
Abstract
BACKGROUND AND PURPOSE: Perfusion imaging with dynamic susceptibility contrast MR imaging (DSC-MRI) has been used to evaluate hemodynamic status in patients with symptomatic occlusive cerebrovascular disease. The aim of the present study was to determine the hemodynamic changes occurring in asymptomatic patients with unilateral internal carotid artery (ICA) occlusion by use of DSC-MRI with transcranial Doppler (TCD) measurement of the breath-holding index (BHI).
METHODS: Nine patients with asymptomatic unilateral ICA occlusion underwent DSC-MRI and TCD examination. One patient was excluded from final analysis because of severe movement artifacts. On a separate workstation, regional cerebral blood volume (rCBV), regional cerebral blood flow (rCBF), and regional mean time to peak (rMTT) were calculated on the basis of signal decay rate during the passage of gadolinium bolus through the sampled volume in the territory of the middle cerebral artery. TCD-BHI was calculated in all patients. Six healthy subjects underwent the same MR protocol as the patients.
RESULTS: Compared with control subjects, patients with unilateral ICA occlusions had hemodynamic changes in the ipsilateral hemisphere: rCBF was significantly lower than in controls (P < .01), and r MTT was significantly increased in both white (WM) and gray matter (GM) in the affected side (WM: P < .01; GM: P < .05). No statistically significant difference in rCBV was found in the group of patients (occluded versus contralateral, P < .1) or between the patient and control groups (occluded side versus controls, P < .1). The correlation of rCBV and BHI showed a strong relation of the two variables, showing a decrease of the latter when the former increased.
CONCLUSION: DSC-MRI is a valuable tool for measuring hemodynamic changes in the presence of carotid disease with hemodynamic impairment. In our opinion, hemodynamic changes and efficiency of collateral pathways can be evaluated in occlusive carotid disease by using paired measurement of BHI and DSC-MRI. In the patient group, MR-determined rCBV and TCD-determined BHI showed a significant inverse correlation, suggesting similar significance of the two indices.
The predictive significance of internal carotid artery (ICA) occlusion in determining ischemic stroke is controversial. The annual stroke rate in patients with carotid occlusion ranges from 0% to 20.1% (1, 2). Different pathogenic mechanisms responsible for ischemic stroke in patients with ICA occlusion have been evoked, and the best therapeutic strategies in patients with carotid occlusive disease is still controversial. Follow-up studies indicate that the risk of cerebral infarction increases significantly in patients with impaired cerebral hemodynamics. Assessment of cerebral hemodynamics can be performed with different techniques.
Dynamic susceptibility contrast MR imaging (DSC-MRI) is a promising technique to investigate cerebral hemodynamics. MR imaging is usually more available than positron emission tomography (PET) and has a higher spatial resolution than other neuroimaging techniques, such as single-photon emission CT (SPECT) or PET itself (3, 4). Moreover, DSC-MRI does not entail exposure to ionizing radiation or the complexities of administration of contrast media that affect xenon CT (5).
The ability to detect changes in the homogeneity of local magnetic fields during the passage of a compact bolus of gadolinium, which causes a drop in signal intensity, provides information about the pattern of brain perfusion in the microvascular bed.
Transcranial Doppler sonography (TCD) allows for rapid investigation of flow velocities in the large cerebral arteries and of velocity changes after a vasodilatory stimulus such as acetazolamide, CO2, or apnea. Such changes, named cerebrovascular reactivity, are considered an index of the capability of adaptive changes in CBF and can be reduced or exhausted in patients with carotid occlusive disease (6). The aim of our study was to correlate the findings of TCD with breath-holding index calculation (BHI) with regional brain perfusion assessed by DSC-MRI in patients with unilateral internal carotid occlusion.
Methods
Nine patients (seven men and two women; mean age, 69 ± 3 years) with asymptomatic occlusion of the ICA and without significant stenosis of the contralateral ICA were enrolled in this study. The patients were selected among those undergoing sonographic examination in the outpatient department and referred by their general practitioner for suspected carotid stenosis. All selected patients underwent a careful neurologic and cardiologic examination, electrocardiography, transthoracic echocardiography, and brain CT. Two patients underwent digital subtraction angiography with arch injection, and seven MR angiography using a 3D fast field echo sequence
(4.3/1.4/1 [TR/TE/excitation]; flip angle, 40°; matrix, 512 × 256/250, effective slice thickness, 1 mm; number of slices, 40; key-hole percentage, 50%) with injection of a double dose of gadopentate dimeglumine (Gd-DTPA) (0.2 mmol/kg) by means of a power injector at the rate of 3 mL/s, followed by a 20-mL saline solution flush. Five dynamic acquisitions were acquired every 7 seconds. Time-of-flight technique was used for intracranial vasculature (30/6.9/1; flip angle, 20°; matrix, 512 × 512; slices, 180). Complete blood work and a clinical history with particular attention to the major vascular risk factors (hypertension, diabetes, smoking, and hyperlipidemia) were obtained from each patient.
