
Abstract
BACKGROUND AND PURPOSE: The response rate of vestibular schwannomas to radiation therapy is variable, and there are surgical options available in the event of treatment failure. The aim of this study was to determine whether pre- and posttreatment ADC values can predict the tumor response to radiation therapy.
MATERIALS AND METHODS: From a data base of 162 patients with vestibular schwannomas who underwent radiation therapy with gamma knife, CyberKnife, or fractionated stereotactic radiation therapy as the first-line therapy between January 2003 and December 2013, we found 20 patients who had pretreatment ADC values. There were 108 patients (including these 20) had serial MR images that included DWI allowing calculated ADC values from 2–132 months after radiation therapy. Two reviewers measured the mean, minimum, and maximum ADC values from elliptical ROIs that included tumor tissue only. Treatment responders were defined as those with a tumor total volume shrinkage of 20% or more after radiation therapy.
RESULTS: The pretreatment mean minimum ADC for nonresponders was 986.7 × 10−6 mm2/s (range, 844–1230 × 10−6 mm2/s) and it was 669.2 × 10−6 mm2/s (range, 345–883 × 10−6 mm2/s) for responders. This difference was statistically significant (P < .001). Using a minimum ADC value of 800 × 10−6 mm2/s led to the correct classification of 18/20 patients based on pretreatment ADC values. The intraclass correlation between reviewers was 0.61. No posttreatment ADC values predicted response.
CONCLUSIONS: Pretreatment ADC values of vestibular schwannomas are lower in responders than nonresponders. Using a minimum ADC value of 800 × 10−6 mm2/s correctly classified 90% of cases.
ABBREVIATIONS:
- TTV
- total tumor volume
- VS
- vestibular schwannoma
Tumors localized in the cerebellopontine angle comprise 5%–10% of all intracranial tumors.1 Vestibular schwannomas (VSs) are the most common tumors in the cerebellopontine angle, accounting for 80% of all tumors there.2,3 Epidemiologic data of VSs suggest the most common patients to be white and aged 50–60 years, with equal distribution between the sexes.4
The diagnosis of VS is suggested by symptoms that may include tinnitus, hearing loss, trigeminal neuropathy, facial nerve palsy, unstable gait, or increased intracranial pressure.5,6 High-resolution MR imaging has led to a greater number of smaller VSs being diagnosed in recent decades.7
Few studies have evaluated the appearance of vestibular schwannomas on DWI. Chuang and colleagues8 have proposed that high ADCs of VSs may correlate with Antoni type B, which is associated with a cystic tumor pattern. However, this correlation is still controversial because the reviewed literature has not proved the correlation between Antoni type dominance and cystic composition.9 Tumors with sparse cellularity (Antoni B type) are associated with higher ADC values compared with tumors with an attenuated cellularity.10
The options for managing VS include observation, surgery, and radiation therapy.11⇓⇓–14 Usually, newly diagnosed and small VSs are managed expectantly with serial imaging follow-up and observation because many tumors remain stable over long periods of time. However, up to half of the tumors grow within 5 years of follow-up.15 Studies also state, however, that a wait-and-see policy is not recommended for patients with cystic tumors16,17 because they tend to be larger and usually have a more rapid clinical evolution.6,18 Specifically, for cystic VS, surgical treatment is the best option, and it is associated with better results than radiosurgery.1 Other than in this cystic VS scenario, where the recommendation is firm, patient preference becomes paramount in the selection between surgery and radiosurgery for treatment. Both are considered appropriate, with similarly acceptable side effects and long-term success. The decision may be guided by multiple variables, such as the size at initial diagnosis, tumor growth rate on serial imaging, or patient symptoms.7,19 More reliable patient-specific predictors of outcome with therapy are needed to guide patients and physicians in this important decision.
ADC is a measure of the random motion of water molecules within a tissue, and it is calculated by using data from DWI or DTI.20,21 ADC values have been shown to be correlated with astrocytoma tumor grading and tumor cellularity.19,20 ADC measurements may serve as diagnostic and prognostic biomarkers as well as predictors of tumor response to treatment in glial tumors.22,23 Thus, ADC values are often used in treatment planning.24
The aim of this study was to determine whether the pre- and posttreatment ADC values may be associated with the response of VS to radiosurgery and to provide guidance for further study.
