
Abstract
BACKGROUND AND PURPOSE: Experience with intravenous abciximab to manage thromboembolism during treatment of ruptured intracranial aneurysms is limited. We present our experience in 13 patients.
METHODS: We retrospectively reviewed all patients with thromboembolic complications during endovascular management of ruptured intracranial aneurysms. Thromboembolic complications were treated with intravenous abciximab. We recorded patient and aneurysm demographics, aneurysm occlusion, drug therapy, complications, and outcomes.
RESULTS: World Federation of Neurological Surgeons Grades were 1 or 2 in 11 patients (85%). Median time from diagnostic angiography to treatment was 1 day. Ten (77%) aneurysms involved the anterior or posterior communicating artery, and one each occurred in the posterior inferior cerebellar artery, middle cerebral artery, and basilar regions. Eleven aneurysms were <10 mm. Five were incompletely occluded (0%–90% treated) at the time of the complication. Thromboembolic complications were at the coil-ball/parent-artery interface in nine patients (69%). Two were associated with coil-loop prolapse; one was prophylactically treated without evidence of thromboembolism. Five patients (38%) had distal complications; one also had a proximal thrombus. All patients received an intravenous bolus of abciximab (5–10 mg in 92%) without infusion. Postprocedural recanalization was complete in eight (62%) and partial in four (31%). Eleven patients (85%) had a Glasgow Outcome Scale score of 1 at 3 months. One had a poor outcome (GOS4). One died following additional coiling after abciximab administration, though this intervention was uneventful in three others.
CONCLUSION: Abciximab completely or partially treated thromboembolic complications arising during coiling of ruptured aneurysms. Further coiling should be performed with extreme caution and needs to be decided on a patient-by-patient basis.
Abciximab (Reopro; Eli Lilly, Indianapolis, IN) is well described as a rescue treatment for thrombus in the context of unruptured aneurysms (1). The Fab monoclonal antibody fragment inhibits platelet blockade through the glycoprotein IIb/IIIa receptor. The effect occurs within 10 minutes, and though it may be reduced, it persists for as long as 48 hours after the cessation of treatment (2). Although we know of no well-controlled studies to evaluate the risk of hemorrhage in the neurovascular interventional setting, no significant increase in hemorrhagic risk was seen in the Abciximab in Ischemic Stroke study (3), in the Evaluation of c7E3 for the Prevention of Ischemic Complications (4), or in isolated case reports in which abciximab was used as a rescue treatment in carotid and/or vertebrobasilar angioplasty and in vertebrobasilar thrombosis (5–7).
However, reports of increased systemic hemorrhage-related complications in cardiac patients (8) have tempered its application in the treatment of procedure-related thrombosis in the context of ruptured aneurysms. To date, one case report and one series of five patients have described the use of abciximab for thrombotic complications arising during the treatment of acutely ruptured intracranial aneurysms (1, 9). In the series, four patients were treated with intra-arterial abciximab 5 mg (1), supplemented with a 17-mg intravenous infusion in one. The fifth patient was treated with a 20-mg intravenous infusion for 10 minutes, without subsequent infusions. Another case report described delayed (12 days) treatment of a ruptured aneurysm, which was similarly treated (10). In all of these reports, the aneurysms were initially completely occluded before abciximab was administered. In one patient, use of abciximab was the last resort after heparin, intravenous nonsteroidal (Ketorolac), and urokinase were given (9). We describe the use of abciximab in 13 patients with ruptured aneurysms who developed thrombotic complications during coiling while receiving therapeutic doses of heparin.
Methods
We retrospectively evaluated 13 patients in a 4-year period who developed thrombotic complications during endovascular treatment for aneurysm rupture who were treated with intra-arterial abciximab. All clinical notes and radiologic images were reviewed. The following data were collected: patient demographics (age, sex), aneurysm morphology (size, location, and number), procedural therapy (anticoagulant and abciximab use and route), time to clot dissolution, number of coils inserted, procedural complications, and Glasgow Outcome Scale (GOS) scores at discharge.
Two operators were responsible for aneurysm embolization and followed a standardized protocol consisting of an initial bolus of intravenous heparin before the insertion of the guiding catheter. Then, hourly intravenous boluses of heparin 1000 U were given with the aim of elevating and maintaining the patient’s activated partial thromboplastin time (aPPT) at 2–2.5 times the baseline value.
