
Abstract
Summary: three-dimensional CT maximum intensity projection (MIP) can depict suture patency, extent of synostosis (ie, complete versus incomplete bone bridging), fracture extent and conspicuity, and 3D calvarial deformity as a single set of projections in children with suspected craniosynostosis or skull fracture. Three-dimensional CT MIP may provide, in only eight views, all the required information to make the diagnosis of craniosynostosis and calvarial fracture extent currently requiring the combined information of 3D CT shaded surface displays and 2D axial CT images (a total of 58 views), and in some cases complementary skull radiographs. Three-dimensional MIP can be added to calvarial helical (spiral) CT imaging with only 5 minutes of additional postprocessing time.
Imaging plays an important role in the diagnosis of craniosynostosis and skull fractures (1). Patients with suspected craniosynostosis are usually studied with 3D CT and/or plain radiography (2). Diagnostic performance of 3D CT is better than plain radiography, but the former has limitations and pitfalls (2). Three-dimensional CT shaded surface display (SSD), which is commonly used, may blend the open suture with the adjacent calvarial bone, giving false-positive results (Fig 1A). Furthermore, 3D CT SSD may not display perisutural sclerosis well, which may be seen in early sutural closure (1). In addition, 2D axial CT images may not show suture patency well if the plane of sectioning is running parallel to the suture (Fig 1B). Because of these limitations and pitfalls, plain radiographs may be needed in some cases to complement CT's diagnostic information (Fig 1C). On the other hand, in patients with severe head trauma, CT is usually performed initially to exclude calvarial and intracranial injury (1). Conventional axial CT images, however, may miss fractures of the calvaria, especially if they are parallel to the axis of sectioning.

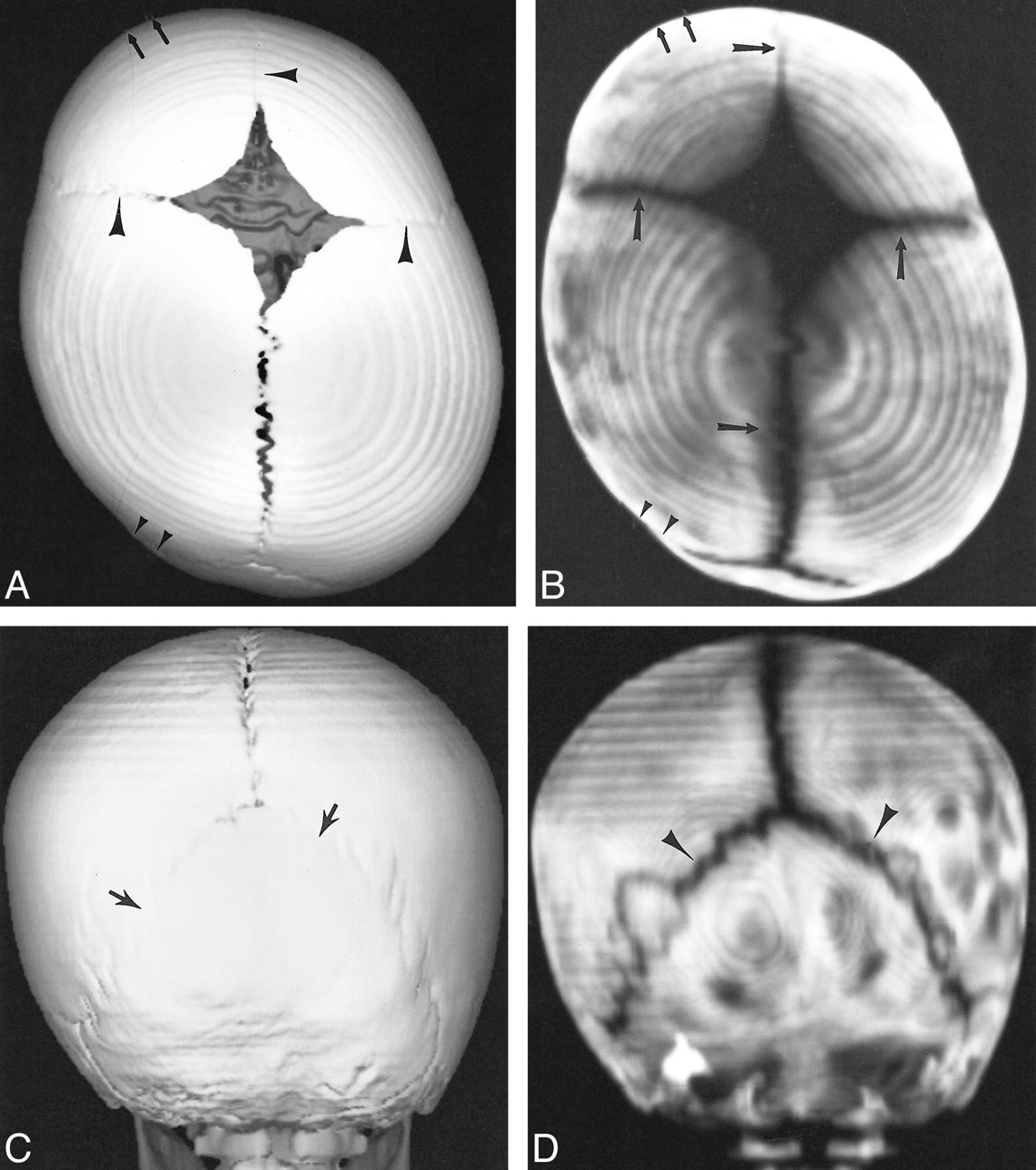
Patient with Antley-Bixler syndrome, who is at risk of lambdoid craniosynostosis.>> A, Posterior projection of 3D CT SSD appears to show closure of the lambdoid suture (arrows).>>B, 2D axial CT image is equivocal in showing left lambdoid patency (arrow).>>C, Plain radiograph obtained the same day reveals an open right lambdoid suture (arrowheads) and questionable patent left lambdoid suture (small arrows).>>D, 3D CT MIP clearly demonstrates patent lambdoid suture bilaterally (small arrowheads)
Maximum intensity projections (MIP) have become a commonly used algorithm for 3D reconstruction of CT angiograms, because they allow separation of high-attenuation enhancing vessels from the lower density surrounding soft tissues (3). This technical note describes the use of calvarial 3D CT MIP in children with suspected craniosynostosis and skull fractures.
