
Abstract
Summary: Kimura disease is a rare chronic inflammatory disorder mimicking malignancy. Nodes are present in the submental and submandibular regions, within the parotid gland, and in the upper cervical chain. On gray scale sonograms, they are hypoechoic and round, with normal hilar architecture and homogeneous internal echoes. On power Doppler sonograms, the nodes show prominent intranodal vessels with a hilar pattern and low intranodal resistance. The soft tissue and parotid lesions also show low-resistance vascularity within.
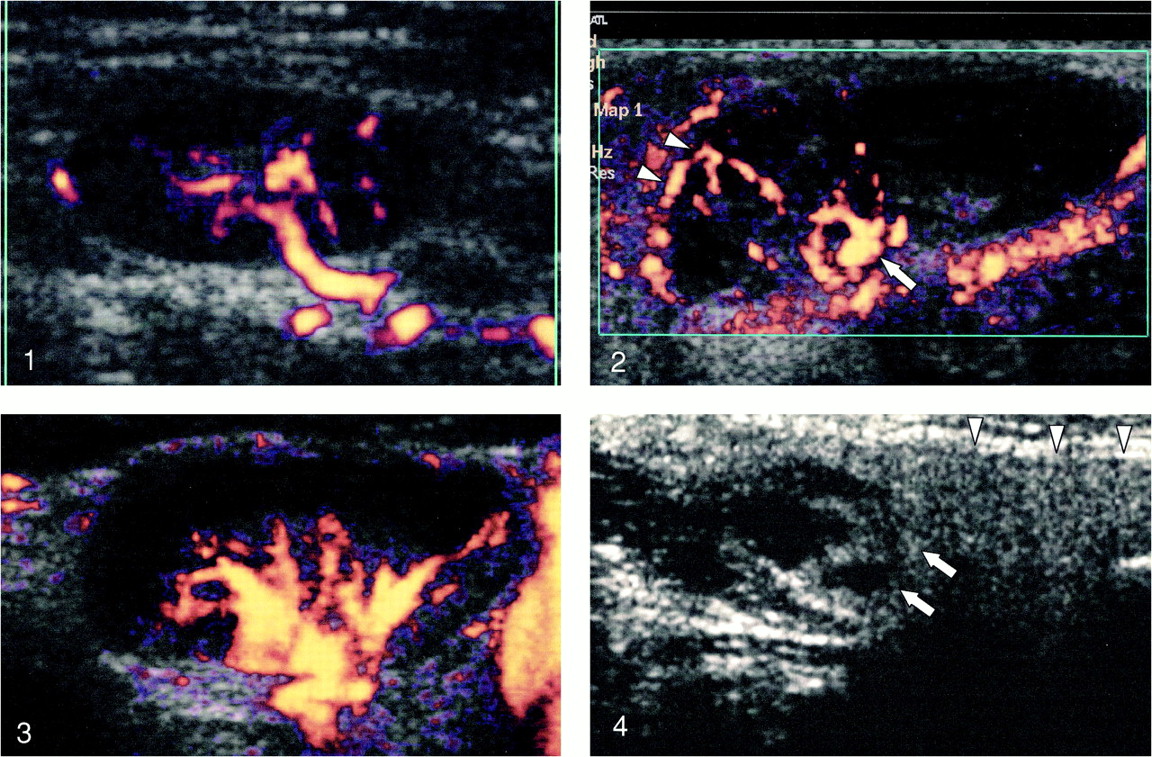
Kimura disease is a chronic inflammatory disorder of unknown origin that mimics a malignant lesion both clinically and on images (1). It is, however, a benign condition, and the prognosis is good, even with conservative treatment. Although there are reports of the appearances of Kimura disease on CT scans (2) and MR images (3), there is scant information in the literature regarding gray scale (1) and power Doppler sonography of Kimura disease. This report documents the appearances of Kimura disease on gray scale and power Doppler sonograms. On power Doppler sonograms, normal nodes show hilar vascularity (Fig 1) and malignant nodes have a more variable appearance.