Results
The Table summarizes the data collected. All 13 patients (eight women, five men) received abciximab. Their median age was 56 years (range, 28–79 years). Seven patients had a World Federation of Neurological Surgeons (WFNS) grade of 1 (54%); four (31%), grade 2; and two (15%), grade five (one of which improved to grade 2 before the procedure). Median times were 4 days (range, 4–23 days) from ictus to intervention but 1 day from diagnostic angiography to treatment. Aneurysms were in the anterior communicating artery (ACOM, five patients [38%]); posterior communicating artery (PCOM, five patients [38%]); and one (8%) each in the posterior inferior cerebellar artery, middle cerebral artery, and basilar regions. Eleven aneurysms were <10 mm and two were 12–15 mm. Mild-to-moderate spasm was present in four patients (31%) at the time of treatment.
Patient Demographic Data
The coils used were a combination of bare platinum and biologically active coils. A median of five coils (range, 0–13) were placed in the aneurysm before abciximab administration. Eight aneurysms were completely occluded at the time of thromboembolic complication, whereas five were incompletely occluded. The latter were a partially treated basilar tip, two ACOM and two PCOM aneurysms with estimated occlusions of 20%, 60%, 80%, 90%, and 0%.
One patient had a major thromboembolic event during preprocedural diagnostic angiography, and abciximab was given on an emergency basis before the patient’s ruptured PCOM aneurysm was treated. The mean periprocedural aPTT was 209 seconds. Thromboembolus occurred at the parent-vessel/coil interface in nine patients (69%), two of whom had prolapse of a single coil loop. Five patients (38%) had distal embolic complications, including one who also had a proximal thrombus. One patient with coil prolapse was prophylactically treated without evidence of thromboembolism.
All patients received an intravenous bolus of abciximab without infusion as first-line treatment. The only exception was one patient, who was first treated with intravenous aspirin, which had no effect. Doses of abciximab were 5 mg in seven patients, 10 mg in four patients, and 20 and 7.5 mg in one patient each. Recanalization at procedural termination was complete in eight (62%) and partial in four (31%). Three of the five patients who had incomplete occlusion at the time of the thromboembolic complication received two to four additional coils. Four patients received intravenous aspirin in addition to abciximab, two received intra-arterial papaverine 30 or 70 mg, and one received intra-arterial nimodipine 4 mg.
Eight patients (62%) had no new postprocedural abnormality due to thromboembolic complications, as shown on CT scans, though three of these patients had transient symptoms after the procedure. Eleven patients (85%) achieved a GOS of 1, including three (23%) with initially symptomatic and imaging-positive infarcts. One patient with an 80% occlusion of an ACOM aneurysm received two additional coils after abciximab administration, but coil-related rupture occurred with the final coil, and the patient subsequently died from severe vasospasm in the bilateral middle cerebral artery territories. One patient with an intraparenchymal hematoma after aneurysm rupture; hematoma evacuation and shunt placement was required 2 days after coiling because of a decline in his Glasgow Coma Scale (GCS) score. Repeat imaging demonstrated increased perihematomal edema, but no increase in the size of the hematoma. He achieved a GOS of 4 (initial WFNS grade of 2) at 3 months, consistent with his parenchymal hematoma and clinical course.
Representative Case 1
A 29-year-old woman presented with a grand mal seizure during the second stage of labor with her first child, as its head was being delivered. The patient recovered consciousness and had headache with vomiting. Her GCS remained at 15, with no neurologic deficit. Having been normotensive during labor, she was hypertensive at this time. Head CT demonstrated subarachnoid blood, ventriculomegaly, and blood in the fourth ventricle. She was transferred to her local neurosurgical unit 12 hours after ictus. Triple-H therapy was started.
The following morning, 24 hours postictus, diagnostic angiography was performed with local anesthesia. The images demonstrated a 9-mm right-sided PCOM aneurysm associated with a fetal posterior cerebral artery.
The patient underwent embolization of her aneurysm. Moderate spasm of the right internal carotid artery (ICA) was present at this time. The aneurysm was completely occluded with six coils (Matrix; Boston Scientific, Natick, MA). At the end of the procedure, the right A1 showed no flow (Fig 1A), and direct cannulation of this vessel was not possible because of spasm. A total of 20 mg of intravenous abciximab was administered, with intra-arterial nimodipine 4 mg, and the vessel reopened (Fig 1B). Images demonstrated no filling defects at the end of the procedure, and the patient awoke without deficit.