Six age-matched, healthy control subjects were also included after excluding hemodynamically significant carotid disease or other significant neurologic disease. The control subjects underwent the same MR imaging protocol. Under control of the ethics committee, volunteers agreed to participate after being instructed of the possible risk related to the IV injection of contrast media and exposure to radiofrequency and magnetic fields.
The study was approved by the local ethics committee, and each participant gave informed written consent.
MR Imaging Study
Perfusion studies were performed on an MR system operating at 1.5 T with a standard, circularly polarized head coil and a gradient strength of 25 mT/m with sinusoidal profile. A turbo spin-echo T2-weighted sequence was first performed in the axial plane (3800/22 [TR/TE]) to exclude patients with territorial or border zone infarcts. DSC-MRI studies were then performed using an echo-planar sequence (0.8/54) to obtain a series of DSC T2*-weighted images acquired during the passage of a bolus of Gd-DTPA in the cerebral microvascular bed. Five images (7 mm thick with 3.5-mm gap) were positioned on a sagittal scout along the anterior commissure-posterior commissure plane for coverage of the parenchyma from the middle cranial fossa to the centrum semiovalis. One hundred volumes were performed at a rate of 1/s. A dose of 0.2 mmol/kg of paramagnetic contrast medium was injected in a compact bolus via an antecubital vein in 5 seconds through an 18-gauge IV line. The injection was timed to the scanner, and usually began after the 10th acquisition was completed, and lasted to the end of the 15th acquisition.
MR Image Analysis
Head movement during MR data acquisition was controlled by visual inspection (rapid scroll of the images). Owing to the presence of major (> 1 mm) movement artifacts, one patient was excluded from further evaluation. Square regions of interest (ROI) of 4 × 4 pixels (1-mm pixel size) were drawn on the precontrast images and automatically repeated on all the images of the time series, in the same position. The ROI were drawn within the vascular territory of the middle cerebral artery (MCA) and the border zone territory between the anterior cerebral artery and MCA in both hemispheres, in corresponding specular position within both gray (GM) and white matter (WM). The territorial boundaries were drawn according to Hupperts et al (7).
For each ROI, signal intensity time series were generated. Upon arrival of the gadolinium bolus in the tissue, these time series exhibited a change in signal intensity due to change in the apparent spin-spin relaxation rate, R2*. The signal intensity, S(t) is proportional to the concentration of the contrast agent in the tissue, C(t) (8–10):  where S0 is the baseline signal intensity (ie, before injection of the gadolinium bolus) and k is a proportionality constant that depends on the magnetic field strength and the pulse sequence. Thus, the signal intensity time series could be converted into concentration time series. In particular, S0 was determined by averaging of the first time points, and baseline correction was performed after conversion of the signal intensity curves into concentration curves by linear interpolation between the start- and end-points of the peak concentration. Subsequently, the regional cerebral blood volume (rCBV) was calculated:
where S0 is the baseline signal intensity (ie, before injection of the gadolinium bolus) and k is a proportionality constant that depends on the magnetic field strength and the pulse sequence. Thus, the signal intensity time series could be converted into concentration time series. In particular, S0 was determined by averaging of the first time points, and baseline correction was performed after conversion of the signal intensity curves into concentration curves by linear interpolation between the start- and end-points of the peak concentration. Subsequently, the regional cerebral blood volume (rCBV) was calculated:  while the mean time to peak (MTT) was obtained by:
while the mean time to peak (MTT) was obtained by:  (11, 12). Finally the regional cerebral blood flow (rCBF) was calculated as:
(11, 12). Finally the regional cerebral blood flow (rCBF) was calculated as:  All variables (rCBV, MTT, and rCBF) were calculated by numerical integration. MTT was expressed in seconds, while rCBV and rCBF were expressed in arbitrary units. The recirculation of contrast media was not corrected and was not considered a major factor influencing the results.
