
Abstract
BACKGROUND AND PURPOSE: Stenosis of the internal jugular, azygos, and other veins detected by using intracranial and neck Doppler and B-mode sonography and confirmed by venography has been reported in MS with a high degree of sensitivity. This article reports the results of sonographic findings in patients with MS and controls, looking for evidence of the controversial entity chronic cerebrospinal venous insufficiency. Furthermore, the venographic appearance in controls is documented.
MATERIALS AND METHODS: Thirty consecutive patients with definite MS and 10 controls had TCD and high-resolution Doppler sonography of the neck vessels by using the published sonography criteria of Zamboni et al. Those with 2 positive findings consented to undergo contrast digital subtraction venography for delineation of possible venous stenosis. Nine consecutive patients undergoing digital subtraction venography for petrosal venous sampling or parathormone sampling had images of their internal jugular veins obtained as part of their procedure, and they were assessed for stenosis.
RESULTS: No patient with MS or control had 2 positive sonographic findings; therefore, none were subjected to venography. Of the 9 controls undergoing venography for other reasons, 6 had bilateral IJV narrowing of ≥50%, and 2 others had unilateral narrowing.
CONCLUSIONS: No difference was detected between patients with MS and controls by using the objective sonographic criteria of Zamboni et al. Furthermore, normal physiologic narrowing is found very commonly in the internal jugular veins in healthy individuals. Nonblinded subjective sonographic assessment of the IJV may erroneously lead to venography, the findings of which may be misinterpreted due to the lack of widespread knowledge about the appearance of these veins in healthy individuals.
ABBREVIATIONS:
- CSA
- cross-sectional area
- ECD
- extracranial color Doppler sonography
- EDSS
- Expanded Disability Status Scale
- IJV
- internal jugular vein
- TCD
- transcranial Doppler sonography
Multiple sclerosis is an inflammatory disease of the central nervous system characterized by focal lymphocytic infiltration and demyelination. The cause is unknown, but the common hypothesis invoked is that environmental factors trigger the disease in individuals with complex genetic risk profiles.1 There is an increased migration of lymphocytes across a breach in the blood-brain barrier, triggering a cascade of events resulting in the development of an acute inflammatory demyelinating lesion.1,2 The close relationship of plaques to deep venous structures has long been observed3,4 and is demonstrable on MR imaging.5,6
A body of controversial literature suggesting an alternative etiology has arisen in the past 5 years stating that the insult triggering demyelination is secondary to impaired cerebrospinal venous return. This evokes venous hypertension, blood-brain barrier breakdown, hemosiderin deposition, and a secondary immune-mediated response with resultant demyelinating plaque.7,8 This has been termed “chronic cerebrospinal venous insufficiency”.9 The proponents of this theory have devised 5 sonographic criteria when studying the internal jugular veins, vertebral veins, and intracranial veins.9⇓–11 Two of these sonographic criteria being abnormal correlated very specifically in patients with MS and was not found in controls (P value <.0001). These patients then underwent venography and were found to have uni- or bilateral IJV stenosis >50% in 91% of cases and azygos abnormalities in 86%, whereas a control group without MS, who had normal sonography findings, underwent venography and had no venographic stenosis.9 There was 100% separation between patients without multiple sclerosis and those with the disease based on the sonographic criteria and venographic findings.
Furthermore, a registry of 65 patients treated predominantly by balloon angioplasty of the narrowed veins demonstrated improvement in their MS clinical outcome measures after treatment at 12 months, particularly in the relapsing-remitting form of the disease with a decrease in gadolinium-enhancing lesions seen on MR imaging.12 This however is comparable with the improvement seen with placebos in published double-blind controlled trials of MS therapy.13,14 Subsequent investigators have been unable to replicate the findings of Zamboni et al9 by using sonography15⇓⇓⇓–19 or MR imaging,20 with contradictory unsupportive data by using combined sonography and MRV imaging.21 Furthermore, 2 other studies with positive Zamboni criteria did not have venographic correlative stenoses in early-onset22 or long-standing MS.19 However the findings of Zamboni et al have been replicated by other groups,23⇓–25 and it has been suggested that special sonographic training is required.26 Finally, Simka et al24 published an article noting that 90% of patients with MS studied with sonography had 2 Zamboni criteria for chronic cerebrospinal venous insufficiency but in 2012, they reported that compared with venography, sonography is of limited value and the diagnosis is best made directly by venography.27
In view of the controversy, we undertook a nonblinded study selecting patients known to have MS and healthy controls for ECD and color TCD by using rigorous application of the original objective criteria of Zamboni et al.9 Any patients with 2 abnormal criteria would consent to undergo venography. In addition, as originally described by Zamboni et al,9 consecutive patients without MS who were undergoing retrograde IJV cannulation for parathyroid hormone or petrosal sinus sampling had formal venographic images of their IJV obtained. These images were compared with published images of patients reportedly with chronic cerebrospinal venous insufficiency.