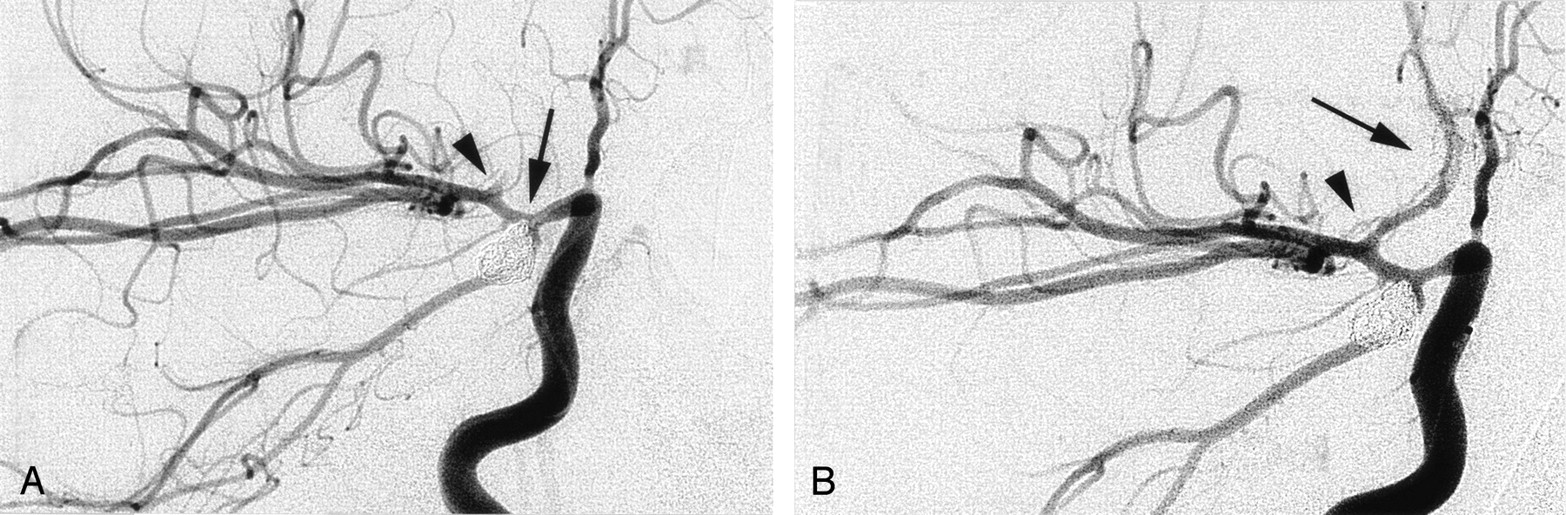
Anteroposterior oblique views, selective right ICA injection.
A, Right PCOM aneurysm in association with fetal-type PCA after the insertion of six coils. Image shows minor projection of coils into the terminal ICA (arrow), which demonstrates spasm. Contrast material irregularly fills the proximal ACA, with nonvisualization of the distal ACA. These findings are consistent with thrombus (arrowhead).
B, Immediately after the intravenous injection of abciximab 20 mg, the A1 segment of the ACA (arrowhead) is completely recanalized. Minor filling defect in the proximal A2 (arrow) dissipated shortly afterward.
Over the next 4 days, the patient had transient left-sided weakness, which affected her leg on days 2 and 4 and her arm and leg on day 5. The signs completely resolved between episodes; this observation was consistent with hypoperfusion, presumably that related to vasospasm. She was transferred from the neurosurgical high-dependency unit to the intensive care unit for continued inotropic management. After a 12-day admission in the intensive care unit, the patient was discharged to the ward. At this time, she had a mild deficit in sensation and proprioception on the left side but no weakness. Brain CT showed no infarct, and brain scintigraphy showed uniform tracer activity. After a short inpatient stay in a rehabilitation unit, she completely recovered.
Representative Case 2
A 56-year-old woman had sudden-onset headache and collapsed at home. She was examined at her local hospital and sent home. That evening, she became confused and was examined at a different hospital, where CT demonstrated a subarachnoid hemorrhage with mild ventricular dilatation and blood in the ventricular system. She was transferred to the neurosurgical unit early in the morning of postictus day 1.
On admission, the patient was mildly confused but able to obey commands. She had no focal neurologic deficit. Triple-H therapy was started. The patient was a smoker with a history of depression. An angiogram obtained with local anesthesia 2 days after ictus demonstrated a 6 × 4-mm aneurysm of the right ACOM that pointed anteromedially. No spasm was evident.