All variables (rCBV, MTT, and rCBF) were calculated by numerical integration. MTT was expressed in seconds, while rCBV and rCBF were expressed in arbitrary units. The recirculation of contrast media was not corrected and was not considered a major factor influencing the results.
A paired Student's t test (using Bonferroni correction for multiple comparisons) was performed to assess hemispheric differences between the occluded and contralateral side. Linear regression analysis was performed to assess the relation between the BHI measured by TCD and the variables exhibiting the largest interhemispheric difference. For each variable, rCBV, MTT, and rCBF, one-way analysis of variance was performed to assess differences between healthy tissue and the contralateral and occluded sides in the GM and WM. An image processing and analysis software (MedX; Sensor Systems, Hernden, VA) and Excel 97 (Microsoft; Bellview Redmond, WA) were used for data analysis.
Transcranial Doppler Study
Carotid artery disease was assessed and defined by color flow b-mode Doppler sonography according to validated criteria (13). Intracranial vessels were examined by means of a Multidop X/TCD instrument. Examination of vessels of the circle of Willis was performed as described by Aaslid et al (14). The patency of major collateral vessels, the ophthalmic artery and anterior and posterior communicating arteries, was evaluated by means of compression tests (15).
All subjects underwent TCD evaluation of cerebrovascular reactivity to apnea. Two dual 2-MHz transducers fitted on a headband and placed on the temporal bone windows were used to obtain a bilateral continuous measurement of mean flow velocity (MFV) in the MCAs. Cerebrovascular reactivity to hypercapnia was evaluated by means of the BHI (16). The index was obtained by dividing the percent increase in MFV occurring during breath-holding by the length of time (seconds) that subjects held their breath after a normal inspiration: ([MFV at the end of breath-holding − rest MFV/ rest MFV] × 100/seconds of breath-holding). End-tidal expiratory CO2 was measured by means of a respiratory activity monitor. All subjects were normocapnic. The study was performed in a quiet room, with subjects lying in a comfortable supine position, without any visual or auditory stimulation. The same two operators who were unaware of the subjects' clinical status and the results of the extracranial carotid studies performed evaluation of coronary vascular resistance in the early morning. MFV and end-tidal CO2 at rest were obtained by the continuous recording of a 2-minute period of normal room air breathing. During the same period, mean blood pressure (MBP) and heart rate (HR) were continuously monitored by means of a blood pressure monitor. After a breath-holding period, MFV, MBP, and HR were recorded over a 4-second interval. Subjects were asked to hold their breath for 30 seconds after a normal inspiration. All subjects were able to hold their breath for the required period. Before proceeding to the definitive recording, subjects were trained to perform the procedure correctly. End-tidal CO2 changes from baseline to the first expiration after breath-holding were very similar in all the study subjects (end-tidal CO2 values during normal breathing: 36.5 ± 3.4 mm Hg; at the end of the apnea period: 46 ± 3.1 mm Hg). The exact length of apnea was checked and ranged from 29.7 to 30.3. Changes in HR and MBP after the apnea period were slight: 2%–4% for HR and 3%–5% for MBP. This method of induction of hypercapnia was effective and provided information about cerebral hemodynamic status comparable with information obtained by methods in which the induction of hypercapnia requires CO2 administration (17).
Results
Conventional MR T2-weighted images showed either no (n = 3) or minimal bilateral (n = 6) signal abnormalities, which were considered compatible with the age of the patients. Image quality was satisfactory in all patients but one, whose data were excluded from further analysis. Although the passage of the bolus of gadolinium through the brain microvasculature caused an asymmetrical labeling pattern in the hemispheres in all patients, the arrival time of the bolus occurred within 15 seconds from the injection in all patients.