Materials and Methods
Western Australia has a multiple sclerosis registry comprising >1000 patients, and an experienced neurologist2 selected consecutive patients on the basis of being seen in the clinic with availability, consent, typical MS phenotypes with an EDSS score of >3.5 MRI, and exclusion of any coexistent medical or surgical history. These patients were offered and consented to TCD and ECD assessment of the IJV and vertebral veins. The studies were conducted by 2 experienced sonographers3 (with >30 year's collective ECD and TCD experience) in conjunction with an experienced interventional neuroradiologist (with >15 years' ECD, TCD, and angiographic experience) by using the original criteria of Zamboni et al9:
Reflux in the IJVs and/or vertebral veins in sitting and supine postures (>.88 seconds)
Reflux in the deep cerebral veins (>.5 seconds)
High-resolution B-mode evidence of IJV stenoses and/or a CSA of the IJV in the supine position of <0.3 cm2
Flow not Doppler-detectable in the IJVs and/or vertebral veins
Paradoxical increase in the size of the CSA of the IJV when going from a supine to an erect position.
Ten volunteers also underwent ECD and TCD after informed consent was obtained. We used a 7.5-MHz linear vascular array transducer (Toshiba, Tokyo, Japan) for ECD and a 2-MHz sector array transducer (Toshiba) with color TCD, looking at the basal vein of Rosenthal, which appears to be the most likely structure demonstrated on previous studies. Direction of flow and reflux was analyzed. The images were obtained and were available on a PACS network. They were formally reviewed by the neuroradiologist. The sonographer's findings and the neuroradiologist's report were compared. If there was a discrepancy, the patient was recalled for consensus imaging with the sonographer and neuroradiologist both present.
Consecutive patients who were undergoing jugular cannulation and venography for petrosal sinus sampling or parathormone sampling of the IJV were studied for stenosis (≥50%) or the presence of bypass collaterals above a stenosis. Both are said to be important venographic findings in chronic cerebrospinal venous insufficiency.9
Results
Thirty consecutive patients were selected with typical MS phenotypes (17 women/13 men; mean age, 51.2 years; range, 26–70 years) with a mean disease duration of 13.4 years (range, 1–34 years). Five cases were relapsing-remitting (mean EDSS score, 3.3), 4 were primary-progressive (mean EDSS, 5.4), and 21 were secondary-progressive MS (mean EDSS score, 6.5). All had typical findings on MR imaging.
All 30 patients had ECD of the neck veins, and 18 consented to concomitant or interval TCD. Ten healthy volunteers were also studied (6 women/4 men; mean age, 37.4 years; range, 25–54 years) with TCD and ECD.