Description of Technique
Technique
Spiral (helical) CT from the base of the skull to the vertex was done on a General Electric Hi-Speed Advantage Spiral CT (General Electric Company, Milwaukee, WI). A 3-mm collimated helical scan with a 1.3:1 pitch was obtained. Images were reconstructed with a 50% overlap at 1.5-mm intervals. Exposure parameters included a kV of 120 and mA of 80–100.
Three-dimensional MIP reconstructions were generated using the software from the General Electric Advantage Windows 3D workstation. Most state-of-the-art CT workstations currently have MIP software programs.
MIP assigns an intensity to each pixel on the screen that is the maximum of all intensities (ie, bone) in the 3D model along a perpendicular line through that pixel (3, 4). Three-dimensional MIP images are reconstructed using only half the calvaria facing the reader. This allows projection of the maximum intensity pixels without overlapping bony structures, which may obscure the patent sutures or fractures. Three-dimensional MIP reconstructions were displayed in frontal, bilateral frontal, oblique, posterior, vertex, base, and right and left lateral orientation (eight projections) for full assessment of all the sutures and calvarial bones. Average reconstruction time for MIP was 5 minutes. No additional scanning time or radiation to the patient was required, because we used the same data set applied for conventional 3D SSD reconstructions.
Patients
Ten patients with a mean age of 20 months (range, 2 months–6 years) were studied. All patients were recruited in a 9-month period and underwent at least a 4-month follow-up. Patients with less than a 4-month follow-up were excluded. Nine patients were referred to rule out craniosynostosis and one with known depressed fracture for assessment of fracture extent. All patients had spiral (helical CT) with 3D MIP (eight projections) and SSD reconstruction (eight projections) and 2D axial bone window CT images (50 views). Eight patients underwent three-view plain radiography. Final diagnosis of craniosynostosis or fracture was based on operative results or at least 4 months of clinical and/or imaging follow-up. Final diagnosis included six cases of craniosynostoses (sagittal n = 4; coronal n = 2), fracture in three, and positional molding in two. Of the three patients with fracture, one had a known depressed fracture, whereas the other two children had incidental nondepressed fractures. One of the patients with an incidental fracture also had craniosynostosis.