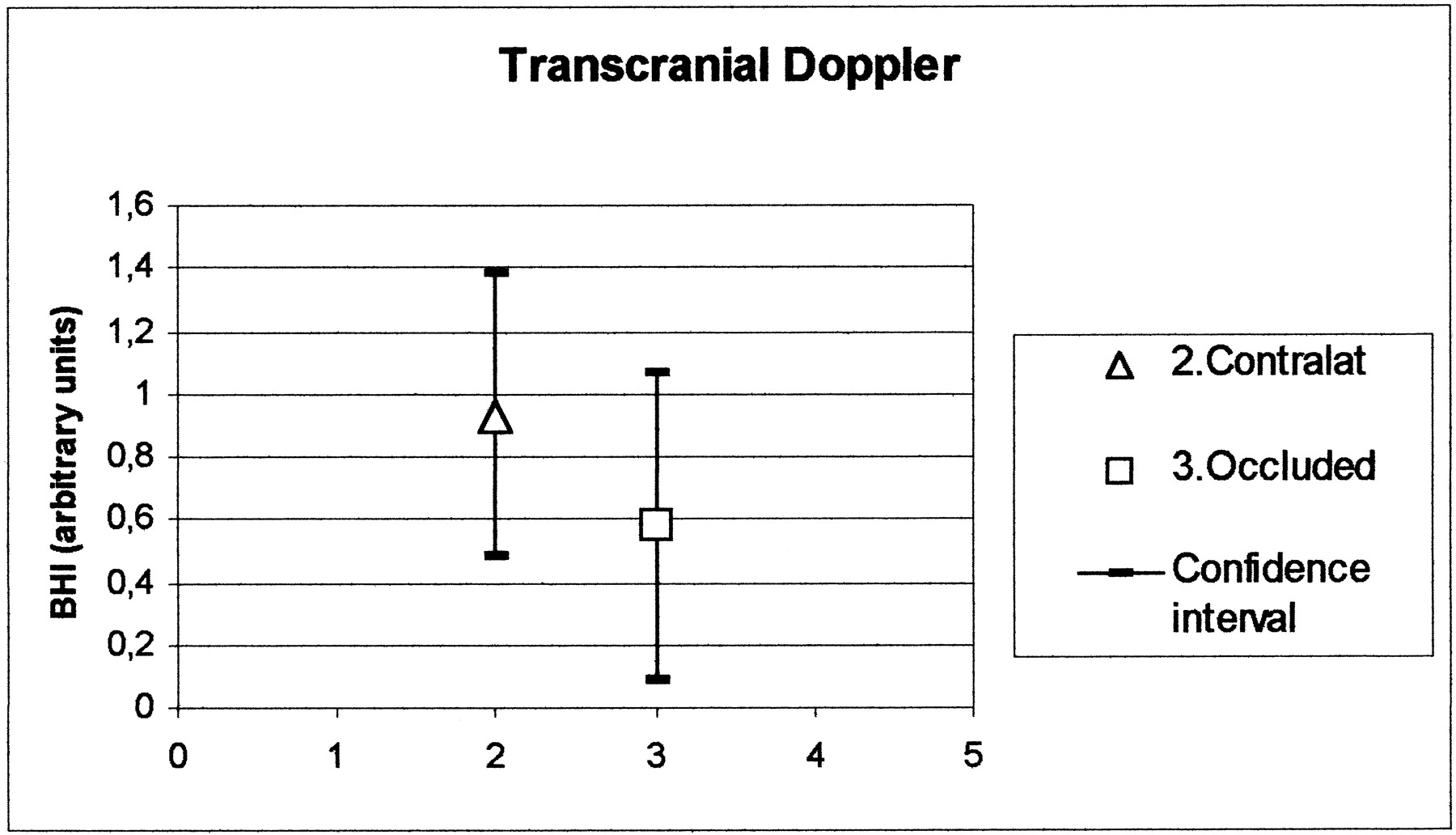
Averages and standard deviations for BHI, rCBV, rMTT, and rCBF in the group of healthy volunteers, and for the occluded and contralateral side of the patient group are summarized in the Table and Figures 1 and 2.
