
Abstract
Summary: Spontaneous intracranial hypotension in a 37-year-old man with intractable headaches was diagnosed on MR imaging. A generous CSF leak was identified at C2 on CT myelography. Successful treatment was performed with CT-guided blood patch at the leakage site after the patient had failed 2 lumbar blood patches. Imaging-guided precise placement of the blood patch is safe and recommended when a lumbar blood patch away from the leakage site could be ineffective.
Spontaneous CSF leak is a recognized cause of intracranial hypotension, and the syndrome of spontaneous intracranial hypotension has been described as a distinct entity (1–3). The symptoms may include postural headaches, neck stiffness, nausea, vomiting, visual symptoms, and cranial nerve pareses (typically VI) (3). Different diagnostic techniques have been used, and the imaging findings have been described on CT, MR imaging, and radionucleotide imaging (1–4). Angiographic features associated with the syndrome have also been documented (5). The treatment options range from conservative supportive measures to epidural blood patch (3). Epidural blood patch has traditionally been performed in the lumbar area, with few cases reported in the thoracic and lower cervical spine (1, 3, 4). We report the clinical and imaging presentation of a case of intracranial hypotension caused by spontaneous CSF leak originating at the C2 level, treated by an epidural blood patch performed at the site of the leak.
Case Report
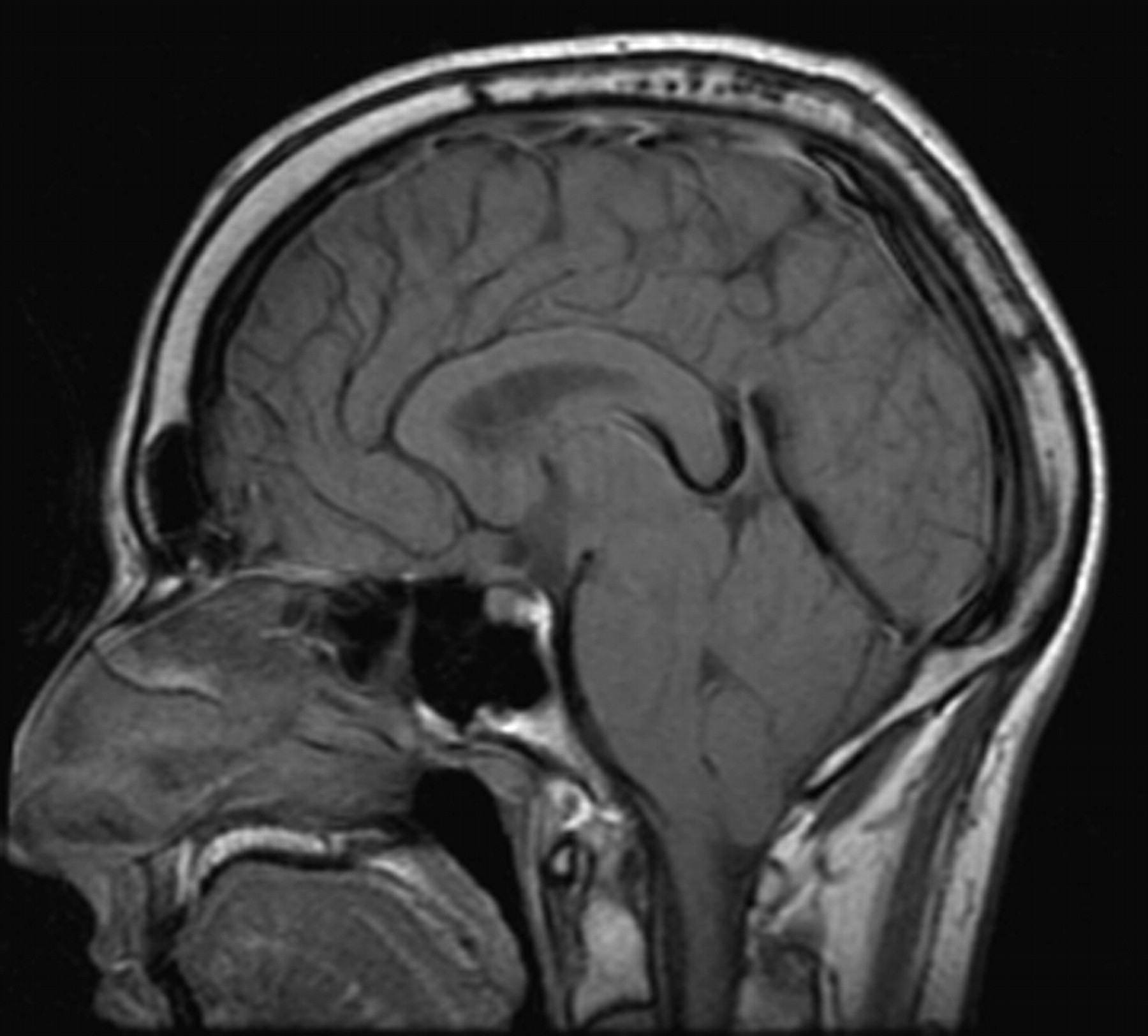
The patient was a 37-year-old man with a 1-month history of progressive intractable headaches and neck stiffness. The headaches were relatively relieved in the supine position. MR imaging of the brain performed at that time showed tonsillar ectopia of at least 8 mm, extending almost to the arch of C1 with a peglike appearance (Fig 1) and diffuse dural enhancement (Fig 2). A thin subdural hygroma was seen over the high right frontal and parietal convexity. A diagnosis of intracranial hypotension was considered. The patient underwent CT myelography of the entire spinal column, which localized a generous leak at the atlantoaxial level with contrast extravasation in the lateral epidural space on the left side (Fig 3). The patient did not have a history of trauma, and there were no historical or physical findings of an underlying connective tissue disorder. Initial treatment included bedrest and supportive measures. He also underwent 2 lumbar epidural blood patches, separated by 1 month, with no relief in his symptoms. Because of the large size of the leak and persistent progressive symptoms despite 2 lumbar blood patches, a direct cervical blood patch was planned with the final option being surgical repair in case of failure.

