
Abstract
Summary: We report our experience with a 3.2F cerebral diagnostic catheter system. Thirty patients (aged 6 months to 76 years) had undergone cerebral angiography. All targeted brachiocephalic vessels were catheterized except for one artery (98.9% success rate). The image quality obtained with the 3.2F catheter was judged to be comparable with that using the 4F catheter in all cases. This catheter system could be used for cerebral angiography as the standard for patients of all ages.
With the advent of digital subtraction imaging technology, diagnostic cerebral angiography has become less invasive because of the reduction of the examination time and total amount of the contrast material required. However, MR angiography and/or X-ray CT angiography have emerged as first-line diagnostic angiography methods instead of catheter angiography because they are inherently less invasive. Therefore, the indication for catheter angiography has been strictly limited, and safer and less invasive catheter angiography is required in the current MR and CT angiography era.
In our hospital, the 5F diagnostic catheter was the standard for the first 2 years of the previous 6-year period, while the 4F catheter became standard for the subsequent 4 years except in pediatric patients younger than the age of 3 years. For further downsizing of diagnostic catheters, we have evaluated the feasibility of a 3.2F cerebral diagnostic catheter system for patients of all ages.
Description of the Catheter System
The 3.2F catheter (Selecon PA; Clinical Supply Co Ltd, Gifu, Japan) was made of polyamide-elastomer. The distal portion (about 2 cm) was formed from two layers and the proximal shaft from three layers, with the middle layer composed of stainless mesh. The outer diameter was 3.2F, and the inner diameter was 0.68 mm (0.027 in). The catheter accepted a 0.025-in guidewire. The surface had a hydrophilic-hydrophobic coating (fluorine-acryl-styrene-urethane-silicone copolymer). The length of the catheter was 100 cm. The maximum injection pressure allowed was less than 1100 psi, and bursting pressure was greater than 1200 psi. There were three catheter tip configurations: H1, H5, and Berenstein types. The H1 configuration catheter was the standard in our hospital. When an H1 catheter could not be introduced into the targeted brachiocephalic vessels because of tortuosity, an H5 catheter was used. The Berenstein catheter usually was used for the pediatric patients. The 0.025-in guidewire was either an Interslue (Clinical Supply Co Ltd, Gifu, Japan) or a RadiFocus (Termo Corp., Tokyo, Japan), 150 cm in length. The former guidewire, slightly stiffer than the latter, was used when more stable guidewire support was necessary. Except for the case of one patient, a 6-month-old boy, a vascular sheath with an outer diameter of 4.7F (Clinical Supply Co Ltd, Gifu, Japan) was inserted into the femoral artery.
Clinical Results
Thirty consecutive patients (15 male, 15 female patients) without selection by age had undergone diagnostic cerebral angiography, and the feasibility of the 3.2F catheter and image quality of the angiograms were evaluated. These patients ranged in age from 6 months to 76 years (mean, 49.3 years). Of the 30 patients, four were in their first decade; one, his second decade; three, their fourth decade; five, their fifth decade; six, their sixth decade; four, their seventh decade; and seven, their eighth decade. Aortography was performed with the same type of catheter in 10 patients. Indications for angiography were suspected cerebrovascular diseases in 20 patients, brain tumors in seven patients, and head trauma in three patients. The contrast material used in this series was iopamidol with an iodine concentration of 300 mg/mL. Angiography was performed after the patients were administered local anesthesia, except for the pediatric patients and the severely ill, who required general anesthesia. The transfemoral approach using the Seldinger method was chosen in all cases. The digital subtraction angiography equipment used was the DFP-60A model (Toshiba, Tokyo, Japan). Simultaneous biplane imaging was performed in most instances, excluding aortography.
Complications, which were defined as any new neurologic and systemic or local adverse symptoms during and after angiography, were recorded prospectively. Postangiography observation was performed at the completion of the procedure and on the day after the procedure. Image quality was subjectively assessed as being comparable with or inferior to images obtained with a 4F catheter by two observers (M.K., M.N.) by consensus. Real injection pressure was measured with a Mark V Plus (Medrad Inc, Indianola, PA). After the procedure, the puncture site in the groin was manually compressed for 5 to 10 minutes, and a cross bandage was applied without any weights. The first 15 patients were kept in bed for 6 hours; the last 15 patients, for 3 hours.
For all 30 patients, the angiographic techniques used were the same as with the 4F or larger catheter systems, and guidewire support was not always required during the catheterization because of the moderate stiffness of the catheter. In 22 patients, only an H1 catheter was used. In four patients, an additional H5 catheter was required to catheterize the innominate artery (one patient) or the left common carotid artery (three patients) because of tortuosity. A Berenstein catheter was used in four pediatric patients. There was no subintimal injection in any patient. In no instance did the catheter tip slip down into the aorta because of the injection jet of the contrast material. No neurologic or local or systemic complications were observed in any case. No local hematomas in the groin area were observed in either group with a 3- or 6-hour period of postprocedural bed rest.