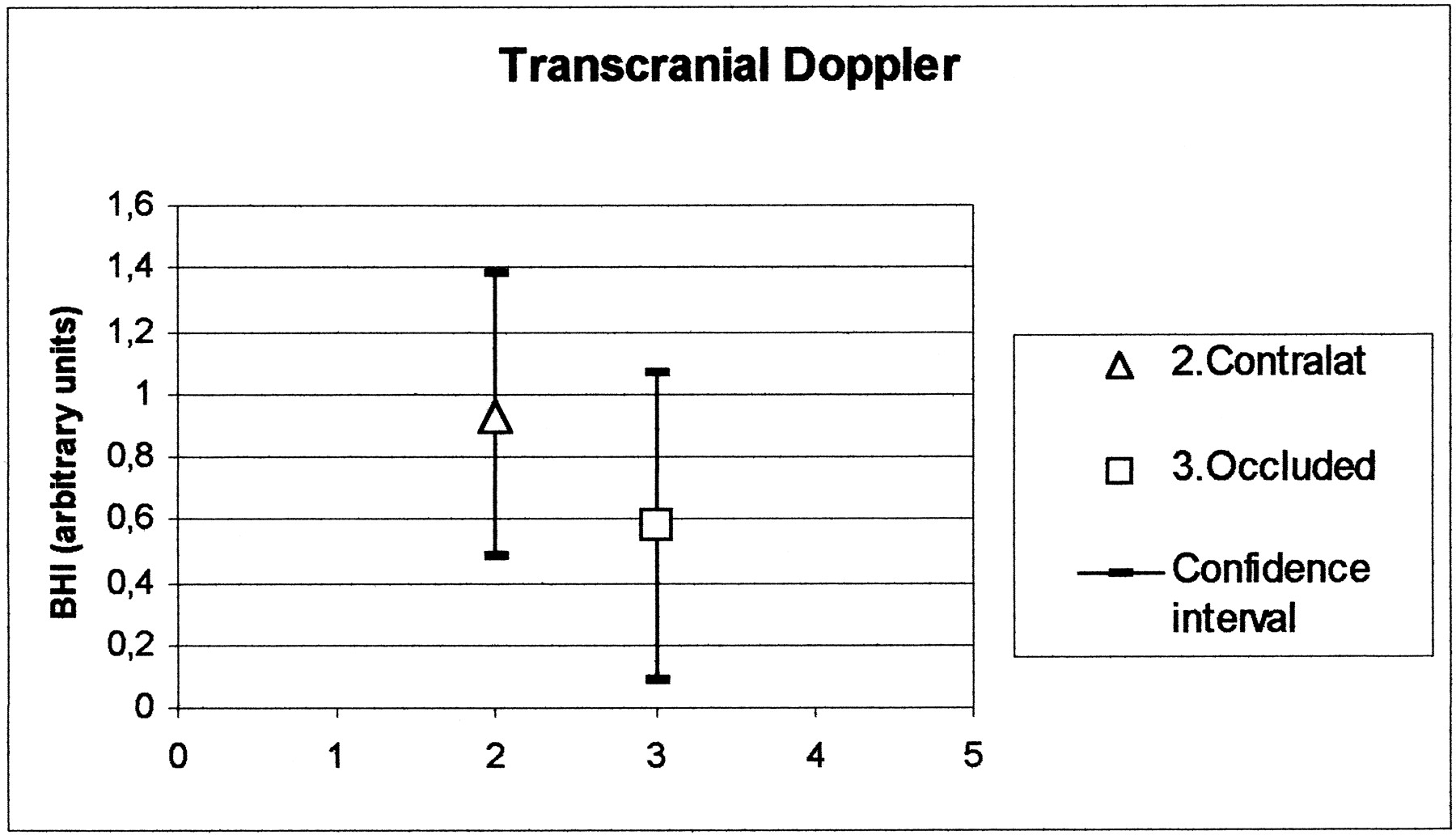
Mean values and confidence intervals (mean ± 1.96 SD) for the BHI measured by TCD
No significant difference was found between the two hemispheres of the healthy volunteers; therefore, their data are presented as the average of the two hemispheres.
A statistically significant delay of rMTT was found between the patients and the control subjects (WM: F = 8.5, P < .01; GM: F = 5.1, P < .05). The rCBV was not significantly different between the patients and volunteers (WM: F = 2.2, P = .14; GM: F = 0.8, P = .45) (occluded and contralateral sides). By contrast, within the patient group, the rCBV of the occluded side was close to significantly higher than the contralateral ICA (WM: P = .06, GM: P < .05, paired t test, corrected for multiple comparisons). The rCBF in the WM was significantly different between the occluded and the contralateral sides and the group of controls (WM: F = 11.5, P < .001). This difference was less pronounced for the GM (F = 2.8, P < .09) ipsilateral to the occluded ICA.
The BHI was significantly lower (P < .05) in the occluded than in the contralateral side.
Linear regression analysis of the BHI versus the rCBV in the GM was performed, including data from both the occluded and contralateral side (Fig 3). There was a significant relation (r2 = 0.616, P < .001) indicating increased rCBV values at decreased BHI.

