
Abstract
BACKGROUND AND PURPOSE: Distal ACA aneurysms remain difficult to treat with endovascular therapy, but improved technology and experience allows for the treatment of some of these aneurysms with excellent results. The purpose of this study was to assess the status of endovascular treatment of distal ACA aneurysms by comparing our results with recent endovascular and microsurgical series of distal ACA aneurysms.
MATERIALS AND METHODS: Between 2000 and 2008, a total of 22 consecutive patients (14 women; mean age, 58.4 years) with distal ACA aneurysms underwent coil placement at Barrow Neurological Institute. Clinical presentations, radiographic findings, endovascular management, and outcomes were reviewed retrospectively.
RESULTS: Of the 22 patients, 13 (59%) presented with subarachnoid hemorrhage. Six patients were HH grade I or II, 1 was grade III, 5 were grade IV, and 1 was grade V. Frontal lobe hematomas occurred in 5 patients with ruptured aneurysms. The mean aneurysm size was 7.5 mm (range, 2.8–25 mm); 55% were smaller than 7 mm. Twelve aneurysms (55%) arose from the origin of the callosomarginal artery (55%). Complete occlusion was achieved in 50% of the cases and near-complete occlusion in 45%. The few periprocedural complications included 1 retroperitoneal hematoma and 1 intraoperative rupture. Four patients had thromboembolic events adequately treated intraprocedurally with abciximab. No deaths occurred in the patients treated.
CONCLUSIONS: The characteristics of the patients and aneurysms treated in our series were comparable to previous reports of endovascular treatment of ACA aneurysms with respect to rupture status. Periprocedural morbidity and mortality rates in our series fared well compared with previous reports, as did our combined rate of complete or near-complete occlusions. Recent advances in endovascular devices and techniques have improved outcomes of distal ACA aneurysms.
ABBREVIATIONS:
- ACA
- anterior cerebral artery
- GOS
- Glasgow Outcome Scale
- HH
- Hunt and Hess
- ICH
- intracerebral hematoma
- ISAT
- International Subarachnoid Aneurysm Trial
Across various series, distal ACA aneurysms have represented 2 to 9.2% of all intracranial aneurysms1⇓⇓⇓⇓–6 and comprised only 4.4% of the aneurysms in the ISAT.7 Bridging veins, attenuated arachnoid adhesions between the cingulate gyri, deep and narrow exposure of the interhemispheric fissure, adherence of the aneurysm dome to the parenchyma, high perioperative rupture rates, and difficulty in controlling the parent vessel have all been considered obstacles to the microsurgical management of these relatively uncommon lesions.8⇓⇓–11 Concomitantly, controlling the microcatheter in its distal vascular distribution and the small size of distal ACA aneurysms are difficulties associated with their endovascular treatment.12,13
We report our 8-year experience managing these lesions and compare our outcomes, focusing on periprocedural results, with those of recent endovascular series and with surgical series of patients with distal ACA aneurysms.
Materials and Methods
The medical records of patients with distal ACA aneurysms treated with endovascular techniques at the Barrow Neurological Institute were reviewed retrospectively for rupture status, clinical presentation, radiographic features, endovascular management, time to treatment, occlusion and recurrence rates, complications, and outcome at last follow-up. A 100% occlusion of the aneurysmal sac was considered complete. Near-complete occlusion was used for aneurysms judged to be 90% or more occluded as previously reported.14
We assessed functional outcome by using the GOS. A GOS ≥4 was considered favorable.
Analysis of Endovascular and Microsurgical Series of Distal ACA Aneurysms
We searched PubMed for endovascular and microsurgical series on both ruptured and unruptured distal ACA aneurysms containing well-reported patient data and detailed outcome assessments on the basis of either the GOS or the modified Rankin Scale. Surgical series that included lesions not managed with the operating microscope were excluded. We analyzed 6 series on the endovascular management of distal ACA aneurysms published since 2004 that had consistent and homogeneous results.10,13,15⇓⇓–18 When our series was added to these 6 reports, our assessment of the current status of endovascular coiling was based on 160 patients with distal ACA aneurysms (Table 1).
