
Abstract
SUMMARY: In Part 1 of this review, the definition, terminology, and diagnosis of carotid near-occlusion were presented. Carotid near-occlusions (all types) showed a lower risk of stroke than other severe stenoses. However, emerging evidence suggests that the near-occlusion prognosis with full collapse (higher risk) differs from that without full collapse (lower risk). This systematic review presents what is known about carotid near-occlusion. In this second part, the foci are prognosis and treatment, pathophysiology, the current confusion about near-occlusion, and areas in need of future improvement.
ABBREVIATIONS:
- ARR
- absolute risk reduction
- CCA
- common carotid artery
- ECA
- external carotid artery
- PCA
- posterior cerebral artery
- ECST
- European Carotid Surgery Trial
Carotid near-occlusion is distal luminal collapse of the internal carotid artery beyond a tight stenosis.1 Please refer to the first part of this review for the literature review, definition, terminology, and diagnosis of carotid near-occlusion.2 Near-occlusion without full collapse seems to be commonly overlooked by some researchers and clinicians. Emerging evidence suggests a difference in prognosis, depending on the degree of collapse.3
The aim of Parts 1 and 2 of this review was to present the definition, terminology, diagnosis, prognosis, treatment, and pathophysiology of carotid near-occlusion; and highlight areas of confusion and those in need of future improvement. In this second part, the foci are prognosis and treatment, pathophysiology, the current confusion about near-occlusion, and areas in need of improvement.
Prognosis and Treatment
The NASCET and European Carotid Surgery Trial (ECST) included 246 cases of near-occlusion without full collapse and 16 cases of near-occlusion with full collapse.1 The cases with full collapse were few, and none had recurrent stroke, so all cases of near-occlusion were analyzed together. For near-occlusions randomized to medical treatment or surgery, the 3-year risk of ipsilateral stroke was 15.1% and 10.9%, respectively (absolute risk reduction [ARR], 4.2%; P = .33). In cases with 70%–99% stenosis without near-occlusion randomized to medical treatment or surgery, the 3-year risk of ipsilateral stroke was 26.0% and 8.2%, respectively (ARR, 17.8%; P < .001).1 The risk of perioperative stroke and death was similar for near-occlusion (5.4%; 8/148) and 70%–99% stenosis (6.2%; 36/581),4 and slightly lower periprocedural risks have been reported since then.5 Because 94% of near-occlusions were without full collapse, the findings from NASCET and ECST are mostly applicable to this group of near-occlusions.1 However, there was no indication that near-occlusion with full collapse differed.1
In 1983, Ringelstein et al6 concluded that “immediate diagnostic clarification and emergency endarterectomy are mandatory” for near-occlusion with full collapse, diagnosed with low-flow findings on continuous-wave Doppler. However, this opinion was not an observed high risk of recurrent stroke but was based on that of 9 patients: Two had crescendo TIA at baseline, 2 had crescendo amaurosis fugax at baseline, and 2 rapidly progressed to occlusion. In fact, no risk of recurrent stroke was reported.6 In 1989, O'Leary et al7 reported that of 9 patients with near-occlusion (most likely with full collapse) who did not undergo carotid endarterectomy, 2 had an angiographic stroke and 3 had a recurrent ipsilateral stroke within 1 year. Presumably, the angiographic strokes affected further management. Recently, in a small study of 10 cases with near-occlusion with full collapse, 4 (40%) had an ipsilateral ischemic stroke within 1 month of presentation, whereas none of 15 patients with near-occlusion without full collapse had recurrent stroke (P = .023).3
Even if near-occlusion with full collapse might show a high risk of recurrent stroke, the evidence level is poor. Indeed, because only approximately half (n ≈ 8) of the near-occlusions with full collapse were observed without an operation in NASCET and ECST, and Ringelstein et al6 did not report the risk of recurrent stroke, the risk of recurrent stroke without or before carotid endarterectomy has only been reported for approximately 27 patients.1,3,7 Of these, 26% (7/27; 95% CI, 8%–44%) had a recurrent stroke within 1 year—ie, roughly equal to the 3-year risk of 70%–99% stenoses (but with a wide margin of error). If anything, 26% might be an underestimation because some were not followed for a full year and some were not followed from the presenting event. This high risk was not observed in NASCET and ECST, possibly because of the long delay between the last event and the study entry (an overall delay of >4 weeks in >50% of cases),1 whereas a recent study found that all recurrent strokes occurred within 4 weeks.3
Asymptomatic near-occlusion prognosis has not been studied. Some near-occlusion cases without full collapse were likely, but unintentionally, included in the Asymptomatic Carotid Surgery Trial.8 In this trial, the diagnosis of carotid stenosis was mostly made with sonography, which cannot distinguish carotid stenosis and near-occlusion without full collapse. Because near-occlusions were not identified, they were not separately analyzed.