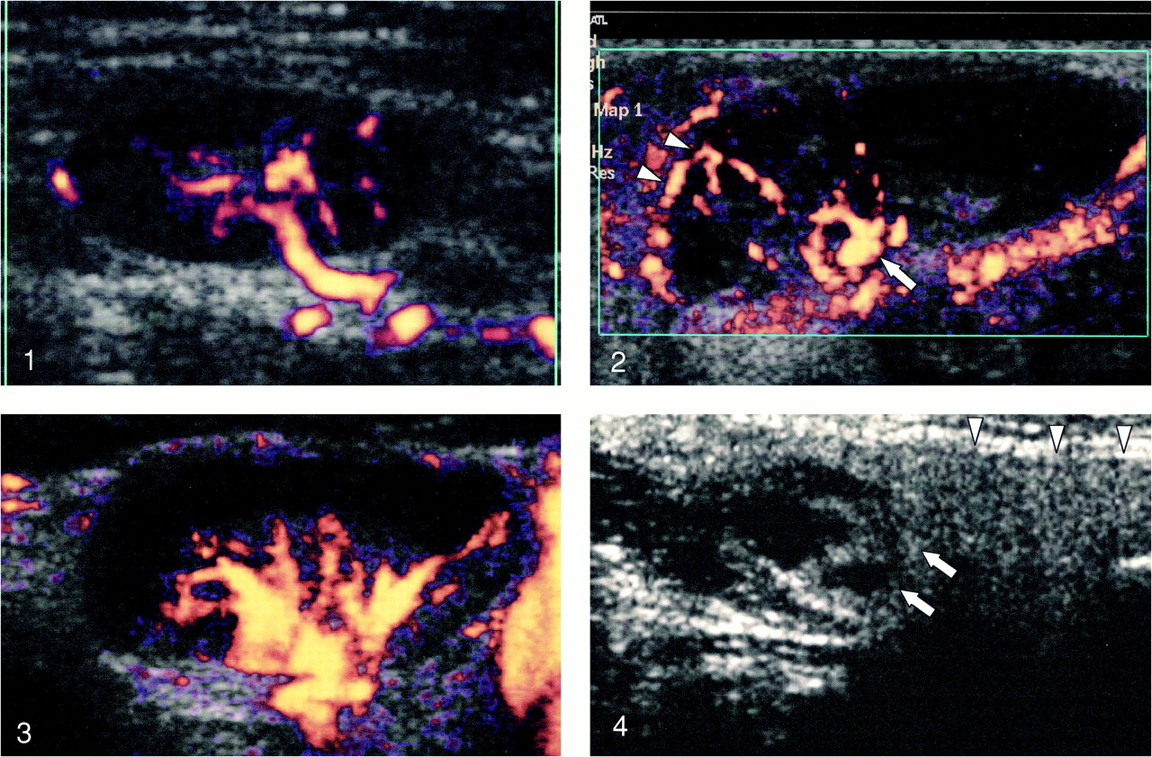
Power Doppler sonogram of a normal lymph node shows hilar vascularity.fig 2. Power Doppler sonogram of a lymph node with Kimura disease shows hilar (arrow) and capsular (arrowheads) vascularity.fig 3. Power Doppler sonogram of a lymph node with Kimura disease shows exaggerated hilar vascularity.fig 4. Transverse gray scale sonogram shows an ill-defined, hypoechoic, heterogeneous nodule with cystic areas within (arrows) in the superficial lobe of the parotid gland (arrowheads).
Case Reports
Case 1
A 33-year-old Vietnamese man with chronic renal failure receiving peritoneal dialysis presented with a 4- to 5-year history of a right submandibular mass. A physical examination revealed that the mass was 4 cm in diameter, firm, lobulated, non-tender, and mobile. No other masses in the neck could be palpated, and the buccal cavity was clear. There was no associated blood eosinophilia, and the serum immunoglobulin E level was not obtained.
A high-resolution sonographic examination (5–12 MHz, ATL HDI 5000 ultrasound system; Bothell, WA) showed unilateral, multiple, round, hypoechoic nodes with sharp borders in the submental and submandibular regions and along the upper cervical chains on the right. All the nodes showed homogeneous internal echoes with preserved hilar architecture (three of four nodes), and on power Doppler sonograms, all the nodes showed profuse, low-resistance vascularity (resistive index [RI] < 0.8 and pulsatility index [PI] < 1.6). Three of the four nodes showed hilar vascularity, and mixed (hilar and capsular) vascularity was seen in one (Fig 2). A fine-needle aspiration biopsy of the node suggested Kimura disease, which was confirmed by an excision biopsy of the right submandibular node.