Demographics, outcomes, and mortality rates from 7 endovascular series of distal ACA aneurysms
The functional status of patients in 4 large series of microsurgical management of distal ACA aneurysms1,2,8,19 was compared with those in the endovascular series (Table 2).
Demographics, outcomes, and mortality rates from microsurgical clipping series of distal ACA aneurysms
Results
Between November 2000 and December 2008, a total of 22 patients (14 women, 8 men; mean age, 58.4 ± 13.3 years; age range, 32–87 years) with distal ACA aneurysms underwent endovascular coiling (Table 3). Thirteen patients (59.1%) presented with subarachnoid hemorrhage attributable to aneurysms of the distal ACA. The mean age of patients with ruptured aneurysms was 56.3 ± 14.0 years and that of patients with unruptured aneurysms was 61.3 ± 12.2 years (Table 4). The features of all aneurysms and associated aneurysms are shown in Table 5. Results from previous endovascular and surgical series of distal ACA aneurysms are tabulated in Tables 1 and 2, respectively.
Summary of clinical and radiologic data of 13 patients with ruptured distal ACA aneurysms undergoing coiling
Summary of clinical and radiologic data of 9 patients with unruptured distal ACA aneurysms undergoing coiling
Summary of characteristics of 22 distal ACA aneurysms
Ruptured Aneurysms
All 13 ruptured distal ACA aneurysms (Figs 1 and 2) were coiled within the first 4 days of hospitalization at our institution; 84.6% were coiled within the first 48 hours. At the end of the procedure, complete occlusion was observed in 7 patients and near-complete occlusion in 6 patients (Table 3). The mean length of hospitalization was 16.2 days (range, 4–34 days). Follow-up was limited and was considered a weakness of the study; of the 8 patients with additional follow-up after discharge, 7 (87.5%) had a favorable outcome at their last clinical consultation. Patients were observed for a mean of 12.5 months (range, 0–50 months).
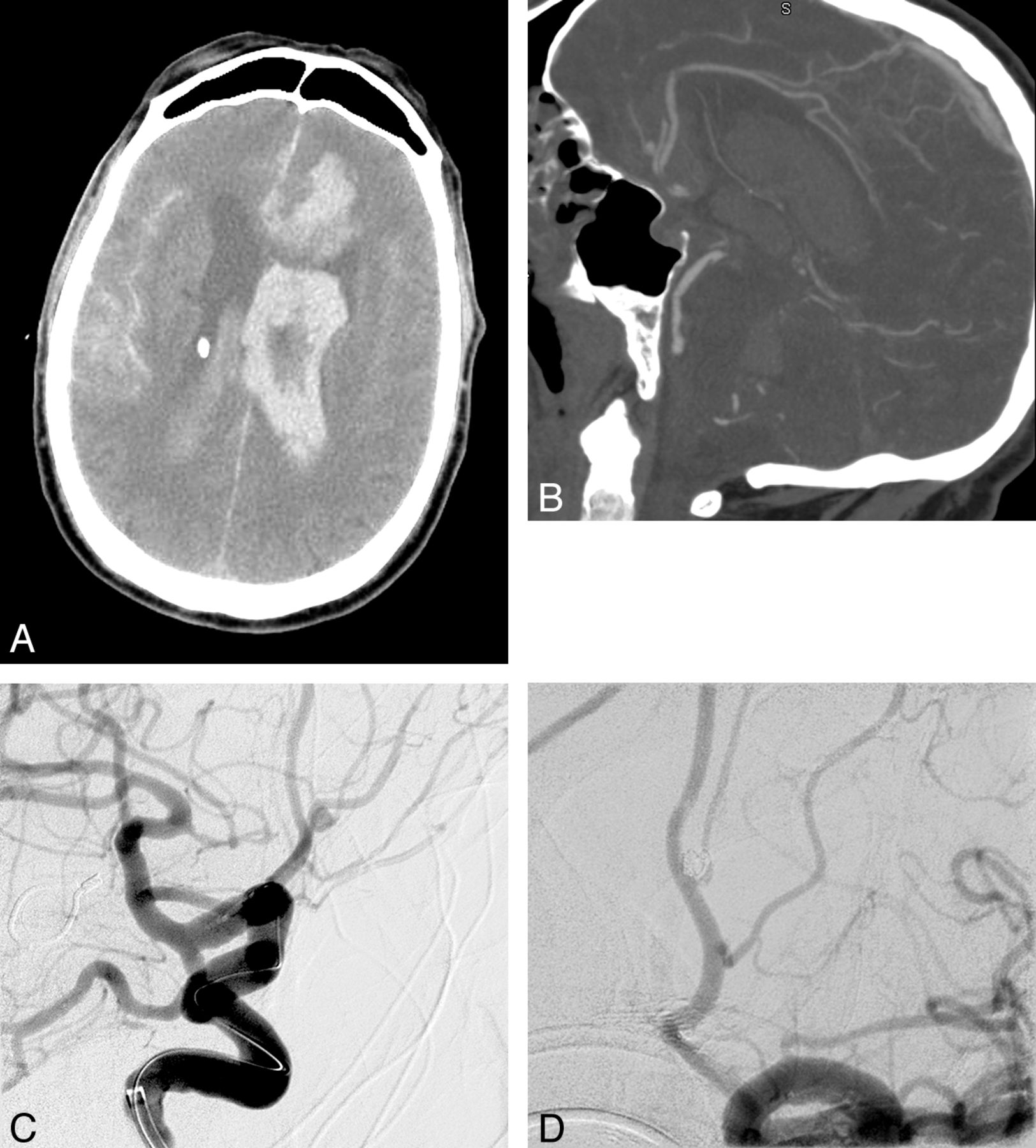
A, Initial CT scan of Patient 9 (Fisher grade IV). B, CT angiogram showed a 2.8-mm aneurysm. The patient underwent coil embolization. Preprocedural (C) and postprocedural (D) angiograms. Three coils were delivered. Complete occlusion was achieved. Used with permission from Barrow Neurological Institute.