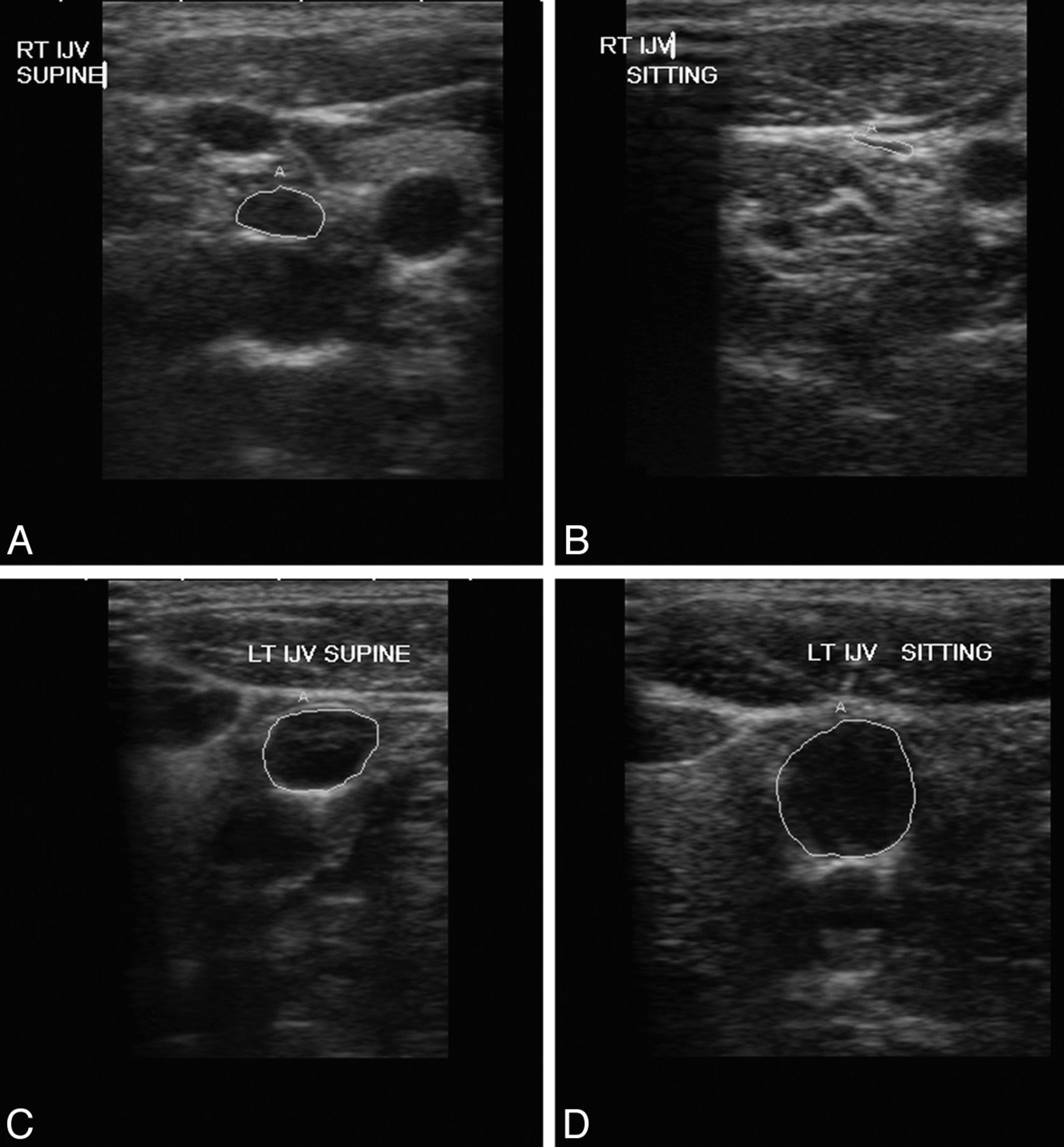
No single patient or volunteer had 2 abnormal findings, the stated requirement for a sonography-based diagnosis of chronic cerebrospinal venous insufficiency.9 Two volunteers had 1 abnormal finding of a CSA of the IJV <.3 cm2 in the supine position but without a paradoxical increase in the CSA in the erect position (Fig 1). One patient with secondary-progressive MS had a small paradoxical increase in the left CSA from the supine to the erect position, but nothing else (Fig 1). This patient also had TCD findings that were normal.

Transverse sonographic images of the right IJV in supine (A) and sitting (B) positions demonstrating appropriate reduction in the CSA in a healthy 29-year-old woman with a supine CSA of 0.29 cm2, an abnormal Zamboni criterion,9 decreasing to 0.04 cm2 in the sitting position. Transverse sonographic images of the left IJV in supine (C) and sitting (D) positions demonstrating a mild paradoxical increase in the CSA from 0.81 to 1.03 cm2 in a 70-year-old man with secondary-progressive MS for 9 years (EDSS score, 7). No other criteria of Zamboni et al9 were present on ECD or TCD.