Case 2
A 62-year-old Chinese man presented with a 10-year history of a right postauricular mass. A physical examination revealed that the mass was 15 mm, non-tender, firm, and lobulated. Small adjacent nodes were palpated in the neck. The results of an examination of the oral cavity were unremarkable. There was no eosinophilia detected in the blood, and the immunoglobulin E level was not obtained.
A high-resolution sonographic examination (5–12 MHz, ATL HDI 5000) showed unilateral multiple round hypoechoic nodes with sharp borders in the right parotid gland. Both the nodes showed homogeneous internal echoes with preserved hilar architecture, and on power Doppler sonograms, both the nodes showed profuse, low resistance (RI < 0.8, PI < 1.6) hilar vascularity (Fig 3).
In addition, in the right parotid gland, there was a 15-mm, noncalcified, ill-defined, hypoechoic mass, with areas of necrosis within (Fig 4). Its internal architecture was not suggestive of a lymph node. On power Doppler sonograms, it showed low-resistance (RI < 0.8, PI <1.6) arterial vessels within.
In view of a parotid nodule and multiple enlarged associated nodes, a suspicion of a malignant parotid lesion was raised. A sonographically guided fine-needle aspiration biopsy of the parotid mass and the lymph node suggested a lymphoproliferative lesion. The diagnosis of Kimura disease was made after excision of the mass and the node.
Case 3
A 42-year-old Chinese man presented with a 5-year history of enlarging masses in his auricles, accompanied by itchiness. A physical examination revealed that the auricular masses were firm, non-tender, and lobulated, with multiple scabs on the skin surface. In addition, there were multiple mobile non-tender lymph nodes in both the submandibular areas and upper cervical chains. A WBC differential count revealed an eosinophil count of 29.9% (normal range, <4.5%). The serum immunoglobulin E level was not obtained.
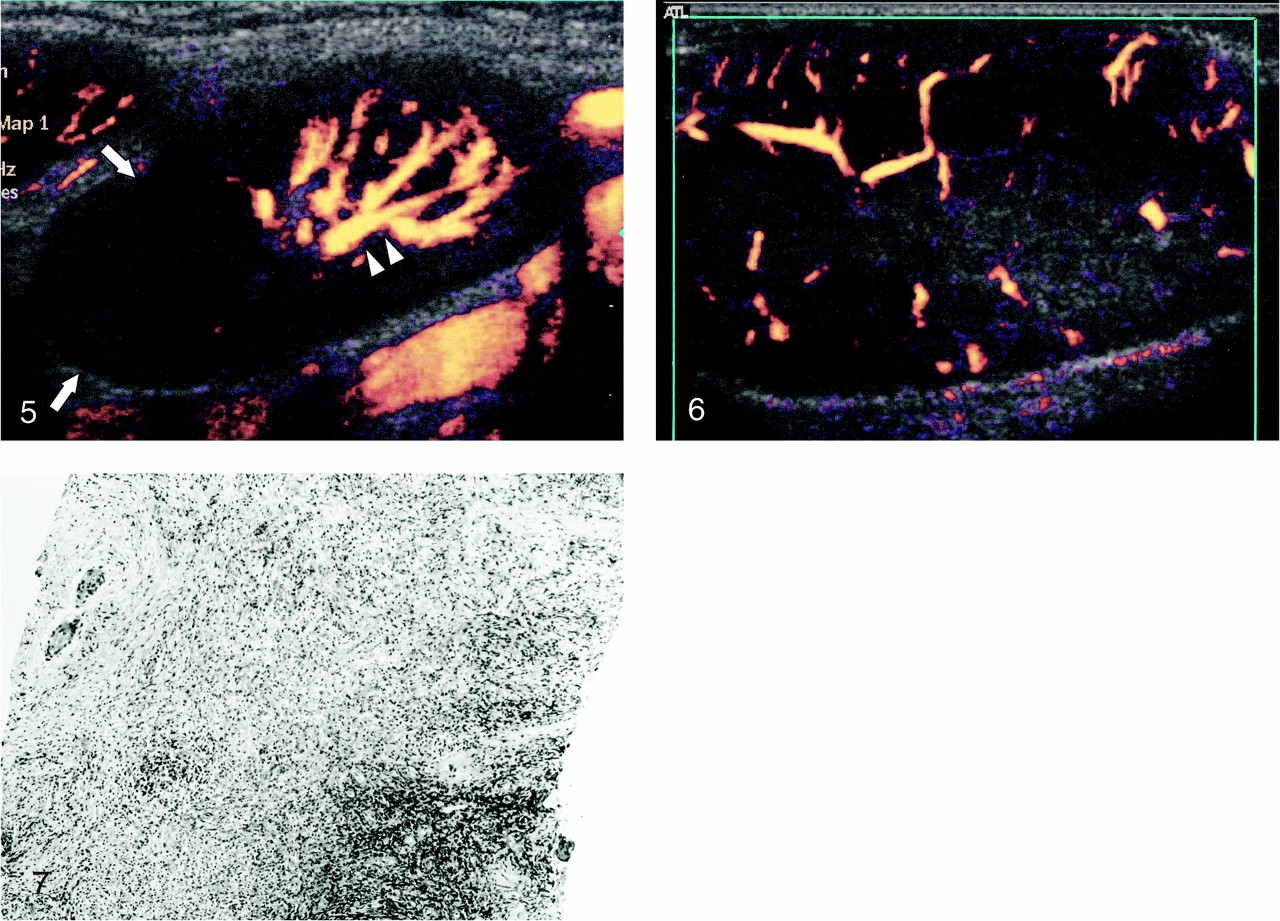