Midsection sagittal T1-weighted image obtained without contrast material shows tonsillar descent almost to the arch of C1.

Axial postcontrast T1-weighted (A) and coronal postcontrast fast spoiled gradient-recalled echo (B) sequences show diffuse meningeal enhancement.

Axial thin-section CT images obtained through the C1-C2 (A) and the C2 (B) levels show epidural contrast material accumulation on the left side, with the possible site of leakage at the C1-C2 level.
The procedure was performed under CT guidance. After placing the patient prone on the CT gantry, we guided a 22-gauge coaxial needle to the left lateral epidural compartment at the mid-C2 level. The needle was positioned adjacent to the thecal sac, matching the site of the leak seen on the CT myelogram (Fig 4). Needle position was also confirmed with injection of 0.2 mL of iohexol (Omnipaque 240, Nycomed Amersham, Oslo, Norway). The blood patch was then performed with injection of the patient’s autologous blood obtained from the right brachial vein. The injection was stopped at 5 mL, at which point the patient reported an increased pressure sensation in the neck. Findings of a neurologic examination performed after the procedure were normal. The patient was kept overnight in the hospital to monitor for signs of spinal compression and was discharged the next day in a stable condition. At the time of discharge, he reported total pain relief.

Two axial CT images obtained with the patient in the prone position show needle placement in the left lateral epidural compartment at the upper C2 level (A) followed by administration of the blood patch; contrast material injected to confirm the epidural location is identified with mild flattening of the lateral thecal sac margin (B).
MR imaging of the brain performed 3 weeks after the first procedure showed near-complete resolution of the dural enhancement; however, the tonsillar ectopia was unchanged. About 1 month and a half after the initial cervical blood patch, his headache returned, though it was of a much lower intensity than the initial intractable headaches. A second cervical blood patch was then performed at the C2 level, and a total of 8 mL of autologous blood was slowly injected. The patient reported complete symptomatic relief without any recurrence up to 6 months after the procedure. Additionally, MR imaging of the brain and cervical spine performed 3 months after the procedure showed resolution of the inferior tonsillar displacement (Fig 5) as well as near-complete resolution of the dural enhancement (Fig 6).

Midsection sagittal T1-weighted image obtained without contrast material shows resolution of the tonsillar descent. This measured less than 3 mm compared with the initial measurement of 8 mm. Compare with Fig 1.

Axial postcontrast T1-weighted (A) and coronal postcontrast fast spoiled gradient-recalled echo (B) sequences show resolution of the diffuse dural enhancement. Compare with Fig 2.
Discussion
Spontaneous intracranial hypotension, as the name implies, is caused by low CSF pressure, usually secondary to an occult leak (6, 7). The most common presenting symptom is postural headaches. Association with Marfan syndrome and other connective tissue disorders has been described (8). MR imaging is the study of choice to depict the intracranial manifestations; the neuroimaging features include diffuse meningeal enhancement, acquired Chiari malformation, and subdural fluid collections (7, 9, 10).
In cases of spontaneous intracranial hypotension, the cause of the CSF leak is predominantly in the cervical or thoracic region, and the diagnosis is typically established by CT myelography or radionuclide imaging (11–13). In our patient, CT myelography was instrumental in identifying the leak site. Although supportive measures and medical therapy such as hydration, bedrest, caffeine, and parenteral fluid may provide temporary relief, a more durable treatment is to seal the site of the leak. A blood patch performed in the lumbar region, though technically easier, offers less likelihood of controlling a large leak in the cervical region. Furthermore, the volume of blood injected is much larger than if the blood patch is performed at the precise site of the leakage with imaging guidance.
Apart from raising the epidural pressure by injecting blood or saline, we believe imaging-guided blood patch at the site of the leakage enhances the sealant effect of the coagulated blood in controlling the leak. Although a lumbar blood patch performed away from the leak may temporarily control the leak by raising the epidural pressure, the leak may reopen once the pressure is dissipated. Large leaks may be difficult to control, and surgical treatment may be ultimately required. Our patient underwent 2 lumbar blood patches without any relief, and it took 2 attempts with CT guidance to achieve symptomatic and imaging resolution. In cases such as these, it is very important to precisely localize the site of leak. With current technology, imaging-guided procedures in the spine can be performed with relative safety and minimal discomfort to the patient, and in cases of cervical leaks, when time can be lost by pursuing other less effective therapies, it is reasonable to offer a cervical blood patch as the initial treatment.
References
- Received March 27, 2005.
- Accepted after revision April 25, 2005.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}