Pathophysiology
Nature of Near-Occlusion.
A few studies shed light on the nature of near-occlusion:
Conventional stenoses can progress to near-occlusion.1
Intraoperative back pressure is higher in cases of near-occlusion with full collapse (mean, 56 ± 15 mm Hg) than for those with conventional stenosis (mean, 33 ± 13 mm Hg).9
Flow velocities are high in near-occlusion without full collapse and can be high or low in near-occlusion with full collapse.3,10⇓–12
Collaterals reaching the ipsilateral MCA via the anterior communicating artery, posterior communicating artery, and/or the ophthalmic artery on conventional angiography are present in 64%, 43%, 25%, and <5% in cases with near-occlusion (with and without full collapse), with 85%–99% stenosis, 70%–84% stenosis, and <70% stenosis respectively.13 Any flow in intracranial collaterals has been reported in 96% of cases with near-occlusion (with and without full collapse).14
Both CBF and SPECT blood flow reactions to acetazolamide are lower among patients with near-occlusion (likely with full collapse alone) than in both patients with 70%–99% stenoses and disease-free controls.15 Before carotid stenting, 20% (3/15) of those with near-occlusions had >10% blood flow increase with acetazolamide; after carotid stenting, 100% (15/15) had >10% increase.15 Some studies included measurements of intracerebral hemodynamics, without analyzing them in detail.16⇓⇓–19
Near-occlusion with full collapse (diagnosed with low-flow velocities on sonography) and high-grade stenosis cause similar infarction patterns with approximately half of patients having infarctions in watershed areas, though occlusions often have large territorial infarctions.20
Some near-occlusions looked similar to conventional stenoses histologically, whereas some were actually recanalized thrombotic occlusions.21 However, the underlying study included both symptomatic and asymptomatic near-occlusions with a mean interval between the last symptom and surgery of 2.2 months.21
A theoretic model presented by Spencer and Reid22 noted that if a stenosis is sufficiently severe, incurring a large pressure drop, the flow from intracranial collaterals will create back pressure. With a sufficiently large pressure difference, the flow through the stenosis will decrease and the artery will collapse. Because stenoses can progress to near-occlusion,1 cases with near-occlusion have high back pressures9 and visible collaterals.13,14 When flow is poised to reduce, the flow velocities are still high, as seen in cases without full collapse having high flow velocities.3,10 This model seems robust in vivo and may explain varying sonographic findings in near-occlusion.
Usable circle of Willis and/or external carotid collaterals should exist for developing near-occlusion, though some individuals may not have usable collaterals.23 It may be that without intracranial collaterals, near-occlusion may not develop when stenosis progresses; rather, hemodynamic strokes may occur instead. No report examined this possibility, to our knowledge.
The diagnosis of near-occlusion is more difficult in cases with contralateral disease.2,24 However, the impact of contralateral disease on collateral use and prognosis has not been studied.
True hypoplasia is rare, between 0.01% and 0.24%.25⇓–27 Most cases of near-occlusion show true artery collapse with a reduced outer diameter, and it inflates after the stenosis is removed.9 However, on CTA, the cross-section of the carotid canal can look like “an island in a lake” or a “small brook in a large river bed” in cases of near-occlusion with full collapse (Fig 1). In contrast, true ICA hypoplasia is seen as a thin artery with a thin bony canal on CTA (Fig 1), without prominent ICA bulb stenosis.