A high-resolution sonographic examination (5–12 MHz, ATL HDI 5000) showed bilateral, multiple, round, hypoechoic nodes with sharp borders in the submandibular region, within the parotid glands, and along the upper cervical chains. Seven of the nine nodes showed homogeneous internal echoes with preserved hila, but two had intranodal necrosis. On power Doppler sonograms, all the nodes showed profuse, low-resistance vascularity (RI < 0.8, PI < 1.6). In all nine nodes, hilar vascularity was observed; one also exhibited capsular vascularity. Of the eight patients with hilar vascularity, the presence of intranodal necrosis displaced the vessels in two nodes (Fig 5). Both the pinna and the ear lobe were massively enlarged and, on sonograms, showed homogeneous, hypoechoic internal echoes. There were multiple arteries and veins (Fig 6) within the lesion, and the arteries showed a low-resistance (RI < 0.8, PI < 1.6) pattern similar to that of the associated node. A fine-needle aspiration biopsy of the node suggested a chronic granulomatous condition. However, a diagnosis of Kimura disease was made after biopsy of the node and the right ear lobe (Fig 7).

Power Doppler sonogram of a lymph node with Kimura disease shows predominant hilar vascularity (arrowheads). Note the displacement of the hilar vessels by avascular cystic areas within the node (arrows).fig 6. Power Doppler sonogram of an enlarged ear lobe shows hypoechoic internal echoes and multiple vessels scattered within.fig 7. Biopsy of a soft-tissue lesion shows chronic inflammatory infiltrates with fibrotic stroma. The infiltrates consist of small and activated lymphoid cells and many infiltrates
In all three cases, all other nodes with gray scale and power Doppler appearances similar to those of the biopsied node were also considered to be Kimura disease. The sonographic appearances of the nodes are shown in Tables 1 and 2.
Gray-scale sonographic features of lymph nodes in the three cases of Kimura disease
Doppler sonographic characteristics of lymph nodes in the three cases of Kimura disease
Discussion
It is generally accepted that Kimura disease was first described in 1937 in China by Kim and Szeto (4). The disease was initially called eosinophilic hyperplastic lymphogranuloma. This disease became more widely known as Kimura disease after Kimura et al (5) reported similar cases occurring in Japan and described the condition as “unusual granulation combined with hyperplastic changes in lymphoid tissue.”