Discussion
Comprehensive understanding of sutural anatomy, fracture characteristics, and three-dimensional skull deformity is important for the diagnosis and potential surgical correction of craniosynostosis or skull fractures. In children with suspected craniosynostosis or calvarial fracture, 3D CT MIP can depict suture patency, extent of synostosis (ie, complete versus incomplete bony bridging), fracture extent and conspicuity, and three-dimensional calvarial deformity as a single set of eight projections (Figs 1–5).
In one patient with sagittal craniosynostosis, a 3D CT MIP reconstruction showed complete bridging of the anterior and middle sagittal suture, but incomplete closure posteriorly, with surrounding sclerosis (Fig 2). Complete and incomplete bony bridging was well characterized by the 3D MIP reconstructions (Fig 2). In patients with clinical suspicion of lambdoid craniosynostosis versus positional molding, 3D MIP adequately showed the patency of the lambdoid suture and associated calvarial deformity required to separate these two entities (Fig 3).

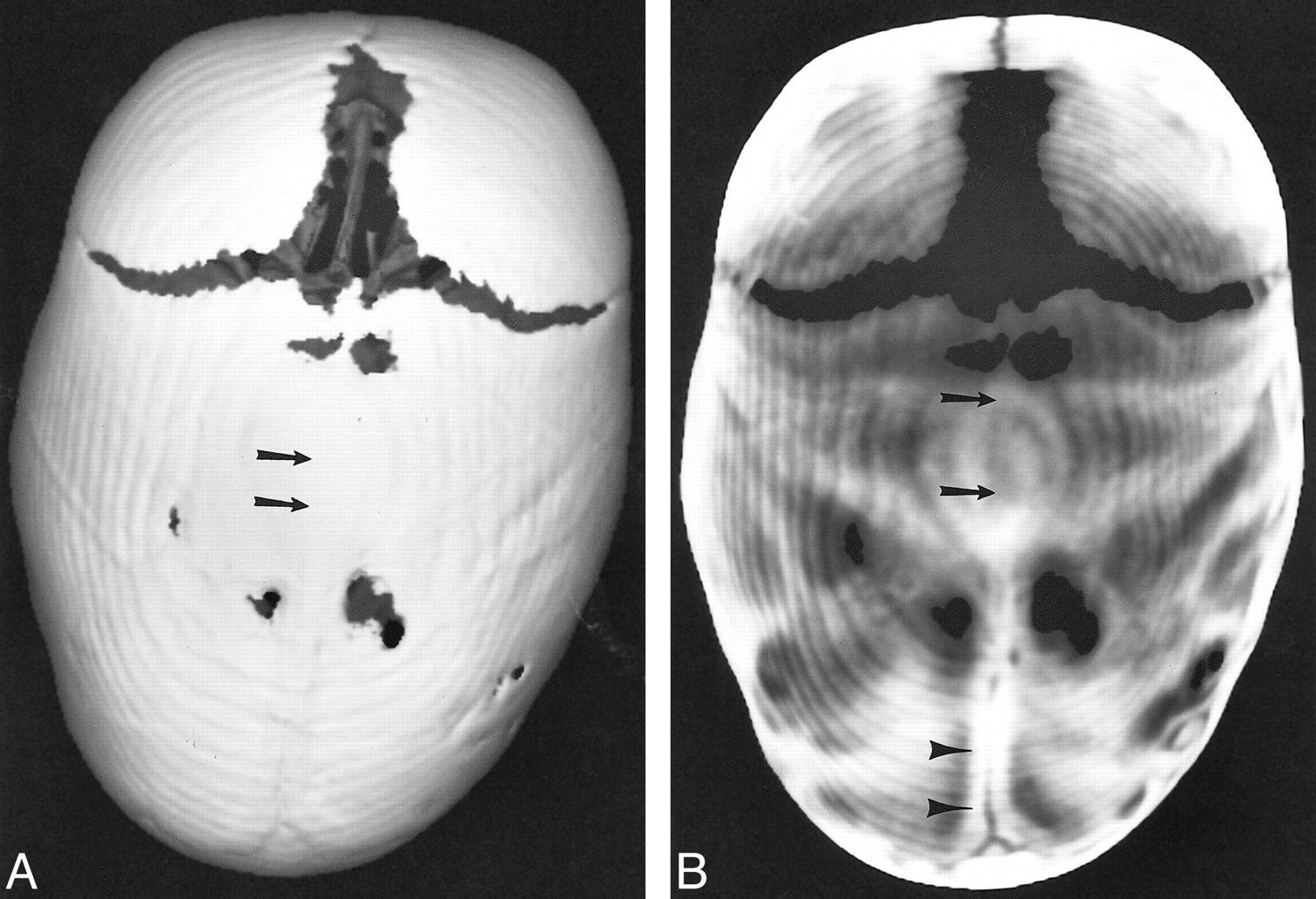