Materials and Methods
This single-center retrospective study was approved by the institutional review board and was compliant with the U.S. Health Insurance Portability and Accountability Act. The study took place at the Johns Hopkins Medical Institution. Patient consent requirements were waived for this retrospective study.
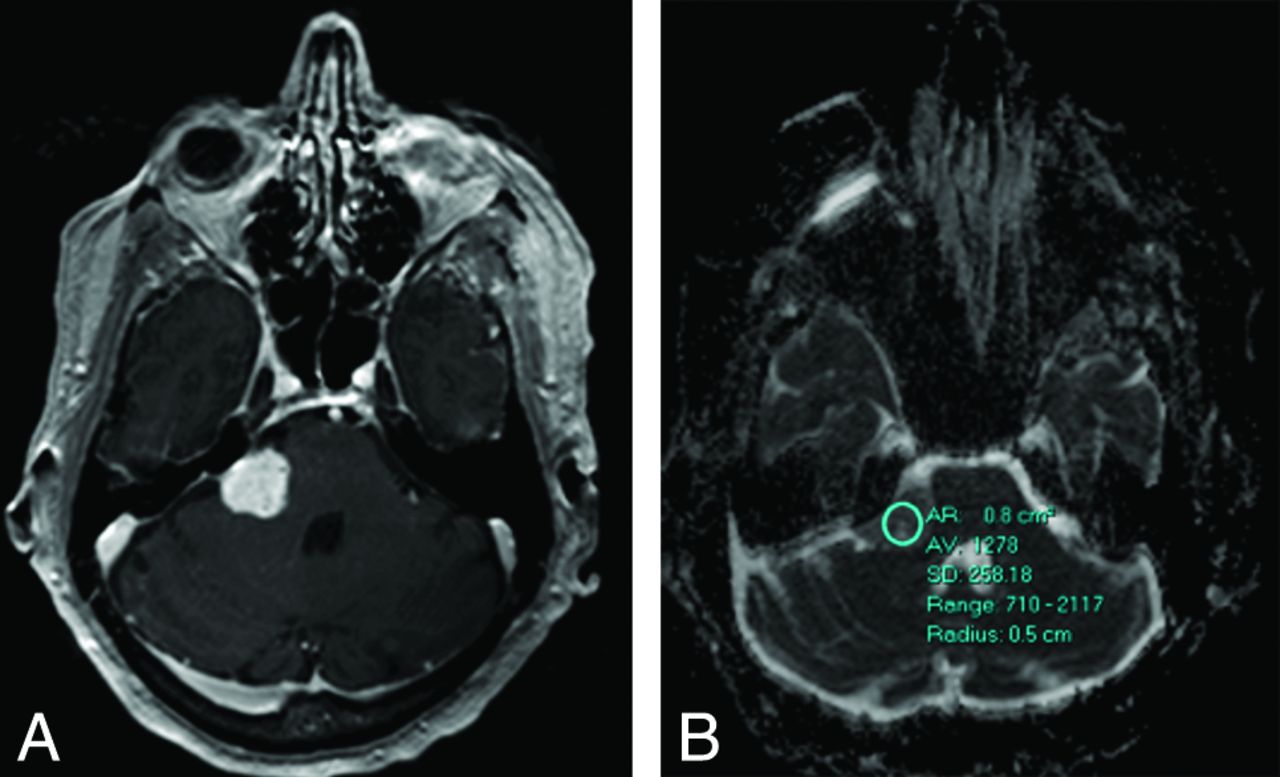
We selected patients with VS who underwent radiation therapy with gamma knife, CyberKnife (Accuray, Sunnyvale, California), or fractionated stereotactic radiation therapy as the first-line therapy at our institution between January 2003 and December 2013. Based on our initial list of 162 patients, 142 patients had MR imaging scans that either did not include pretreatment DWI scans or had artifacts that precluded measurement of ADC values. Twenty patients had pretreatment studies with diffusion-weighted sequences that allowed ADC calculations and ROI analysis. These scans took place 1–24 months before radiation therapy. The ADC values were derived by putting elliptical ROIs on the tumor from the postprocessed ADC maps derived from the DWI sequences. We used a single ROI encompassing the entire tumor on the single section that had the least amount of artifact from the adjacent (aerated) petrous/mastoid temporal bone. The ROI provided mean, maximum, and minimum ADC values from the Carestream PACS (Carestream Health, Rochester, New York) (Figs 1 and 2). Maximum, minimum, and mean ADC values were derived from DWI pulse sequences. The person performing the ADC ROI analysis was blinded to the tumor response. A second reviewer performed the ADC analyses independently and was blinded to the radiation therapy results. Based on the presence or absence of bright T2WI signal intensity and peripheral enhancement, the tumors were labeled as cystic or solid.

