
Abstract
BACKGROUND AND PURPOSE: Colloid cysts of the third ventricle are rare benign brain tumors. The purpose of this study was to correlate their patterns on MR images with the probability of success of percutaneous treatment.
METHODS: Nineteen patients underwent endoscopic treatment for colloid cysts of the third ventricle. The cases were divided into two groups based on difficulty of the aspiration procedure. We reviewed CT scans and MR images and divided cysts into groups based on their signal intensity on the MR images and their density on CT scans. Intensity and density were correlated with difficulty of aspiration during the endoscopic procedure.
RESULTS: The aspiration procedure was difficult in 63% of the cases. Eighty-nine percent of hyperdense cysts on unenhanced axial CT scans were categorized as difficult, and 75% of hypodense cysts were categorized as easy. On T2-weighted MR sequences, 100% of low-signal cyst contents were difficult and nearly 63% of high-signal lesions were easy. There was a significant correlation between the T2-weighted sequences and the CT scans regarding the difficulty of the aspiration procedure.
CONCLUSION: T2-weighted MR sequences are useful for predicting difficulty of aspiration during stereotactic or endoscopic procedures. A T2-weighted low-signal cyst is correlated with high-viscosity intracystic contents.
Colloid cysts of the third ventricle are benign tumors that comprise approximately 1% of primary brain neoplasms. They are suspended to the anterior tela choroidea and contain a colloid substance of variable viscosity. The necessity of their treatment is widely admitted. The major factor that is predictive of difficulties during percutaneous procedures is the high viscosity of the cyst's content (1). Because colloid cysts are rare, there are few available reports of large patient series and few reports correlating MR imaging patterns with cyst viscosity (1, 2). Nineteen patients with anatomicopathologically proved colloid cysts of the third ventricle were treated at our institution by endoscopic procedure from December 1994 until June 1998. We correlated the pattern of colloid cysts on MR images and CT scans with the viscosity and the difficulty of the aspiration procedure.
Methods
Nineteen patients underwent endoscopic treatment for colloid cysts of the third ventricle between December 1994 and June 1998. There were 12 men and seven women (age range, 20–76 years; mean age, 40 years). The most frequent presenting symptom was intermittent headache (15 patients). Other less frequent symptoms included nausea (six patients), memory deficit (four patients), gait disturbance (four patients), mental status changes (four patients), blurred vision (three patients), coma (two patients), and seizure (one patient).
All procedures were performed by the same operator, using the same apparatus (Decq Neuroendoscope, Karl Storz GmbH & Co.; Tuttlingen, Germany). The procedure consisted of the introduction of the neuroendoscope through a burr hole into the lateral ventricle, initial puncture and manual aspiration with a Pury needle (external diameter, 5F), and opening of the cyst's wall with microscissors and forceps so that large aspirating probes could be used. We divided the cases into two groups: the easy group, in which the cyst was collapsed and mostly evacuated after initial aspiration; and the difficult group, in which initial aspiration produced a small amount of viscous material and failed to collapse the cyst.
MR imaging was performed with high field strength of 1.5 to 2 T in 18 cases and 0.5 T in one case. Of the 19 patients who were treated, all had undergone preoperative T1-weighted MR imaging (500–600/10/2 [TR/TE/excitations]) and 17 had undergone T2-weighted fast spin-echo imaging (2500–5000/90–100/1). Contrast-enhanced T1-weighted sequences were available for five patients. Appearance on MR images was described in terms of the signal intensity of the cyst's contents in reference to brain white matter. Among the 19 cases, preoperative unenhanced CT scans were available for 13 patients and contrast-enhanced CT scans for four. We reviewed the pattern of the cyst's content and considered it in reference to brain. The larger diameter of the cyst was noted in millimeters. Two neuroradiologists, who were unaware of the endoscopic aspiration procedure's level of difficulty, conducted analysis of the available MR images and CT scans. We retrospectively compared the signal on T2- and T1-weighted spin-echo images and the density of each cyst with the difficulty encountered during the endoscopic procedure.
Results
Results are summarized in Table 1. Nineteen patients underwent one endoscopic procedure each. One patient (patient 9) presented with a residual cyst of 12 mm after the first endoscopic procedure. Two years later, a second endoscopic operation failed to treat the residual cyst. There was no statistical difference (P = .42 by use of Student's t test) in terms of cyst size between the easy (22.6 ± 7.1 mm) and the difficult (21.6 ± 13.2 mm) groups. There were 12 (63%) difficult and seven (37%) easy aspirating procedures. In seven (36%) cases that were classified as difficult, aspiration procedures failed to produce any material, and cyst content was evacuated only after opening the wall with microscissors and using aspirating probes. See examples of scans and images in Figures 1 and 2.