Histologically, lesions in Kimura disease are characterized by numerous lymphoid follicles with proliferation of post-capillary venules lined by plump endothelium and marked eosinophilic infiltrates (6). Nodal involvement by Kimura disease is characterized by prominent eosinophilic infiltration with occasional formation of eosinophilic microabscesses, increased number of small blood vessels, eosinophilic folliculolysis, and perinidal eosinophilic infiltration. Specific cytologic features of Kimura disease have been described and, on cytology smears, include presence of significant numbers of eosinophils in a background of lymphoid cells and fragments of collagenous tissue and Warthin-Finkeldey polykaryocytes. In the cell block, vascular proliferation and fibrosis are useful features that support the diagnosis (7).
The disease occurs mainly in people of Asian descent, and more than 80% of the patients are men in their second and third decades. The most common presenting feature is swelling in the salivary region and adjacent lymphadenopathy.
The previously described appearances of Kimura disease on CT scans and MR images vary. On CT scans, irregularly shaped subcutaneous mass or masses and swelling of the salivary glands are seen (8). On contrast-enhanced CT scans, enlarged lymph nodes show homogeneous enhancement, whereas the salivary glands enhance heterogeneously (2). On T1-weighted MR images, the masses are either hypointense or isointense compared with salivary tissue and hyperintense on T2-weighted images (1). However, the hyperintensity on T2-weighted images and the degree of enhancement on CT scans vary, probably because of different degrees of fibrosis and vascular proliferation (9). Increased uptake on early and delayed Tl-201 single-photon emission CT scans have also been reported in the soft-tissue masses in cases of Kimura disease (10).
Sonographic evaluation of Kimura disease consists of two parts: gray scale findings and power Doppler findings.
Gray Scale Sonography
The sonographic findings of adenopathy in association with Kimura disease have been previously reported. The nodes were hypoechoic, solid, and distributed in the submental and submandibular regions and in the upper cervical chains (1). Some maintain their hilar architecture.
In this study, all the nodes with Kimura disease were round, well defined, and hypoechoic, and showed the presence of an echogenic hilum. Most nodes were homogeneous (87%), and only two nodes (13%) showed evidence of intranodal necrosis. All the nodes were distributed in the submental and submandibular regions and upper cervical chains, and in all the cases, the adjacent soft tissues were normal. With the newer high-resolution transducers, the appearances are consistent with the gray scale features described in the earlier report (1).
Power Doppler Sonography
There are numerous reports of the role of power Doppler sonography in differentiating benign from malignant nodes (11, 12). Although few nodes with Kimura disease are included in these studies (1, 11, 12), the appearances of these nodes have not been specifically described. We were therefore interested to learn whether nodes with Kimura disease had any specific appearances on power Doppler sonography that may help in their identification.
Intranodal Vascular Distribution
In reactive nodal disease, nodes tend to have prominent hilar vascularity (11) owing to increase in vessel diameter and blood flow (12). Malignant nodes have a more variable vascular pattern and may show avascular areas, displacement of vessels, increased peripheral vessels, and an aberrant course of hilar vessels.
Power Doppler sonography is able to detect this abnormal vascularity, evaluate the distribution of vessels, and estimate the intranodal vascular resistance, thus differentiating histologically proven benign from malignant nodes with a high degree of accuracy (83% to 89% of sensitivity and 76% to 98% of specificity) (12).
In this study, a majority (87%) of nodes in Kimura disease showed hilar vascularity and 13% showed a mixed hilar and capsular vascular pattern. Thus, in most cases, the distribution of intranodal vascularity was consistent with benign nodes, but the vessels were prominently seen.
Intranodal Vascular Resistance
Previous reports (11, 12) have suggested that benign nodes can be differentiated from malignant nodes by estimating the intranodal resistance. Malignant nodes tend to have higher intranodal vascular resistance (RI > 0.8 and PI > 1.6) compared with benign lymphadenopathy (11). In this study, all the nodes showed intranodal resistance of benign nodes with an RI and a PI of < 0.8 and < 1.6, respectively.
Involvement of Soft Tissues and Salivary Glands
Soft-tissue nodules in the neck, particularly in the region of the salivary glands, are common in cases of Kimura disease. On gray scale sonograms of a patient with Kimura disease, the appearances are also varied and the masses are hypoechoic and predominantly solid but may have a cystic component, with homogeneous or heterogenous internal architecture (1).