A, Postcontrast T1-weighted axial scan through the posterior fossa shows a right cerebellopontine angle vestibular schwannoma. B, The ADC values were calculated from an elliptical region of interest.

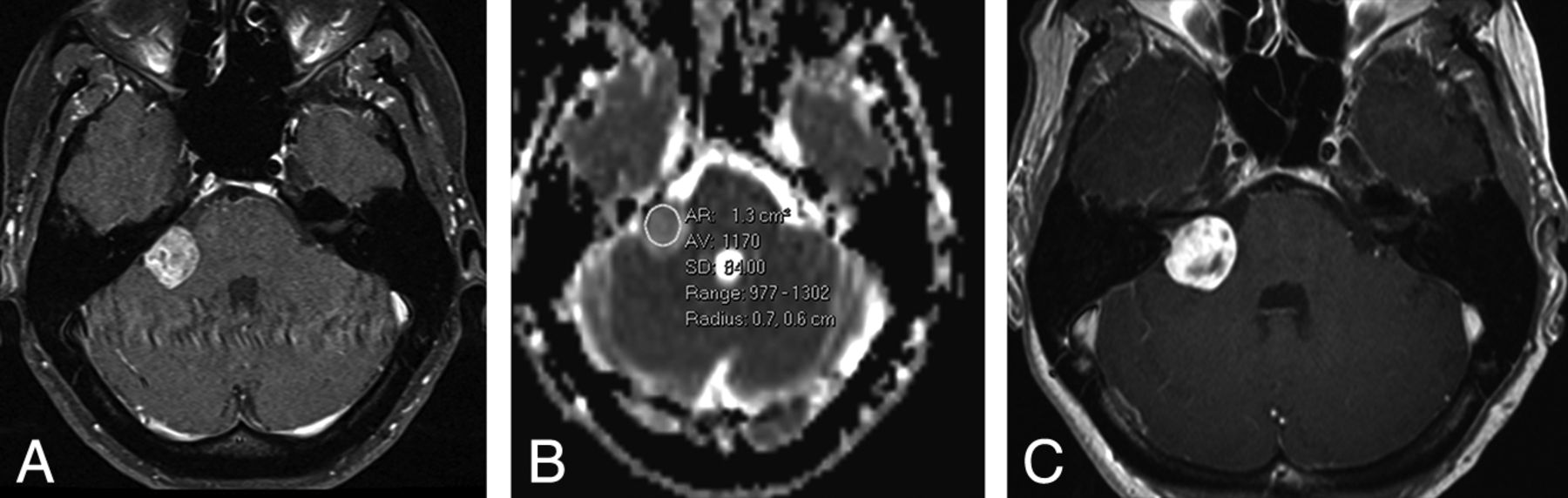
A, Right vestibular schwannoma at baseline on postcontrast axial T1-weighted scan. B, ADC calculation showing minimum value of 977 × 10−6 mm2/s. This would predict treatment failure. C, Four-year follow-up shows tumor growth on the postcontrast axial T1-weighted scan.
Standard DWI pulse sequences with 3 tensors were performed on Siemens (1.5T and 3T; Erlangen, Germany), GE Healthcare (1.5T; Milwaukee, Wisconsin), and Philips Healthcare (1.5T and 3T; Best, the Netherlands) magnets. DWI was performed with an EPI sequence with a TR/TE range of 4900–10000 ms/80–133 ms; 5-mm thin contiguous sections; FOV, 220 × 220 mm to 240 × 240 mm; and a matrix size of 96 × 96 to 192 × 192. Diffusion was measured in the 6 orthogonal directions with 2 b-values (0 and 1000 seconds/mm2) with automated postprocessed ADC maps. MR imaging studies were obtained on 1.5T (84%; GE Healthcare, Siemens, or Philips Healthcare) or 3T scanners (16%; Siemens or Philips Healthcare).