A, Angiogram of a ruptured distal ACA aneurysm in Patient 12 reveals a 3-mm aneurysm arising from the A3 segment. B, Lateral view of a selective injection of the right pericallosal artery after coiling. The aneurysm was packed with 2 coils. Total occlusion was achieved. Used with permission from Barrow Neurological Institute.
Again, as for clinical follow-up, radiographic follow-up was limited, with angiography available for 7 patients, all of whom had a complete occlusion. Only 1 patient experienced a recurrence, which was discovered 4 months after treatment. The lesion was recoiled. A third intervention was necessary to address a second recurrence 3 years later. Follow-up angiography showed complete occlusion 1 year after that treatment. There were no cases of rebleeding in the limited follow-up period.
Unruptured Aneurysms
In 9 patients treated for unruptured aneurysms, complete occlusion was achieved in 4 patients (44.4%) and near-complete occlusion in 4 (Table 4). The patients were hospitalized for a mean of 4.6 days (range, 1–26 days) and were observed for a mean of 18.4 months (range, 1.5–62 months). At discharge, 7 patients (77.8%) had a GOS score of 5. Of the 9 patients, 8 had a GOS score of 5 at their last follow-up consultation, which again was of limited duration.
Angiographic follow up was limited and was available for 6 of the 9 patients. Five patients had completely occluded lesions; a sixth patient maintained a near-total occlusion. In 1 patient, aneurysm regrowth was observed on follow-up MR angiography 5 months after embolization (Fig 3). The lesion was again coiled, and complete occlusion was observed during a 5-year follow-up period.

Recurrence was observed in 2 of 13 patients who underwent follow-up angiography in our institution. Anteroposterior (A) and lateral (B) angiography at 5 months of a 69-year-old woman diagnosed with a 20-mm unruptured distal ACA aneurysm who underwent uneventful coiling. The aneurysm regrew after coil compaction to almost the initial size. Anteroposterior (C) and lateral (D) projections immediately after retreatment. Total occlusion was obtained. Used with permission from Barrow Neurological Institute.