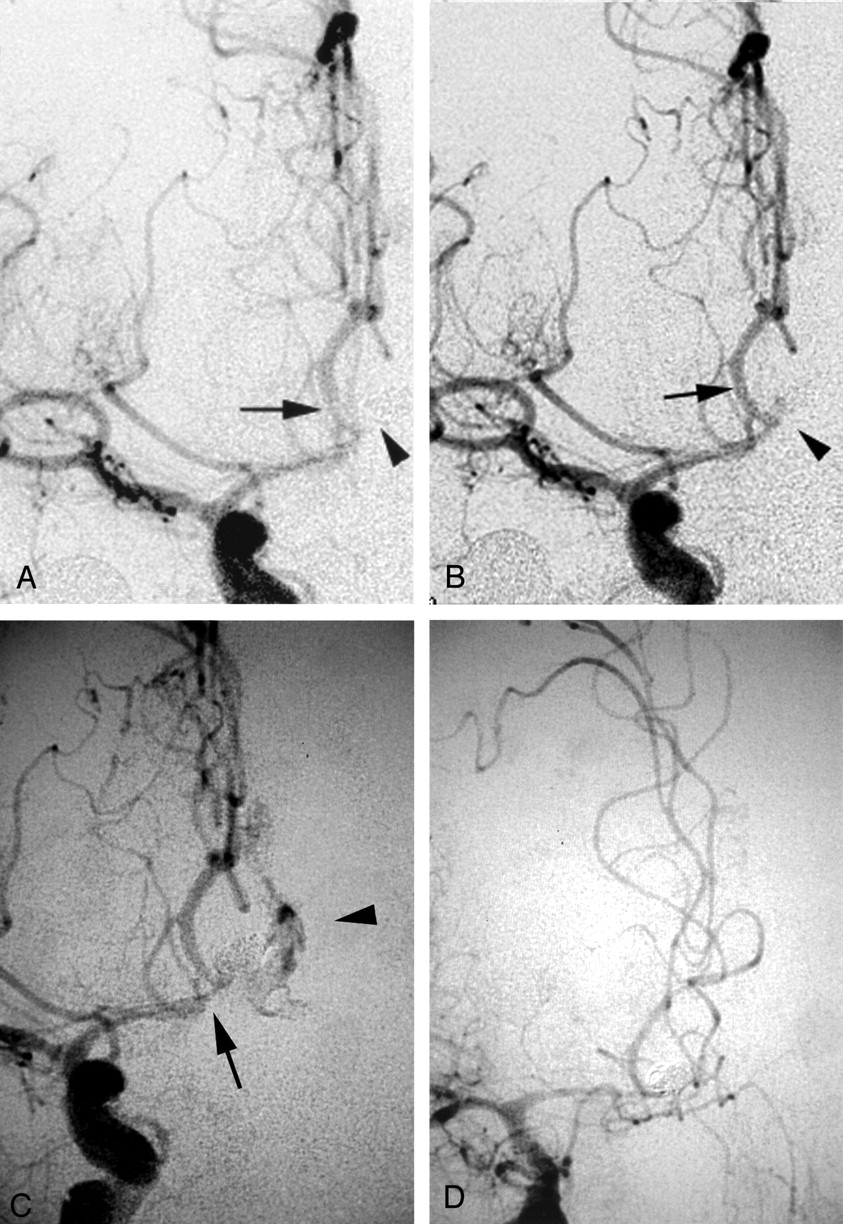
On postictus day 4, the aneurysm was treated with coils with the patient under general anesthesia. No spasm was noted at the beginning of the procedure, but catheter-induced A1 spasm was seen during catheterization of the aneurysm. After the first two coils were inserted (Cerecyte; Micrus Corporation, Sunnyvale, CA) angiography showed a little thrombus in the right A1. This rapidly and spontaneously cleared, and an additional coil was inserted. Angiography then demonstrated thrombus in the right A1 and A2 (Fig 2A). Abciximab 5 mg and aspirin 500 mg were administered intravenously, with a substantial improvement in angiographic appearances (aPTT of 240 seconds; baseline aPPT, 87 seconds) (Fig 2B). A fourth coil was inserted, and increased right A1 vasospasm was noted. A fifth coil (2 × 2 cm) was inserted but required repositioning once because of microcatheter and coil prolapse in its final 2–3 mm. Angiography unexpectedly revealed aneurysm rupture (Fig 2C). Heparin was reversed with protamine 50 mg, and the coil was detached. No further leakage was demonstrated, and the aneurysm was completely occluded, as shown on angiograms. Marked spasm was observed in the right anterior and middle cerebral arteries (Fig 2D). The procedure was terminated, and the patient underwent CT, which demonstrated no change in ventricular size or intracranial blood load.

