the Jamshidi and Waldemar needle sets. Of the 19 vertebral biopsies performed with this method, 11 (58%) results were true-positive, and eight (42%) were true-negative at a clinical follow-up of 12–60 months. The overall success rate was 100%.
Conclusion
Percutaneous vertebral biopsy is associated with a 0–26% rate of complications (1–9); the most frequently reported are pulmonary, neurologic, and infectious disorders. However, none of our patients had either immediate or long-term complications of the procedure. Two patients (10.5%) had excessive bleeding which was easily controlled by insertion of Gelfoam through the coaxial system. Bleeding is not considered a specific complication of this technique. The coaxial technique for CT-guided percutaneous biopsy of the spine has three advantages. First, intact specimens of adequate size can be obtained in most cases. Second, the use of the coaxial system enabled us to retrieve two or three biopsies through a single tract for better diagnosis. Third, the cannula can also be used to control bleeding in vascular lesions. We suggest that our system is more effective, reliable, safe, and rapid than the traditional technique.
References
- Received May 12, 2003.
- Accepted after revision May 23, 2003.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}