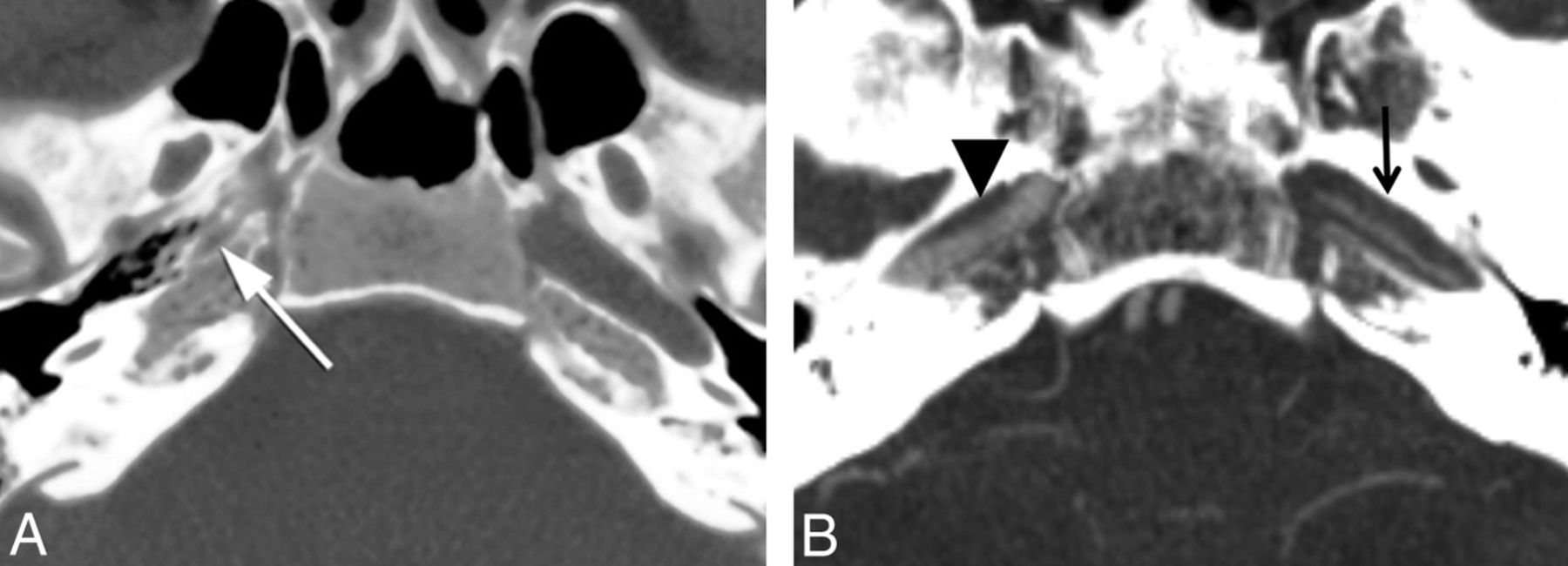
Comparison of bony carotid canals with ICA hypoplasia and near-occlusion. A, A case of right ICA hypoplasia. A narrow bony carotid canal (white arrow)—smaller than that on the contralateral side. Reprinted with permission from Ibrahim et al.58 B, A case of left near-occlusion with full collapse. The narrow left ICA (black arrow) is in a normal-sized bone channel—“a small brook in a large river bed.” Bone channels are similar on the left (black arrow) and right (black arrowhead).
Mechanism behind Recurrent Strokes.
Near-occlusion with full collapse might cause a high risk of recurrent stroke.1,3,7 If confirmed, by what mechanism can near-occlusion with full collapse cause the observed higher stroke risk? It has been reported that untreated near-occlusions often progress to occlusion.7 However, a recent article found that none of 4 fully collapsed near-occlusions progressed to occlusion when examined after presumed embolic recurrent stroke.3 Other pathophysiologic mechanisms of near-occlusion with and without full collapse have not been studied. Both hemodynamic and embolic mechanisms are reasonable for the possible high risk of stroke among patients with symptomatic near-occlusion with full collapse.