Anteroposterior views.
A and B, Selective right ICA injection after the insertion of three coils. Before abciximab treatment (A), thrombus is seen at the neck of the aneurysm (arrowhead) and in the proximal right A2 segment of the right anterior cerebral artery (arrow). After abciximab (B), improvement in both is noted.
C and D, Selective injection after the insertion of five coils and aneurysm rupture. In C, thrombus (arrow) is present in the distal A1 segment and ACOM, with adjacent extravasation of contrast material (arrowhead). After heparin reversal, repeat angiogram in D demonstrates aneurysm occlusion, cessation of extravasation, and absence of thrombus, but marked vasospasm is present.
The patient was electively ventilated in the intensive care unit for 2 days, after which sedation was withdrawn. A further CT scan demonstrated bilateral, focal frontoparietal infarcts. Three days after coiling, her GCS score improved to 7, but her level of consciousness subsequently deteriorated (GCS score of 3) despite aggressive treatment. She developed fixed, dilated pupils, and ventilation was withdrawn on day 6.
Discussion
Thromboembolic complications are reported in 5%–10% of patients treated endovascularly (11–14), though permanent deficit is less frequent, with rates of 1%–5% (15–17). Associations between the development of thrombosis, the size of the catheter/introducer, and the duration of the procedure (18–20) have been established. Thrombotic complications of coiling are most commonly recognized as distal emboli (11, 15) on check angiography and less commonly occur with a filling defect at the coil-ball/parent-artery junction (1, 9). However, we had an increased prevalence of local thrombosis. Large aneurysm diameter and coil protrusion are independent risk factors for postprocedural thromboembolic events (16).
Factor VIII mediates the mechanism of local thrombus formation, resulting in fibrinogen deposition on the catheter or coil and leading to platelet-potentiated thrombus formation (21). The mechanical effect of the guidewire and catheter on the endothelium and the inherent thrombogenicity of catheters and wires are other factors (22). Although electrothrombosis was previously considered a contributor to thrombus formation (23–27), its role at the time of coil detachment has not been established (28).
Treatment of thrombus formation may be local (mechanical clot extraction and/or disruption [29]), or systemic (blood pressure elevation, intravascular volume expansion) (11). Pharmacologic approaches include intra-arterial aspirin, intra-arterial fibrinolytics (29), intravenous aspirin (29, 30), intravenous heparin (31), and abciximab (10, 31), or a combination (9).
Treatment of thrombotic complications in ruptured aneurysms requires a fine balance between maintaining intra-aneurysmal occlusion (to which coil packing and thrombosis contribute) (32, 33) and lysis of the thrombus in the parent artery. The use of fibrinolytics in ruptured intracranial aneurysms has variable outcomes. Cronqvist et al (29) reported a poor outcome (GOS score of 5) in three of six patients with urokinase-related hemorrhage. Two of the patients had aneurysm rerupture, whereas the third developed hemorrhagic transformation of an ischemic lesion. Whether complete embolization was achieved in the first two patients before urokinase administration is unclear, though one had marked intraluminal aneurysmal filling 3 days after thrombolysis. The authors concluded that fibrinolytics should be administered only in patients with sufficiently embolized aneurysms. On the basis of this report, several other authors have subsequently emphasized the need for the aneurysm to be completely occluded before the administration of abciximab (1, 9, 10). However, we are unaware of peer-reviewed evidence demonstrating an increase in rerupture rates in unsecured aneurysms in this context. Our experience in five cases in this series is contrary to these recommendations. Although two patients had high degrees of packing (80% and 90%) at the time of complication, packing was poor in 2 (20% basilar tip, 60% ACOM) or untreated (PCOM). Three patients received additional coils without complication after being treated with abciximab; one had a fatal aneurysm rupture. The decision to insert further coils was made on an individual basis by taking into account the degree of packing and the configuration of coils relative to the fundus and site of rupture. Therefore, we observed no increased hemorrhage with partially occluded (20%–90%) or unoccluded aneurysms in four patients. However, because of the fatality, caution should be exercised if further aneurysm coiling is expected after abciximab administration.