However, the involvement of the pinna is rare, and there has been one reported case of bilateral auricular involvement (3). One of our patients (Case 3) also had bilateral auricular involvement. On gray scale sonograms, the soft-tissue auricular mass was diffusely hypoechoic and solid, with homogeneous internal echoes. There was vascularity throughout the lesion, and power Doppler sonography showed both arterial and venous flow. On spectral Doppler sonograms, the intravascular resistance was low, with an RI and a PI < 0.8 and < 1.6, respectively. This was similar to the low intranodal vascular resistance detected in the adjacent associated nodes.
In case 3, in addition to the multiple nodes, there was also a 15-mm, well-defined, hypoechoic, heterogeneous soft-tissue mass with a cystic component in the right parotid gland. It also showed the presence of intranodular vessels that were arterial in nature, with low intravascular resistance (RI < 0.8 and PI < 1.6) similar to the low resistance in the adjacent nodes, suggestive of a benign lesion.
The differential diagnoses of Kimura disease include salivary nodules with adjacent adenopathy, and lymphadenopathy with no other lesions.
In patients with salivary nodules and adjacent adenopathy, it is not possible to exclude malignant lesions on the basis of imaging alone. However, a patient with a malignant lesion typically has a shorter history of an enlarging mass and, in the case of parotid neoplasms, may have facial nerve paralysis. On sonograms, malignant salivary lesions are ill defined, with irregular outlines and heterogeneous internal echoes. On gray scale sonograms, malignant nodes are round and hypoechoic, with heterogeneous internal architecture, and they frequently show loss of hilar architecture. On power Doppler sonograms, malignant nodes frequently show the presence of capsular vascularity, whereas Kimura disease often shows hilar vascularity only.
For patients with lymphadenopathy alone, the differential diagnoses include benign reactive nodes, Kikuchi disease (histiocytic necrotizing lymphadenitis), metastatic nodes from a regional primary lymphoma, and tuberculous adenitis. Benign reactive nodes have appearances similar to those of Kimura disease, exhibiting normal internal vascular architecture with low-resistance vascularity. However, they are more widely distributed in the neck, bilaterally, particularly along the cervical chains and posterior triangle, and they maintain an elliptical shape.
Kikuchi disease is a benign disease that is common in Japan, affecting younger women. Sonographically, the nodes are hypoechoic, homogeneous, or heterogeneous, but are surrounded by hyperechoic rims (13). They also show a benign vascular pattern on power Doppler sonograms (12). Metastatic nodes are round and hypoechoic, with loss of hilar architecture, and may show the presence of intranodal cystic or coagulation necrosis and high resistance peripheral vascularity on Doppler sonograms. Lymphomatous nodes are also round and hypoechoic and may have a micronodular or a pseudocystic appearance and show profuse central and peripheral vascularity on Doppler sonograms. In our experience, tuberculous nodes are frequently in the posterior triangle and show intranodal necrosis with nodal matting as well as adjacent soft-tissue edema. On power Doppler sonograms, they have variable appearances with mixed vascularity or displaced vascularity due to intranodal necrosis.
Therapeutic options for Kimura disease include steroids, radiotherapy, and surgery. Steroids provide transient relief, and the swelling may recur after cessation of therapy (2). However, some recommend surgery as the treatment of choice. Although complete resection is necessary, radical neck dissection for these cases is usually not performed, because functional neck dissection results in complete clearance of nodes with good cosmetic results.
Conclusion
The possibility of Kimura disease should be considered when an Asian man clinically presents with painless long-standing nodes in the salivary region that are round, solid, hypoechoic, and homogeneous, with normal hilar architecture in the submental, submandibular, and upper cervical regions on gray scale sonograms. These nodes show profuse hilar vascularity with low resistance on power Doppler sonograms and the associated soft-tissue subcutaneous and/or salivary gland lesions that also manifest low intravascular resistance. However, malignant salivary lesions with associated lymphadenopathy cannot be distinguished from Kimura disease by sonography. Other causes of enlarged lymphadenopathy, such as reactive nodes, malignant nodes, and Kikuchi disease, should also be considered in the differential diagnoses.
Footnotes
1 Address reprint requests to Anil Ahuja, FRCR, Department of Diagnostic Radiology and Organ Imaging, Prince of Wales Hospital, The Chinese University of Hong Kong, 14 Shatin, N.T., Hong Kong.
References
- Received May 1, 2000.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}