Mean values and confidence intervals (mean ± 1.96 SD) for healthy subjects and occluded and contralateral hemisphere of the patients in the GM and WM for rCBV (A), MTT (B), and rCBF (C) measured by MR

Linear regression analysis of the BHI and rCBV of the GM in the occluded hemisphere, showing that patients with higher rCBV have lower BHI values
Discussion
Patients with ICA occlusion have a variable neurologic outcome (18). The presence of ICA occlusion does not predict the hemodynamic status of the distal circulation (19). If hemodynamic factors are found to be important in the pathogenesis of ischemic stroke, then hemodynamic staging will be of the outmost importance in designing therapeutic trials. Revascularization with extracranial-intracranial bypass is reported to be more effective in patients with severely impaired cerebral hemodynamics, whereas patients with normal hemodynamics would probably benefit from antithrombotic therapy (20).
The results of our study are in overall agreement with previously published results (21, 22) reporting an increased rMTT on the occluded side and an increase of rCBV (20). The rCBF was found to be homogeneously distributed, with only slight discrepancies between the two hemispheres. The rCBF was found to be more impaired in the WM ipsilateral to the ICA occlusion than the ipsilateral GM, probably because WM is a terminal territory, while GM more easily develops a pial net of collateral pathways for blood supply from bordering vascular territories.
A significant inverse correlation was found between the BHI and rCBV (Fig 3), indicating that those patients with higher rCBV had lower BHI values, and suggesting similar significance of the two indices. The slope of the linear regression of Fig 3 described this trend; the higher end of the linear regression indicated that the hemispheres with lower values of BHI were also found to have high values of rCBV. Assuming that high rCBV reflects compensatory vasodilation, it infers the reduction of the compliance of the already dilated arteriole and capillary bed. The rCBV could be, therefore, considered an index of the residual cerebrovascular reserve and it is likely related to dilation of the microvascular bed.
Higher rCBVs, as expected from previous studies, were found in GM because of the predominant representation of the microvasculature compared with WM.
Our group of patients, homogeneous from a clinical point of view, presented variable responses to TCD-BHI with a hypercapnic stress test. The BHI provides an indirect measurement of cerebrovascular reactivity in patients in which adaptation to a blood supply regimen has led to a vasodilation of intracranial vessels of various degrees. In this respect, recent investigations have shown a significant correlation between a reduction of BHI values and the risk of stroke in patients with carotid artery steno-occlusive disease (6, 23, 24). The strong inverse correlation between rCBV and BHI seems to indicate similar significance of the two indices. Major discrepancies of the rCBV and BHI between the two hemispheres could be interpreted, in our opinion, as inefficiency of collateral pathways. Hence, a more or less even distribution of blood flow between the two hemispheres possibly could be considered an indirect assessment of the functionality of the collateral circulation.
Although the mean rCBV between the two hemispheres of the patient group reached only near significance, the large confidence interval and the fact that mean rCBV was not statistically different in the patient and control groups reflects the fact that rCBV alone cannot be used predictively in individual patients with asymptomatic ICA occlusion. This concurs with a recent article (25) suggesting that rCBV did not correlate with reserve capacity assessed by SPECT before and after acetazolamide challenge in symptomatic occluded ICA. The overlap of the confidence intervals of BHI study has similar import.
The striking inverse correlation of rCBV and BHI, which may reflect physiologic events at different vascular levels, suggests that each is indeed a marker for the relative efficacy of collateral flow. The challenge is to learn how to use these tests individually or in combination to identify when inefficiency borders on—and predicts—ischemia.
Conclusion
On the basis of our preliminary observation, BHI by TCD and rCBV by MR imaging showed a significant inverse correlation, suggesting similar significance of the two indices. They provided complementary data that should be analyzed together, because they indicate two different vascular levels reflecting a marker of the efficacy of collateral flow.
The challenge is to learn how to use these tests individually or in combination to identify those patients at risk of ischemia.
Footnotes
1 Address reprint requests to Alessio Apruzzese, via Cesare Rasponi 19, 00162 Rome, Italy.
References
- Received January 28, 2000.
- Accepted after revision February 5, 2001.
Average values (standard deviaiton) of results of transcranial Doppler sonography and perfusion MR for white matter and gray matter
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- DSC MR Perfusion at 7T MRI: An Initial Single-Center Study for Validity and Practicability
- ASFNR Recommendations for Clinical Performance of MR Dynamic Susceptibility Contrast Perfusion Imaging of the Brain
- Quantitative Assessment of Cerebral Hemodynamics Using Perfusion-Weighted MRI in Patients With Major Cerebral Artery Occlusive Disease: Comparison With Positron Emission Tomography