Although its effect on ruptured aneurysms is unknown, abciximab impairs platelet cross-linking and aggregation (35), promotes fibrinolysis, and inhibits platelet-dependent prothrombin activity. These effects may disrupt the newly formed thrombus, sealing the recently ruptured aneurysm to prevent intra-aneurysmal thrombus formation after coiling and to stop flow from penetrating the aneurysm, both of which are risk factors for rerupture. Its action is prolonged and, though reduced, it may persist as long as a week (36) after administration. In contrast to heparin, abciximab is not easily reversed. Despite these theoretic effects, abciximab has been used for carotid (5) and vertebrobasilar (6) rescue and for the treatment of acute stroke, without a substantial increase in intracerebral hemorrhage (3). Therefore, abciximab does not appear to have intracranial risk on par with that of thrombolytic agents.
In addition to aneurysm rerupture, the systemic effects of intravenous abciximab may increase the prevalence of groin (37) and postsurgical hemorrhage (8). Such complications may be reduced by using short-acting IIb-IIIa antagonists such as the peptide eptifibatide (Integrilin, half-life of 2.5 hours; Cor Therapeutics, South San Francisco, CA), which inhibits receptor-ligand binding, and the nonpeptide receptor antagonist tirofiban (Aggrastat, half-life of 2 hours; Merck, West Point, PA). A reduction in the aPTT from 300–350 to 200 seconds when concomitant heparin is administered has also been suggested as a means of reducing the likelihood of hemorrhagic complications (38).
Song et al (1) hypothesize that local or intra-arterial abciximab use may reduce the dose required for successful recanalization and thus reduce systemic effects. They achieved only partial recanalization with a 5-mg bolus in three patients and complete recanalization in one patient. The authors acknowledge that further work is required to evaluate the optimum dose, route, and choice of IIb-IIIa inhibitor. We used variable but predominantly low intravenous doses (5 mg in 54%) without subsequent infusion and achieved complete and partial clot dissolution in all patients. One patient, a 72-year-old woman, had a combination of hard and soft thrombus that caused near-total occlusion of the basilar tip following a vertebral dissection; this was observed at the time of diagnostic angiography immediately before emergency coiling. Abciximab immediately cleared the soft basilar thrombus, but the focal thrombus persisted at the origin of the superior cerebellar artery. This clot did not respond to attempted mechanical disruption by using the guidewire, leading us to conclude that this was hard, atheroembolic material dislodged from the vertebral artery dissection. Her PCOM aneurysm was then successfully occluded with four coils. We did not observe any treatment-related hemorrhagic complications. In fact, one of our treated patients had an intraparenchymal hematoma after aneurysm rupture, which remained unchanged despite the intravenous administration of abciximab 5 mg. The investigators in the Evaluation of c7E3 for the Prevention of Ischemic Complications concluded that a bolus followed by an infusion was more effective than a bolus alone (37). However, like others (1, 9), we found that a bolus dose may suffice in the context of first-line abciximab for thromboembolic complications of coiling. We suggest that an infusion may potentially confer an additional and unnecessary risk of hemorrhage. Postprocedural anticoagulation can be effectively maintained with heparin followed by aspirin and/or clopidogrel.
Conclusion
We demonstrated the safe and effective use of a bolus of abciximab as first-line treatment in patients with ruptured aneurysms and procedure-related thrombotic complications. In 92% of our patients, no complication occurred with abciximab, though five aneurysms were only partially or completely occluded. Recanalization was favorable in 92%, and most patients achieved a GOS score of 1. We caution against the insertion of further coils after abciximab administration, as this led to aneurysm rupture and death in one patient.
References
- Received December 14, 2004.
- Accepted after revision January 26, 2005.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Intra-arterial versus intravenous abciximab therapy for thromboembolic complications of neuroendovascular procedures: case review and meta-analysis
- Rescue Treatment of Thromboembolic Complications during Endovascular Treatment of Cerebral Aneurysms: A Meta-Analysis
- Rescue Treatment of Thromboembolic Complications During Endovascular Treatment of Cerebral Aneurysms
- Adjunctive use of eptifibatide for complication management during elective neuroendovascular procedures
- Intra-arterial abciximab for the treatment of thrombus formation during coil embolization of intracranial aneurysms
- Abciximab Is a Safe Rescue Therapy in Thromboembolic Events Complicating Cerebral Aneurysm Coil Embolization: Single Center Experience in 42 Cases and Review of the Literature
- Clinical and Angiographic Follow-up of Ruptured Intracranial Aneurysms Treated with Endovascular Embolization