Patient with sagittal craniosynostosis.>>A, Superior view of 3D CT SSD shows complete closure of the superior sagittal suture.>>B, Comparable superior view of 3D CT MIP characterizes the sagittal suture synostosis further by showing complete closure of the anterior and mid suture (arrows), but still incomplete closure posteriorly, with surrounding sclerosis (arrowheads)
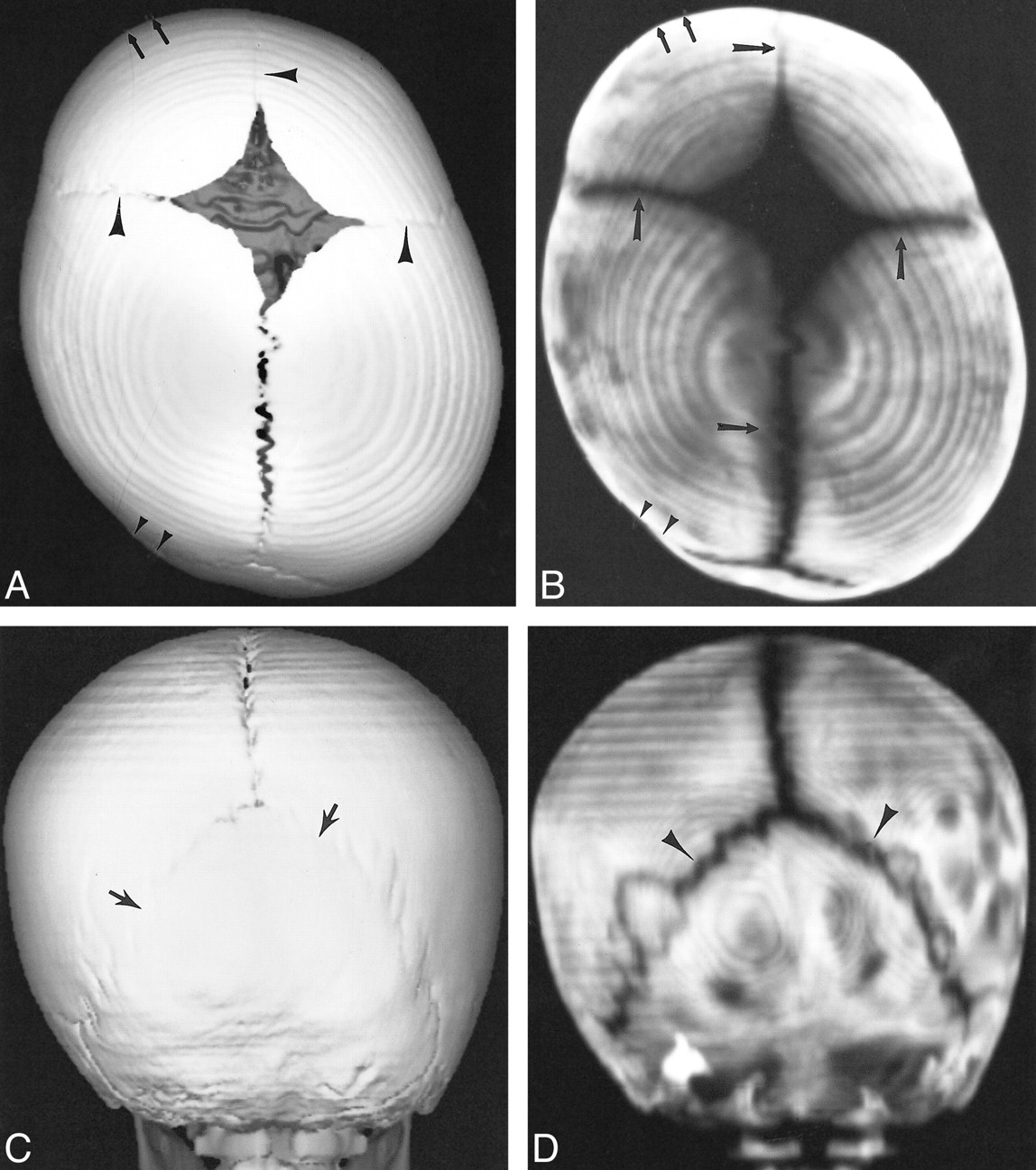
Patient with positional molding.>>A, Superior projection of 3D CT SSD shows patent sagittal suture and probable patency of coronal and metopic sutures (arrowheads).>>B, Same projection with 3D CT MIP shows clearly patency of the coronal, sagittal, and metopic sutures (arrows). Both reconstructions show characteristic flattening of the posterior calvaria (small arrows) and ipsilateral frontal bone bossing (small arrowheads).>>C, Posterior projection of 3D CT SSD shows questionable patency of the entire lambdoid suture (arrows).>>D, Same projection with 3D CT MIP reveals unequivocal patency of lambdoid suture bilaterally (arrowheads)
Three-dimensional MIP demonstrated the calvarial deformity in all dimensions (ie, depressed fracture) as well as the fracture extent in a single set of projections (Figs 4 and 5). Three-dimensional MIP also showed the full extent of complex skull fractures extending in multiple bones and planes.

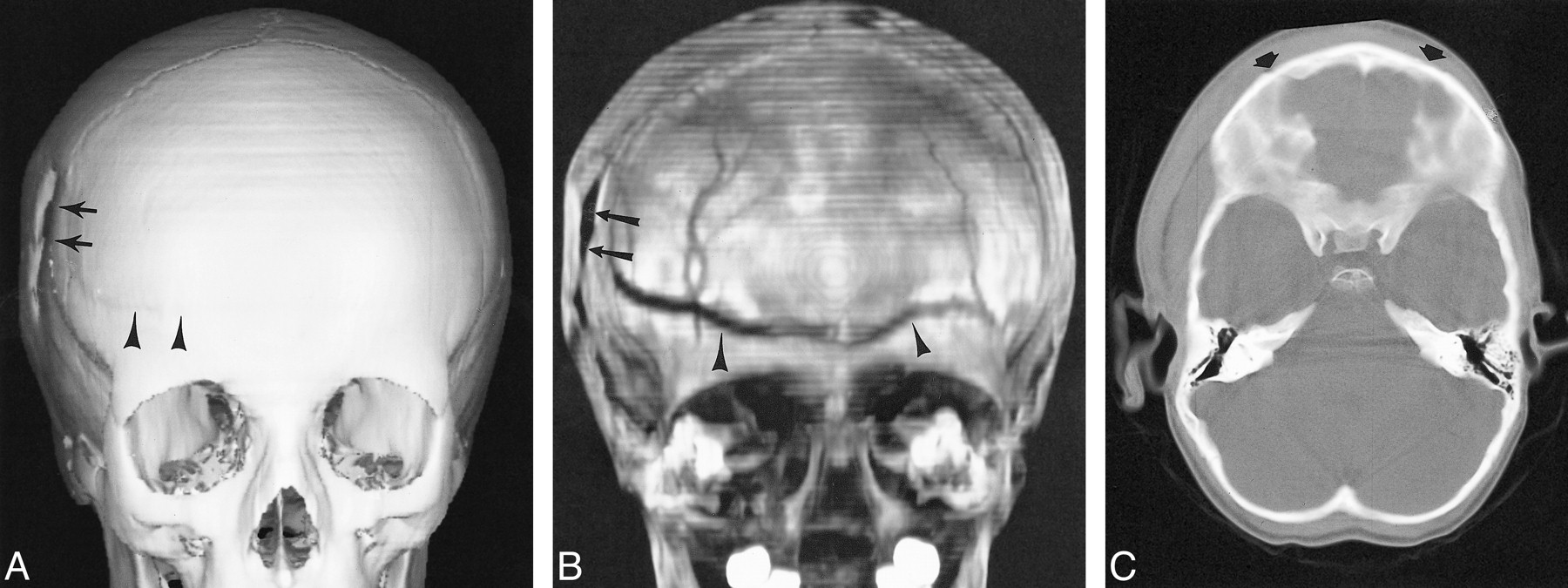