All targeted brachiocephalic vessels (total, 92; average, 3.1 vessels per patient) were catheterized successfully except for the right vertebral artery in one instance (98.9% success rate), in which case the innominate arterial injection gave sufficient information about the right vertebral artery. In most cases, common carotid injection was performed, but in 11 patients, selective internal and/or external carotid injection also was performed successfully.
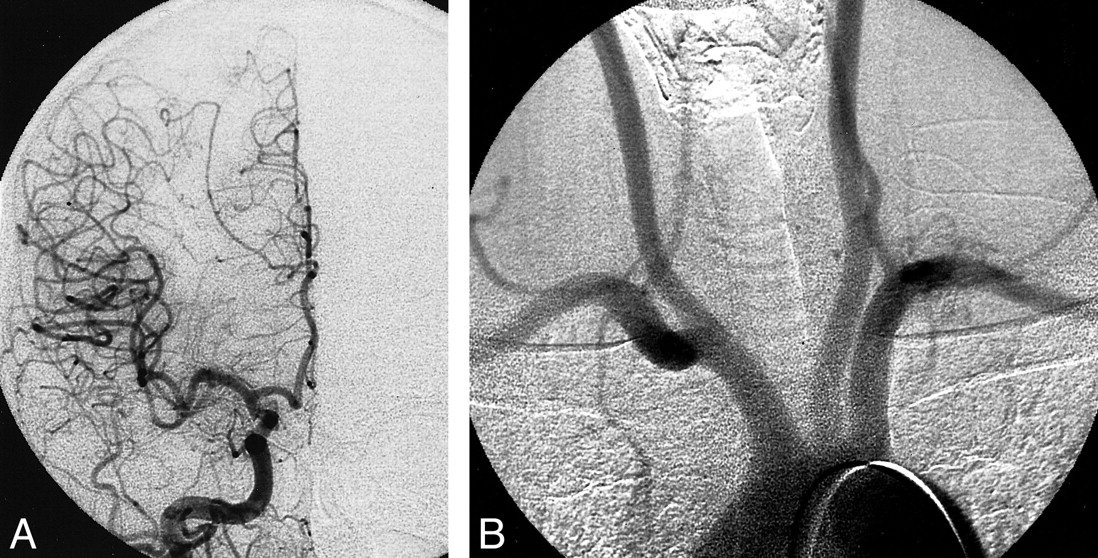
The injection pressure with a 3.2F catheter was recorded for 26 patients. The maximum injection pressure was generally constant at the given flow rate and total volume of contrast material. Detailed data about injection pressure, flow rate, and volume of the contrast material are shown in the Table. Aortography was performed with 10 mL of contrast material at the rate of 6–8 mL/s in 10 patients in which the prefixed pressure limit restricted the injection pressure up to 800 psi for safety. At 800 psi, about 5.6 mL/s of the contrast material could be injected through the 3.2F catheter. The quality of the cerebral angiogram (Fig 1A) was judged as being comparable to that obtained with a 4F catheter in all cases. Aortograms could also be performed with a 3.2F catheter (Fig 1B), and they provided the same image quality as that with a 4F catheter.
Contrast material injection data

fig 1. A 48-year-old man with a right falx meningioma. Cerebral and aortic angiography performed with a 3.2F catheter system.
A, Cerebral angiogram from a right common carotid injection (frontal view). Contrast material (total amount, 6 mL) was injected at the rate of 5 mL/s. Injection pressure was 601 psi.
B, Aortogram. Contrast material (total amount, 10 mL) was injected at the rate of 5.6 mL/ s. Injection pressure was 798 psi.
Discussion
Although we did not compare image quality directly obtained with 3.2F and 4F or 5F catheters, we believe that the image quality with 3.2F catheters was equivalent to that with 4F or 5F catheters. This is because both catheters delivered the contrast material at the same injection rate and volume in our series. A 3.2F catheter also can be used for aortograms by placing the tip several centimeters proximal to the orifice of the innominate artery in the ascending aorta. A pigtail catheter was not required. In 1986, the total volume in an arch study (meglumine iothalamate 60%) was 20–30 mL injected at rates of 10–15 mL/s with a 5.0F H1 catheter without side ports (2). Now, we can obtain digital subtracted aortograms with a total volume of 10 mL injected at the rate of 5–6 mL/s through an end-hole 3.2F catheter.
We had thought that a larger catheter allowed more stable manipulation for cerebral catheterization, but even a 3.2F catheter allows stable manipulation and does not require additional time for catheter manipulation. In only four of our patients did an H1 catheter have to be changed to an H5 catheter, and this often happens with a 4F or 5F H1 catheter. In our series, a 3.2F catheter was used for three pediatric patients younger than the age of 5 years without complications. We believe, therefore, that this 3.2F catheter can be used from pediatric to older patients, indicating no discrimination in catheter selection by age. Thus, we might call this “a catheter for all ages.”
In conclusion, our preliminary experience indicates that this 3.2F diagnostic catheter system can be used for cerebral angiography as the standard catheter for all ages.
Footnotes
1 Address reprint requests to Masaki Komiyama, Department of Neurosurgery, Osaka City General Hospital, 2-13-22, Miyakojima-Hondori, Miyakojima, Osaka 534-0021 Japan.
References
- Received January 8, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.