Digital subtraction venography of 9 patients (8 women/1 man; mean age, 54.4 years; range, 44–67 years) undergoing parathormone (n = 7) or petrosal sinus sampling (n = 2) was studied. Fourteen of the 18 IJVs (77.8%) demonstrated stenosis of ≥50 (mean, 68.6%; range, 50%–95%), with 6 of these being accompanied by a collateral vein bypassing the narrowing. Six of 9 patients had bilateral stenosis; 2 others had unilateral stenosis. One had a 40% narrowing with a collateral vessel bypassing the narrowing. Representative examples are demonstrated (Figs 2⇓–4). These images are very similar to those published in chronic cerebrospinal venous insufficiency treatment articles.

Selective anteroposterior venography of the right IJV demonstrates a high-grade narrowing of the distal IJV (black arrow) with an associated large collateral vein. This patient is a 44-year-old woman without MS who was being investigated for hyperparathyroidism. These appearances are remarkably similar to those in Zamboni et al (Fig 5)12; Zamboni et al (Fig 2Bg)9; and Simka et al (Fig 3)40.

Selective anteroposterior venography of the right IJV. A, A 60-year-old female patient without MS being investigated for hyperparathyroidism. B, A 51-year-old man without MS being investigated for Cushing disease with petrosal sinus sampling. Both images demonstrate very high-grade narrowing of the distal IJV. Figure 3A is remarkably similar to Fig 2 in Ludyga et al,45 and 3B is very similar to Fig 2B (e and f) from Zamboni et al,9 Fig 2 from Simka et al40 and Fig 4A from Zamboni et al.12

Discussion
Chronic cerebrospinal venous insufficiency is an entity proposed to be associated with MS and said to be detected in 90% of patients with MS by the use of ECD and TCD as a screening tool,9,24 with promising treatment proposed by transvenous angioplasty or stent placement primarily of the IJV and, less often, the azygos vein.12,28 This treatment is reported to be performed with low morbidity as an outpatient procedure,29 with improvement in the patient's symptoms, though the restenosis rate in angioplasty of the IJV approaches 50% at 6 months.12
The sonographic data have been confirmed by some groups24,30 and are unable to be reproduced at all by others.15⇓⇓–18,31 MR imaging venographic data have been mixed, with the sonographic findings not being replicated.20,32 A combined sonography and MRV study21 was not able to replicate the findings in 40 patients with MS. A recent MR imaging study by Garaci et al33 demonstrated no significant specific interaction between the presence of chronic cerebrospinal venous insufficiency and MS in measured hemodynamic changes of mean transit time, cerebral blood flow, or volume.
We undertook a study with experienced vascular sonographers, a vascular interventional neuroradiologist, and an MS neurologist and were unable to find a single case on sonography fulfilling the criteria of Zamboni et al9 for chronic cerebrospinal venous insufficiency. Moreover, the number of positive sonographic findings was higher in a small healthy control group.
How is this so? Studying the criteria carefully, one finds the following:
A paradoxical increase in CSA of the vessel when changing posture
CSA <.3 cm2 in the supine position
Reflux lasting >.88 seconds
Deep cerebral vein reflux of >.5 seconds.
The above criteria are objective and relatively easy to perform. Nevertheless, the basis of these arbitrary values is, at best, sketchy.