Predictors of Outcome
As would be expected, a high HH score at hospital admission was associated with a significantly poor clinical outcome (P = .006, r = −0.562). No correlation was found between overall outcome and other predictive variables, including age, aneurysm size, intracerebral hemorrhage, and associated aneurysms, though the overall outcome at last follow-up was of limited duration. Periprocedural outcomes were excellent and included only 1 retroperitoneal hematoma and 1 intraoperative rupture. Four patients required abciximab infusion for thrombus formation, which developed during the procedure.
Discussion
Evolution of Endovascular Management of Distal ACA Aneurysms
In the 1990s, favorable results from centers experienced with microsurgical clipping, combined with the low incidence of distal ACA aneurysms, discouraged early referrals for endovascular care. Moreover, the peripheral location of distal ACA aneurysms and their small size precluded successful treatment by endovascular means with the use of developing technology.12,15 Pierot et al12 pioneered the endovascular management of 8 cases of distal ACA aneurysms in 1996, but embolization was successful in only 25%. Although based on a small series, Menovsky et al10 first proposed coiling distal ACA aneurysms as an alternative to clipping. Initial complete occlusion was obtained in 91.7% of their 12 cases. At last follow-up, 66.7% of the aneurysms remained completely occluded, no patient had again presented with bleeding, and 91.7% of the patients achieved a GOS score of 5 (Table 1). In a large microsurgical series primarily composed of patients with a good clinical grade, 83% of the patients with a ruptured distal ACA aneurysm had a favorable GOS score, and the mortality rate was 7.7% (Table 2).1 Although our follow-up was limited, periprocedural occlusion rates in our series compare well against historical controls. Of 22 patients, 11 (50%) experienced complete occlusion and another 10 (45%) had near-complete occlusion. Furthermore, there were no periprocedural deaths and only 1 instance each of intraprocedural rupture and retroperitoneal hematoma formation. Thromboembolic events were treated successfully with abciximab infusion in 4 patients.
Nguyen et al17 pointed out the caveat that the rate of intraprocedural rupture was higher when these lesions were coiled, compared with coiled aneurysms located elsewhere. They reported 3 perforations in 25 patients undergoing endovascular management of distal ACA aneurysms and suggested that the small size and distal distribution of the aneurysms could explain the high rate of rupture.17 Overall, in 7 endovascular series that enrolled 160 patients, including the current series, intraoperative rupture occurred in only 5.6%.10,13,15⇓⇓–18
Recurrences
Nguyen et al17 emphasized the recurrence rate of coiled distal ACA aneurysms, though the rate was not significantly higher than that for intracranial aneurysms coiled elsewhere. The cumulative rate of distal ACA aneurysm recurrence was 52.6%. A major recurrence, an event leading to retreatment, was observed in 21%. Pandey et al16 reported an 18% recurrence rate at a mean follow-up of 16.5 months. In a similar circumstance, Waldenberger et al15 identified a recurrence in 17.2% of patients at 6-month follow-up examination. Although it is difficult to draw strong conclusions on the basis of the length of follow up, we observed aneurysm regrowth in 2 patients (15.4%) at a mean follow-up of 15 months. Both of our patients underwent coiling again, and the aneurysms remained completely obliterated.
At a mean follow-up of 12.3 months, Raymond et al20 found recurrences in 33.6% of 381 intracranial aneurysms at various sites after endovascular treatment. They stressed that a main factor involved in recurrence, besides the initial occlusion rate and rupture, is the large size of an aneurysm (an infrequent feature of distal ACA aneurysms).20 Furthermore, the ISAT showed that the clinical implications of recurrences are unknown.7,21,22 For comparison, Tsutsumi et al23 found regrowth in 2.3% of 220 patients undergoing initial complete surgical obliteration of an intracranial aneurysm at a mean follow-up of 10 years. A review of 147 consecutive surgically treated aneurysms at our institution revealed a recurrence in 1.5% of completely obliterated aneurysms, but a regrowth occurred in 41.7% of those in which a neck remnant was observed on initial postoperative angiography.24 A neck remnant may lead to aneurysm regrowth, but its presence may not necessarily be indicative or predictive of an aneurysm that is unsecured or is more likely to rupture than a completely occluded aneurysm. The risk for subarachnoid hemorrhage from a neck remnant remains unclear.