Patient with depressed right parietal fracture extending into the frontal bone.>>A, Frontal projection of 3D CT SSD reveals the depressed parietal fracture (arrows) but poorly outlines the extent of the frontal fracture (arrowheads).>>B, Comparable 3D CT MIP projection not only reveals the depressed parietal fracture (arrows) but the full extent of the frontal fracture (arrowheads).>>C, 2D axial CT failed to show the nondepressed frontal fracture component running parallel to sectioning plane (arrows)

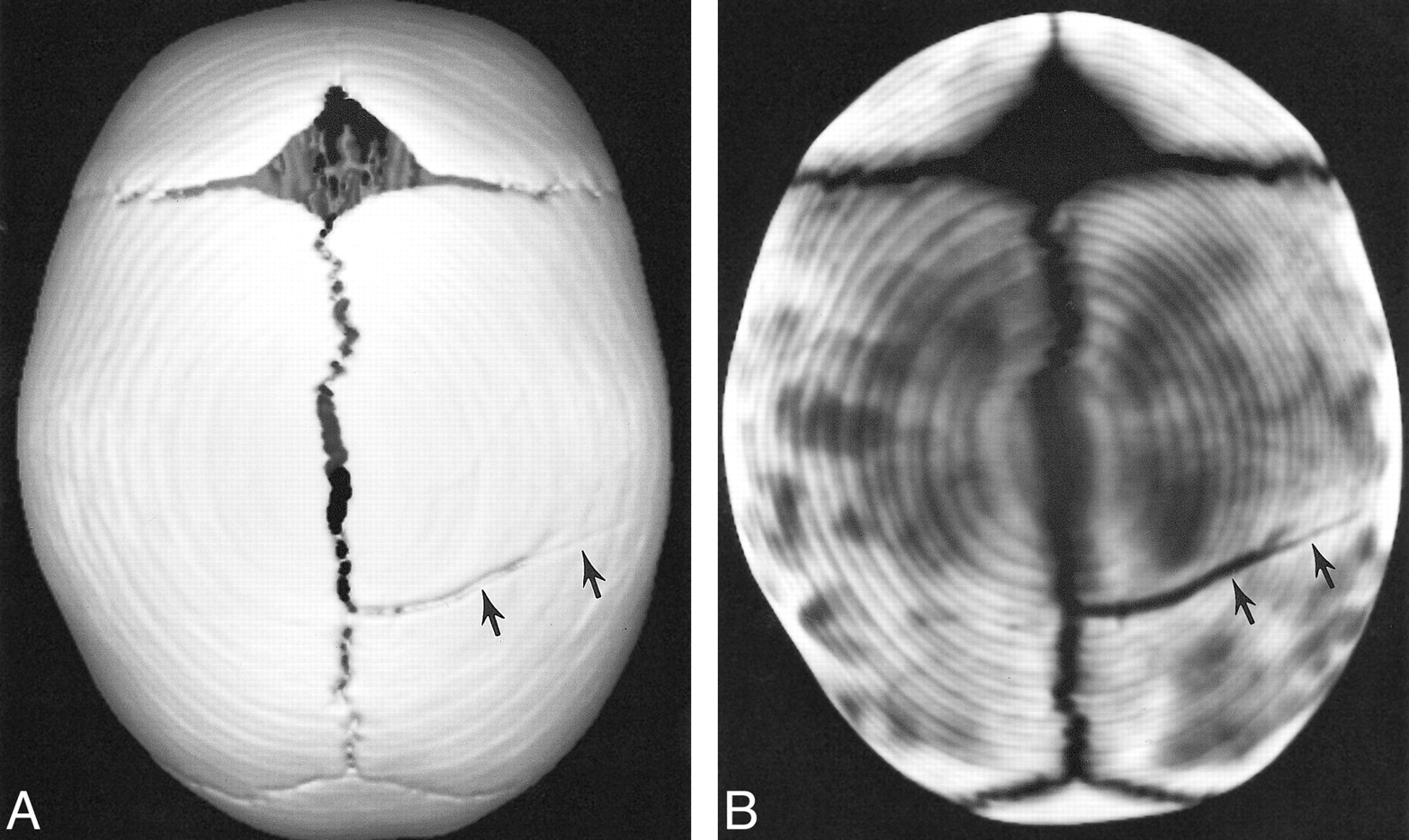
Patient with non-depressed parietal fracture.>>A, Superior projection of 3D CT SSD blends the margins of the fracture with the calvaria, making assessment of the extent of the fracture less conspicuous.>>B, Comparable 3D CT MIP shows the full extent of the fracture by separating the high density bone from the low-density fracture. Also note that conspicuity of all open sutures is well shown with 3D CT MIP
Suture patency, extent of craniosynostosis, and fracture conspicuity is shown well by MIP, because it assigns the maximum of all intensities in the 3D model along a perpendicular line through that pixel (3, 4). This perpendicular assignment decreases the potential of blending the open suture or fracture with the adjacent calvarial bone, a common pitfall with conventional 3D CT SSD recontructions (Figs 1–5). In addition, 3D CT MIP 50% image reformat overlap decreases the potential of missing a fracture or patent suture (ie, squamosal suture) running parallel to the CT plane of sectioning.