As near-occlusion progresses from without-to-full collapse, the ipsilateral hemisphere receives less from its carotid artery and more from collaterals. Patients with near-occlusion with full collapse show compromised cerebral hemodynamics15; it is reasonable to suspect a hemodynamic mechanism for recurrent strokes. The presence or absence of systemic hypotension at the time of recurrence was not analyzed in previous studies.1,3,7
Severe flow reduction of near-occlusion with full collapse stimulates blood stagnation with presumed increased risk of thrombus formation, leading to embolic risk from the ICA bifurcation up to the first good intracranial collateral. Comparably, ischemic events from embolic mechanisms were seen for 3% of cases undergoing balloon occlusion for unclippable aneurysms.28 Such embolic risk seems greatest before thrombus organization, likely a short-lived phenomenon. Most stroke recurrences occurred early (within 1 month),1,3,7 indicating a short-lived stroke-risk increase followed by stability, supporting the embolic mechanism. Even though reduced flow may lower embolic transportation in near-occlusion, full-collapse cases might still be at increased risk of embolic strokes overall from increased thrombus formation. Indeed, some near-occlusions are likely recanalized thrombotic occlusions.21
Confusion about Near-Occlusion
In Part 1 of this review, we presented the terminology, definition, and diagnosis of near-occlusion.2 Because some of the confusion in terminology definition and diagnosis is interwoven with prognosis, treatment, and pathophysiology, all issues are presented here.
Terminology and Definition.
The multitude of terms for near-occlusion and their interchangeable use may contribute to confusion. The expanded near-occlusion definition, including subtle collapse in NASCET,14 was not recognized by all. “Near-occlusion” was used interchangeably with the “string sign” (or similar variations), even though the “string sign” (full collapse) is a subset of near-occlusion.
Near-occlusion without full collapse continues to be ignored, unknown by many. Existing guidelines do not clearly acknowledge this diagnosis.29,30 Educational articles,31,32 reviews,33 editorials,34,35 and book chapters36 do not acknowledge this diagnosis (with few exceptions).37,38 Without recognition, incorrect calculations for NASCET percentage stenosis are performed for near-occlusion without full collapse. In addition, near-occlusion without full collapse is the natural intermediate step between severe stenosis with normal-caliber ICA beyond it and near-occlusion with full collapse. Yet near-occlusion without full collapse is well documented—but ignored. Many authors10,16,34,39⇓⇓⇓–43 have cited outcomes of near-occlusions with full collapse from the 1997 NASCET article14 as the outcome of all near-occlusions, without mention or explanation of those without full collapse. In contrast, fewer correctly made this distinction when citing that article.17,18
In some articles, terms for near-occlusion (“pseudo-occlusion” and “string sign”) were used differently from those for severe atherosclerotic stenosis, and clearly for another entity.44⇓⇓⇓⇓⇓⇓⇓⇓–53 However, in other articles, terms for near-occlusion have been used inappropriately by also including carotid stenoses without distal collapse in the term but without clarification that something else was intended; rather the findings were directly compared with those in near-occlusion studies,42,54 or the article was educational without references.31 Specifically, with high-flow velocities on sonography, many high-grade conventional stenoses can be called “near-total occlusion.”42 In 2 articles, threadlike stenosis without distal collapse was called the “string sign.”54,31
Diagnosis.
Near-occlusion should be listed as “near-occlusion,” not as a “percentage stenosis.” Suggestions that the contralateral ICA be used as a denominator when the ipsilateral ICA is collapsed, creating tight percentage stenosis,55 seem an extraordinary devotion to percentage stenosis without recognizing the reality of near-occlusion. The prognosis of part-near-occlusion seems to differ from that in severe stenosis1; using the contralateral ICA as a denominator for percentage seems inappropriate. Some argued that the NASCET method is fallacious because the distal artery can collapse,56 though this argument ignores the fact that NASCET called for recognition of near-occlusions and requested that such stenoses not be graded with percentages.37 Those who do otherwise are not performing the NASCET grading as recommended. It is important to exclude distal artery collapse before grading a carotid stenosis; subtle collapses can be overlooked and not identified as near-occlusion if not actively sought consistently. If you do not seek it, you will not find it.