Single-session radiosurgery was performed with Leksell Gamma Knife Perfexion (Elekta Instruments, Stockholm, Sweden). Fractionated stereotactic radiation therapy was linear accelerator-based, using either the BrainLAB (BrainLAB, Feldkirchen, Germany) or Pinnacle (Philips Healthcare) treatment planning system.
To further evaluate the role of ADC values as a predictor of therapy response, we sought to collect the ADC values during the follow-up period after radiation therapy. Of the 162 patients evaluated, 54 patients were excluded due to absent or nondiagnostic ADC maps. The ADC values of 108 patients were collected during the follow-up period, from 2–132 months after the date of radiation therapy.
Tumor response was defined as a tumor total volume (TTV) shrinkage of 20% or more after radiation therapy. The tumor total volume was derived by subtracting the follow-up volume from the initial tumor volume and dividing by the initial tumor volume. This value was chosen based on previous work by Plotkin et al,25 who proposed a tumor volumetric reduction of 20% to define treatment response, based on pre- and posttreatment tumor volumes. The TTV for each patient was obtained from a previous research project that evaluated the VS volumetrically.26 The volumetric analysis was performed by a 3D semiautomated quantitative assessment of TTV, and the follow-up was defined as the time from the last radiation therapy session to the date of the most recent MR imaging study obtained in our institution.26
We also measured the longest dimension of the tumor in axial, craniocaudal, or anteroposterior dimension. We used electronic calipers to measure the largest diameter of the lesion from axial and coronal images.
Statistical Analysis
Statistical analyses were performed by using Stata 12 (StataCorp, College Station, Texas). The Student t test was used to test the difference in mean ADC value between responders and nonresponders. The association between ADC values and tumor size measures was evaluated by using the Spearman correlation. Logistic regression was used to assess the pretreatment ADC values in predicting the treatment response (responders versus nonresponders), adjusting for initial tumor size. Robust option was used for variance estimates. ROC curve analyses were performed on the serial cutoff values of minimum ADC. Sensitivity and specificity and area under the curve, with 95% CI, were used to evaluate the overall classification accuracy. Intraclass correlation coefficient and κ values were calculated for the reliability test on ADC values reported by the 2 observers. For the wide range of tumor volume data, log-transformed TTV values were used for the statistical significance test and modeling. A P value of .05 or less was considered statistically significant.
Results
Pretreatment ADC Values
For the 20 patients who had pretreatment ADC values, the median follow-up was 3.54 years. Based on a TTV reduction of 20% or more as response criterion, 11 did not respond (55%) and 9 responded (45%) to treatment. The initial TTV was higher for responders than nonresponders (Table). Responders received fractionated stereotactic radiation therapy (n = 3), CyberKnife (n = 1), and gamma knife (n = 5); nonresponders received fractionated stereotactic radiation therapy (n = 2), CyberKnife (n = 2), and gamma knife (n = 7).
Characteristics of nonresponders versus respondersa
The mean of the minimum ADC values for nonresponders was 986.7 × 10−6 mm2/s (range, 844–1230 × 10−6 mm2/s; median, 944 × 10−6 mm2/s; SD, 261 × 10−6 mm2/s) and for responders, the mean was 669.2 × 10−6 mm2/s (range, 345–884 × 10−6 mm2/s; median, 747 × 10−6 mm2/s; SD, 184.0 × 10−6 mm2/s). Nonresponse status was associated with statistically significant higher minimum ADC values (P < .001). If one used a minimum ADC value of 800 × 10−6 mm2/s as the cut-point, one could distinguish nonresponders from responders in 18/20 (90.0%) patients, with the 2 outliers being responders with a minimum ADC value of 877 × 10−6 mm2/s and 884 × 10−6 mm2/s based on pretreatment ADC values. The resulting sensitivity and specificity were 77.8% and 100%, respectively. The ROC area was 0.89 (95% CI, 0.74–1.00). The minimum ADC value had a statistically significant correlation with percent of tumor size reduction (Spearman ρ = 0.71; P < .001). The logistic regression analysis showed that the pretreatment ADC values were predictive of response. The odds ratio of being a nonresponder for each 10 × 10−6 mm2/s increase of minimum ADC value was 1.32 (95% CI, 1.14–1.52) and was 1.04 (95% CI, 1.01–1.08) for the same increase in mean ADC value. When controlling for pretreatment tumor volume and the largest 2D linear measurement of the tumor, each 10 × 10−6 mm2/s increase in the mean ADC value predicted an 8% increase in the likelihood of being a nonresponder (odds ratio, 1.08; 95% CI, 1.02–1.14).