MIP software is currently available in most state-of-the-art spiral (helical) CT workstations. Three-dimensional MIP only requires 5 minutes of postprocessing time and can be added to any spiral (helical) CT calvarial acquisition. Currently used 3D CT SSD and 2D axial CT images require the rexamination of at least eight and 50 views, respectively, for a total of 56 images, whereas the entire calvarium can be assessed using eight MIP projections.
Vannier and colleagues (5) have described other 3D reconstruction algorithms, including surface-projection rendering (SPR) for craniosynostosis. This technique creates the image by calculating cumulative density along a ray perpendicular to the displayed surface. This technique makes brightness inversely proportional to cumulative density (5). SPR uses surface projection, which calculates cumulative density only for those features with a chosen distance below the object surface (5). Although this postprocessing technique depicts craniosynostosis well, it is not as widely available as MIP.
This technical note illustrates our initial experience with 3D CT MIP. A larger prospective study is required to compare the different 3D CT reconstructions (ie, MIP vs SSD), 2D axial CT images, and plain radiographs before MIP can be recommended for routine clinical practice. We are currently conducting such a prospective study to determine sensitivity, specificity, and interobserver and intraobserver agreement of 3D CT MIP in the setting of various skull defects.
In summary, 3D CT MIP can depict suture patency, extent of synostosis (ie, complete versus incomplete bone bridging), fracture extent and conspicuity, and three-dimensional calvarial deformity as a single set of projections in children with suspected craniosynostosis or skull fracture. Three-dimensional CT MIP may provide, in only eight views, all the required information to make the diagnosis of craniosynostosis and calvarial fracture extent in contrast to the combined information of 3D CT SSD and 2D axial CT images (total of 58 views) and complementary skull radiographs. Three-dimensional MIP can be added to calvarial helical (spiral) CT imaging, adding only 5 minutes of postprocessing time.
Acknowledgments
I am indebted to Gary L. Hedlund and Mark J. Halsted for their valuable comments at the beginning and end of this project, respectively.
- Received January 25, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.