Radiologic and surgical features
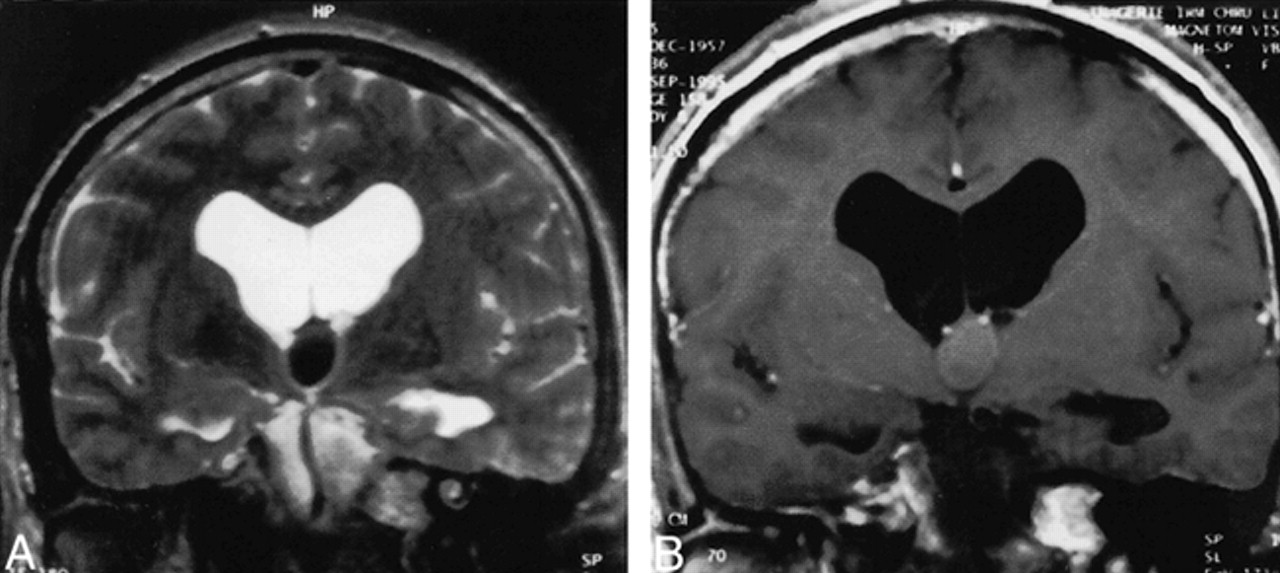
Patient 7.
A, Coronal T2-weighted sequence shows a very low-signal colloid cyst of the third ventricle, with obstruction of Monro's foramen.
B, High signal intensity can be seen on the T1-weighted sequence. Aspiration during the endoscopic procedure was difficult. The cyst's contents were evacuated after opening the cyst's wall by using larger aspirating probes.

Patient 8.
A, Axial T2-weighted sequence shows a high-signal colloid cyst of the third ventricle, obstructing Monro's foramina.
B, Axial T1-weighted sequence shows a low signal–intensity cyst.
C, Axial CT scan shows a hypodense cyst. Aspiration during endoscopic procedure was easy.
CT Scans
Among the 13 colloid cysts analyzed on unen-hanced CT scans, there were nine (69%) hyperdense, five (31%) hypodense, and no isodense lesions. Contrast-enhanced CT scans (n = 4) showed no enhancement in all cases, three of which were difficult and one of which was easy. Three (75%) of five hypodense colloid cysts were classified as easy at the time of aspiration, and eight (89%) of nine hyperdense lesions were difficult. We found a significant correlation between CT pattern and the aspiration procedure's difficulty (P < .1 by use of χ2 test). A hyperdense cyst was predictive of a difficult aspiration.
MR Imaging
On T1-weighted spin-echo sequences, 80% of low-signal cysts were easy, 100% of isosignal cysts were difficult, and 62.5% of high-signal cysts were difficult. There was no significant correlation between signal intensity of the cysts on the T1-weighted sequences and the difficulty of the aspiration procedure (χ2 test, P = .6). Available contrast-enhanced T1-weighted sequences (n = 5) showed no enhancement inside the cyst in all cases. In three of five cases, thin peripheral enhancement corresponding to septal veins was observed, one of which was easy and two of which were difficult. The other two cases showed no enhancement and were difficult. On T2-weighted sequences, all (100%) low-signal cysts were classified as difficult and 62.5% of the high-signal lesions were easy. We found a statistical correlation between the signal on T2-weighted sequences and the aspiration procedure (χ2 test, P = .02). The T2-weighted hyposignal pattern was predictive of a difficult aspiration procedure.