Based on the 20 patients who had baseline data, nonresponders had a smaller initial volume than responders (0.87 mL versus 2.34 mL) and similar maximum linear measurements (1.7 cm versus 1.6 cm), but the differences were not statistically significant. The correlation between pretreatment TTV and percent of tumor size reduction was not significant (correlation coefficient, 0.39; P = .09).
There was no association between mean and maximum ADC values, initial and posttreatment TTV, or linear size and response.
Reliability tests on ADC values were performed on 20 images by 2 observers. For the quantitative minimum ADC values, the intraclass correlation coefficient is 0.61. Using the cutoff of 800 × 10−6 mm2/s and making the minimum ADC values as 2 categorical scales, the actual agreement is 89.4% and κ is 0.77 (95% CI, 0.34–0.94). Based on Landis and Koch's27 seminal work (with κ values graded as follows: <0 as no agreement, 0–0.20 as slight, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial, and 0.81–1 as almost perfect), the level of agreement was substantial.
Posttreatment ADC Values
Posttreatment ADC values were available for 108 patients. There were 197 posttreatment ADC values obtained from the 108 patients. Of the 108 patients, 48 had only 1 posttreatment ADC value available. The median follow-up to assess TTV among all 108 patients was 4.96 years. Eighty-one (75%) patients received fractionated stereotactic radiation therapy, 21 (19.5%) received gamma knife, and 6 (5.5%) received CyberKnife. Based on the same response criteria, there were 56 nonresponders and 52 responders. We calculated the mean ADC values of all patients at each year, from year 1 to year 10. Repeated measure analysis on multiple ADC values observed over the years after radiation therapy did not result in any significant findings in the change/pattern of any ADC values (mean, minimum, and maximum).
Imaging Features Besides ADC Values
Of the 20 patients evaluated before treatment, 18 had solid tumors (based on homogeneous enhancement) and 2 had mixed cystic and solid tumors (predominantly solid). The T2-weighted signal intensity was graded based on comparison with cortical gray matter. Fourteen VSs were darker on T2WI than the gray matter, 2 were brighter, 2 were isointense, and 2 had mixed darker and brighter portions (the cystic and solid cases described above). None of these factors were predictive of radiation response. One mixed lesion was a responder, and the other was not.
Discussion
Small to medium-sized VSs have proved to be, in general, the best candidates for radiation therapy because of better hearing preservation, less facial nerve palsy, good tumor control, and favorable mortality and morbidity rates in patients.28,29 Ninety-two percent of patients treated with gamma knife radiosurgery have shown tumor control in a follow-up of 7 years, associated with high rates of quality of life.30 It also has been stated that fractionated stereotactic radiation therapy is associated with a tumor control rate of 97.5% and excellent quality of life (improvement of tinnitus and vertigo and low rates of hearing impairment and trigeminal and facial nerve damage).31,32 Very long-term outcome data are not available.
Studies have tried to correlate the initial imaging findings and the clinical presentation of VS with tumor natural course and/or treatment response. It has been reported, however, that clinical worsening and original VS volume and size are not able to predict tumor growth.15,33,34 Our study has shown that minimum ADC values for VS tumors, using a cutoff of 800 × 10−6 mm2/s, predict tumor response with 90% accuracy, 77.8% sensitivity, and 100% specificity. All nonresponders showed ADC values greater than 800 × 10−6 mm2/s.
As in this study, Plotkin et al25 defined a treatment response based on tumor volumetric reduction of 20% when comparing pre- and posttreatment tumor volumes. Studies based on this 20% threshold reported that 17% of tumors have pseudoprogression (see explanation below), 52% regress, and 10.6% progress.25,35 In this study, we report a 20% reduction in tumor volume in 9 (45%) of 20 patients with preoperative ADC values and 52 (48.1%) of the 108 patients. Please note that by Plotkin et al's25 definition, a stable tumor volume (no growth) would be considered absence of response, a definition to which most radiation oncologists may object.