Immediate Occlusion Rates in Microsurgical Series and Subsequent Rebleeds
In 1999, de Sousa et al1 observed an impressive 100% rate of complete occlusion on routine postoperative angiography after treating 74 distal ACA aneurysms with surgery, though their long-term follow-up was limited. Lehecka et al19 reported a satisfactory occlusion rate of 95% of 362 patients undergoing microsurgical treatment. In microsurgical clipping, recurrent subarachnoid hemorrhage can affect 2.7% of patients with complete occlusion of an intracranial aneurysm.23 An identical rebleed rate was found in 43 patients in a surgical series focusing specifically on distal ACA aneurysms.2 In a large series of 262 clipped distal ACA aneurysms, the rebleeding rate was only 0.4%.25 Although immediate complete occlusion with clipping occurs at an incredibly high rate, the rate of immediate occlusion with coiling, whether complete or near-complete, was more than 95% in this series and compared favorably with previous reports (Table 2).
Clinical Outcomes in Endovascular and Microsurgical Series, Focusing on Distal ACA Aneurysms
In 1999, Vanninen et al26 reported the first randomized prospective study comparing endovascular treatment of ruptured intracranial aneurysms with surgical clipping. A late analysis at 12 months showed no significant difference in the clinical outcomes of both groups managing ACA aneurysms, but the procedure-related mortality rate was higher among patients undergoing surgical clipping.
The endovascular group in the ISAT had better outcomes, even after 7 years of follow-up.27 However, this finding could not be generalized to a specific type of aneurysm such as distal ACA aneurysms.16,28
Studies have shown that the admission HH grade is a significant predictor of poor clinical outcome.8,15,16,19,29 Intracerebral hemorrhage on initial CT also predicted a poor outcome in patients undergoing either endovascular or microsurgical treatment of distal ACA aneurysms.8,15,19 The large number of distal ACA aneurysms surgically managed by Lehecka et al19 yielded a longer list of predictors. Intraventricular hemorrhage, severe preoperative hydrocephalus, age, and rebleeding before treatment were associated with unfavorable clinical outcomes in their series.
Periprocedural Morbidity and Mortality Rates
Endovascular management of ACA aneurysms was associated with a mean morbidity rate of 8.8% and ranged from 0%–17.2%.10,13,15⇓⇓–18 In 2 surgical series providing satisfactory data, the mean rate of morbidity among 405 patients was 14.3%.2,19 Finally, the mean mortality rate in patients with distal ACA aneurysms undergoing endovascular treatment was 8.8% in the assessed series, including ours, and ranged from 0%–20.7%.10,13,15⇓⇓–18 On analysis of only the cases of patients with ruptured aneurysms (n = 124), the mortality rate for endovascular treatment reached 11.3%. Overall, in 7 endovascular series that enrolled 160 patients, including the current series, intraoperative rupture occurred in only 5.6%.10,13,15⇓⇓–18
Conclusions
In our series, the periprocedural morbidity and mortality rates were similar to the risk profile of other reported series and demonstrate that these aneurysms can be treated safely by endovascular means. Recent advances in endovascular devices and techniques have improved treatment outcomes of distal ACA aneurysms, as seen in our series, with a favorable safety profile on the basis of analysis of periprocedural treatment success and complication rates.
Footnotes
Disclosures: Daniel Cavalcanti—UNRELATED: Employment: Paulo Niemeyer State Brain Hospital. Cameron McDougall—UNRELATED: Consultancy: Covidien, Gore.
REFERENCES
- Received June 13, 2012.
- Accepted after revision September 22, 2012.
- © 2013 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Treatment of Distal Anterior Cerebral Artery Aneurysms with Flow-Diverter Stents: A Single-Center Experience
- Use of flow diverters in the treatment of unruptured saccular aneurysms of the anterior cerebral artery
- Assessment of intracranial aneurysm rupture based on morphology parameters and anatomical locations
- Endovascular Treatment of Distal Anterior Cerebral Artery Aneurysms: Single-Center Experience and a Systematic Review