Prognosis and Treatment.
Smaller studies,6,7 before NASCET and ECST, suggested that near-occlusions with full collapse have a high risk of stroke; this suggestion was negated by NASCET and ECST.1 However, NASCET and ECST mostly included near-occlusion without full collapse. Recently suggested are relevant differences of short-term prognosis between symptomatic near-occlusion with and without full collapse,3 differing from previous knowledge,1 with symptomatic near-occlusion without full collapse associated with a lower risk of recurrent stroke. However, symptomatic near-occlusion with full collapse is rarely studied, with conflicting results; it could have a high risk of recurrent stroke,1,3,6,7 which was not picked up by NASCET and ECST. After all, those studies were both randomized trials requiring patients to be acceptable candidates for both medical and surgical treatment arms, the equipoise requirement for a randomized treatment trial. In the late 1980s and early 1990s, few cases with fully collapsed ICA beyond a bulb stenosis would have been randomized.
Need for Future Improvement
Near-occlusion without full collapse needs recognition for future studies, guidelines, and clinical practice. Many seem unaware of this diagnostic category. As a result, patients can presumably be misdiagnosed as having conventional carotid stenosis, even nonsignificant stenosis, severely affecting management. Current guidelines simply state that near-occlusion has a low risk of stroke.29,30 Awareness of near-occlusion with only full collapse will not pick up partial near-occlusion. Guidelines should be revised to highlight the 2 types of near-occlusion, that near-occlusion without full collapse has been well-studied but misunderstood by many, and that only this type may have a lower risk of stroke. On the other hand, near-occlusion with full collapse is widely known, but its real stroke risk is less known.
Further studies of symptomatic near-occlusion prognosis with full collapse are warranted. Some small studies suggest a high risk of recurrent stroke,3,7 despite being thought of as low.1 If this high risk is further documented, a randomized trial is warranted.
Several Other Areas for Improvement.
More high-quality studies comparing sonography, CTA, and MR imaging with conventional angiography are warranted.
Sonography, common as the first and often only carotid imaging, cannot distinguish near-occlusion without full collapse from conventional stenosis with peak systolic velocity analyzed. Other velocity or diameter measurements or both need analysis.
A small sonographic study reported how often different pathologic flow profiles indicate distal occlusion or near-occlusion in situ.57 This should be reproduced.
The value of contrast-enhanced sonography to better distinguish near-occlusion from occlusion should be evaluated.
The prognosis of asymptomatic near-occlusion is unknown.
It is not well worked out if the mechanism for recurrent strokes in patients with near-occlusion with and without full collapse is predominantly hemodynamic or predominantly embolic.
Footnotes
Disclosures: Elias Johansson—RELATED: Grant: Several smaller stroke funds contributed, with funding listed in the footnotes*; none had any influence on the content. Conforms to “no disclosures.” Allan J. Fox—UNRELATED: Expert Testimony: medical malpractice suits, none relevant to the topic of this work. *Money paid to the institution.
This work was funded by the Swedish Stroke Foundation, the Northern Swedish Stroke Fund, the foundation for neuroscientific research at Umeå University Hospital, the County of Västerbotten, and the Medical Faculty of Umeå University.
Indicates open access to non-subscribers at www.ajnr.org
References
- © 2016 by American Journal of Neuroradiology





{kind=link}
Jump to section
Related Articles
Cited By...
- Cerebral blood flow pattern in patients with carotid artery stenosis with low trans-stenotic blood flow
- Comparison of 30-Day Outcomes after Carotid Artery Stenting in Patients with Near-Occlusion and Severe Stenosis: A Propensity Score Matching Analysis
- Diagnosing Carotid Near-Occlusion with Phase-Contrast MRI