Reflux of >.88 seconds being abnormal is a derived figure and arbitrarily determined by using a study looking at IJV insufficiency.15,34 The validity of this supposition has been questioned by others.15 Likewise, the figure of 0.5-second reflux in the deep cerebral veins being abnormal appears to be derived from lower limb varicose vein incompetence studies.35
Menegatti et al11 stated, “Stenosis of the IJVs with a CSA of 0.4 cm2 or less was measured by Lichtenstein et al.”36 This appears to be used as justification of the value of 0.3 cm2 being abnormal. In the original article by Lichtenstein,36 this finding was not described as an abnormality or stenosis but merely asymmetry in patients requiring central venous catheterization in an intensive care unit setting. The European Society of Neurosonology has published a position statement declaring that there is no scientifically sound validation for each of the 5 criteria quoted by Zamboni et al for the diagnosis of chronic cerebrospinal venous insufficiency.37
The problem of a lack of blinding of the sonographer in this area of research has been widely discussed.38 One of the subcriteria of Zamboni et al9 is high-resolution B-mode evidence of IJV stenosis. This allows very subjective analysis of the IJV and valvular morphology, and the literature on chronic cerebrospinal venous insufficiency is littered with descriptions of IJV valvular abnormalities,24,30 describing the presence of an inverted valve, a membranaceous or netlike septum, flap, immobility, annulus, double channels, anomalous orientation of the valve leaflets, or ectasia of the carotid bulb causing IJV narrowing.24,30,39 Sixty-seven percent of patients with MS have these abnormal subjective findings compared with 17.5% of healthy individuals; these are the most common sonographic abnormalities found.39 It has been suggested that special training is required26,39 to facilitate detection, and it would appear that these subjective valvular findings are a central tenet in the technique.
Simka et al27 subjected 58 patients with MS to ECD and catheter venography and concluded that ECD was relatively insensitive in detecting all venous abnormalities compared with a 92.2% incidence of IJV stenosis detected by venography and that the diagnosis of chronic cerebrospinal venous insufficiency should, therefore, rest with venography.
Simka et al40 published a large series on venography in 586 patients with MS demonstrating venous abnormalities in 64% of the right IJVs and 81.7% of the left IJVs. Stenosis of the IJV was demonstrated unilaterally or bilaterally in 59 of 65 patients with MS (91%) in the study of Zamboni et al,12 which is remarkably similar to the rate of IJV narrowing of ≥50% in our small series of 8/9 patients (88.9%) without MS.
Although IJVs are commonly accessed for central lines and interventional procedures, detailed knowledge of the normal diagnostic venographic appearance of the IJV and azygos system is limited. The anatomy is variable,41⇓⇓–44 and we hypothesize that any person subjected to venography is highly likely to have findings of apparent narrowing in these vessels. The reality is that any noninvasive test that purports to accurately differentiate patients with MS from those without MS on the basis of a supposed vascular stenosis will result in a “confirmatory” venogram, which may be misconstrued as detecting pathologically narrowed veins. This inevitably clears the way for endovascular treatment of this “abnormality.” The essential missing step is that the knowledge of the normal venographic appearance of the IJV and its tributaries is absent from the investigation and discussion.
The safety of endovascular angioplasty and, to a lesser extent, stent placement has been reported in the setting of chronic cerebrospinal venous insufficiency and MS,45 but the efficacy of treatment and the vascular pathogenesis on the basis of venous hypertension remains highly controversial.46 The overwhelming evidence is that it is unlikely that a thickened jugular valve is responsible for this disease; and the absence of MS in patients with dural fistula, radical neck dissection, idiopathic intracranial hypertension, and other known causes of significant venous hypertension has also been noted.46 Most important, the normal appearance of the head and neck veins needs to be widely disseminated to prevent inadvertent ascription of a pathologic process to these findings. The label of chronic cerebrospinal venous insufficiency as a medical condition needs to be questioned very closely.
Conclusions
We were unable to separate healthy controls from patients with MS on the basis of objective sonographic criteria specific for chronic cerebrospinal venous insufficiency. Furthermore, venography in 8 of 9 consecutive control patients demonstrated findings identical to those published in chronic cerebrospinal venous insufficiency articles claiming to be pathologically abnormal in patients with MS.
Acknowledgments
We thank sonographers Elvie Haluszkiewicz and Jacquie Saunders for their expertise and dedication.
Footnotes
Disclosures: Allan Kermode—UNRELATED: Consultancy: Bayer, Sanofi-Genzyme, CSL, Merck, Biogen-Idec, Novartis, Payment for Lectures (including service in Speakers Bureaus): Bayer, Sanofi-Genzyme, CSL, Merck, Biogen-Idec, Novartis, Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Bayer, Sanofi-Genzyme, CSL, Merck, Biogen-Idec, Novartis.
REFERENCES
- Received August 20, 2012.
- Accepted after revision September 17, 2012.
- © 2013 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.