After radiation therapy, the well-known phenomenon of transient tumor enlargement must be considered before classifying the response as treatment failure.36,37 This pseudoprogression phenomenon is often transient and tends to start 6–9 months after radiosurgery peaking in the year that follows radiosurgery35⇓⇓–38 Five percent to 10% of patients show tumor volume increase, followed by stabilization.35⇓–37,39
Failure of radiation therapy, defined as sustained tumor growth, is rare, accounting for less than 5% of cases, and has been (in the literature, but not our study) more frequently associated with large tumor volume at the time of treatment, inadequate radiation therapy dose coverage, and cystic VS.29 However, it is important to report that no guideline or consensus is available to standardize the definition of responders and nonresponders for VS management. This explains the different rates of treatment failure versus success in the literature, given the variable criteria adopted.
Microsurgery and/or additional radiosurgery are the options for treatment failure; the choice is based on the tumor size and clinical tolerance.29 Patients who have undergone salvage microsurgery after radiation therapy have experienced poorer outcomes compared with those who never received irradiation,40 and salvage microsurgery is associated with a high risk of facial nerve injury, likely resulting from the challenge of postradiosurgery fibrosis.41 It is better to get the choice of treatment at the outset rather than after a failed therapy. Hence, the goal of this study was to find parameters that will predict radiosurgery treatment response.
Because sustained tumor growth must be confirmed with sequential follow-up images after radiation therapy before determining response,29 the recommended time for tumor response assessment should be at or after 36 months.35 This is particularly important if the clinical symptoms do not correlate with the treatment response.37 It also has been proposed that VSs that enlarge beginning after 24 months usually correspond to treatment failure.35 To ensure a reliable final TTV and, thus, response classification, we selected cases from before 2013 to obtain accurate treatment response volumes (median, 3.54 years for pretreatment ADC assessment and 4.96 years for posttreatment ADC evaluation).
ADC values have been correlated with the tumor cell attenuation, with high values usually indicating low cellularity, necrosis, or cystic features.42⇓–44 We found that the minimum ADC values were more reflective of tumor response than mean or maximum ADC values, which might be useful in characterizing cystic schwannomas. Our study observed that patients classified as nonresponders had higher ADC values, whereas responders showed the opposite trend, with lower ADC values. We did not find studies in the literature based on pretreatment ADC values in VS as therapeutic predictors. Thus, we believe that our findings should lead to prospective studies regarding the use of ADC before therapy to guide treatment planning and management.
Chuang and colleagues8 have stated that ADC may be used during follow-up to assess tumor response in VS after gamma knife radiosurgery. In our study, however, the evaluation of posttreatment ADC values did not show statistically significant correlation with tumor response. After radiation therapy, the tumor tissue architecture is affected, cytotoxicity may occur, and vasogenic edema arises, leading to changes in the water diffusion within the tumor and, therefore, in ADC values.8,9,45 We believe that these phenomena may occur in the tumor architecture after radiation therapy and can lead to changes in ADC values, making them unable to predict a reliable response/nonresponse status.
This study has some limitations. Being a retrospective study, we could not control the heterogeneity of MR imaging quality, artifacts regarding ADC, the heterogeneity of DWI/DTI pulse sequences performed, and the timing of the MR imaging before the institution of radiation therapy. In addition, imaging was performed on different scanner types. In a similar fashion, there was lack of uniformity in the type of radiation therapy used (gamma knife, CyberKnife, and fractionated stereotactic radiation therapy were the modalities used). In this study, we adopted only radiologic response criteria; no quality of life assessment was used. Nonetheless, the difference in minimum pretreatment ADC values between responders and nonresponders was striking and statistically significant. Using a minimum ADC value of 800 × 10−6 mm2/s correctly classified tumor response in 90% of cases, with high (κ = 0.77) interobserver agreement.
Conclusions
It would be useful, a priori, to predict a vestibular schwannoma's likely response to radiosurgery techniques. Our study suggests that high ADC values before treatment (above 800 × 10−6 mm2/s) predict less benefit for radiosurgery. This statistically significant correlation should lead to prospective studies, using homogeneous pulse sequences and scanning techniques, confirming the value of pretreatment ADC as an important predictor for the planning and management of vestibular schwannomas.
References
- Received October 27, 2016.
- Accepted after revision January 22, 2017.
- © 2017 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.