Discussion
A colloid cyst of the third ventricle can be symptomatic (increased intracranial pressure) or asymptomatic. The reported risk of sudden death (3, 4), however, has led to a widespread belief that all patients should be treated. Different neurosurgical techniques have been proposed: ie, simple shunting of both lateral ventricles, open surgical removal techniques, and percutaneous aspiration procedures (simple cyst aspiration, stereotactic aspiration, endoscopic procedure). The best surgical option has not been clearly determined. Because of the associated risks of epilepsy, venous infarction, and fornix damage (5–10, 11); however, many institutions reserve the open surgical technique for patients for whom percutaneous treatment has failed. The major factor that is predictive of difficulties during percutaneous procedures concerns the high viscosity of the cyst's content (1), which was correlated only with the hyperdense aspect on CT scans. Because percutaneous procedures are often performed when colloid cysts are discovered, we think that it is important to be able to predict through MR findings the difficulty they will present during percutaneous procedures because MR imaging offers a higher anatomic definition in a 3D space.
A review of the literature revealed two reports correlating the MR imaging pattern of the cyst's contents with its viscosity and difficulty of the aspiration procedure. Kondziolka and Lunsford (1) found a correlation between CT hyperdensity of the cyst and the high viscosity of its contents in 22 cases. In the same study, eight of 22 patients were evaluated with MR imaging and no correlation was found; however, the outcomes in all of the cases with low-signal cysts were unsuccessful. In our series, we found more low-signal cysts (nine of 17 available T2-weighted sequences), and all of them were difficult. The difference with our results may be explained because the small number of MR images obtained may make correlation difficult. Peragut et al (2) reported four cases of colloid cysts that were treated successfully by stereotactic aspiration, all of which appeared hyperintense on T2-weighted images. Wilms et al (12) reported five cases of colloid cysts that were treated surgically, with anatomicopathologic confirmation. On T2-weighted images, two had strong low signal surrounded by high signal and the other three were strongly hypointense. The low signal on T2-weighted sequences was related, by anatomicopathologic examination, to a viscous colloid slimy material that had the consistency of motor oil. The hypersignal peripheral rim was composed of amorphous material with presence of cellular debris, erythrocytes, and cholesterin clefts (12). This report seems to support the general belief that intracystic low signal on long-TR sequences is related to a high-viscosity material, indicating difficulties in aspiration procedure. Our series established correlation between intracystic low signal intensity on long-TR sequences and viscous or hard intracystic content, making the aspiration procedure very difficult or impossible. The significance of this low signal is still unclear. Maeder et al (13), in their attempt to correlate MR imaging and CT patterns with the cyst's chemical analysis, showed that increased CT density was not correlated with the presence of calcium or any metal but with high cholesterol contents. On MR images, they also correlated high signal on T1-weighted sequences with high cholesterol contents. Regarding T2-weighted sequences, they reported that strong intracystic low signal was not correlated with the presence of metallic paramagnetic elements or with recent or old hemorrhage. Kondziolka and Lunsford (1) correlated small cysts (<1 mL) with unsuccessful aspiration. Success in larger cysts was related to the viscosity of the cyst's contents rather than the cyst's size. The mean size of the cysts in our series was larger than 12.4 mm (ie, >1 mL in volume) and was equivalent in both difficult and easy cases (P = .42 by use of Student's t test). Therefore, success of aspiration was related to viscosity rather than cyst size. In our series, the pattern of the cyst's contents on CT scans was hyperdense in 69%, which is equivalent to the cases reported in the literature (approximately 70%). Our study also confirmed the correlation between hyperdense cysts and the difficulty of their aspiration during stereotactic procedures.
Conclusion
Previous studies failed to correlate the success of stereotactic aspiration with the MR imaging appearance of the cysts, very likely because of few patient series. The present study provides a significant correlation between low signal on T2-weighted fast spin-echo sequences and viscous (and therefore hard or impossible-to-evacuate) cysts. T2-weighted sequences are useful for predicting the difficulty of aspiration of colloid cysts during percutaneous procedures by either stereotactic aspiration or endoscopic techniques.
Footnotes
↵1 Address reprint requests to Carl El Khoury, MD, Service de Neuroradiologie.
References
- Received June 7, 1999.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}