
Positron-emission tomographic CT (PET-CT) is gaining greater acceptance in a wide variety of oncologic indications in numerous organ systems (head and neck, central nervous system, breast, gynecologic, pulmonary, lymphoma). The dual-technique capability of PET-CT, which permits direct image fusion and improves the ability to anatomically localize foci of fluorodeoxyglucose (FDG) uptake, is replacing stand-alone PET systems. There are numerous potential clinical applications for PET-CT to evaluate malignancies of the head and neck, specifically squamous cell carcinoma (HNSCCA). Potential clinical applications include pretreatment staging, treatment monitoring and evaluation of the previously treated patients.
The current literature suggests that most primary site HNSCCA with volumes >1 mL will be FDG avid. These correspond to lesions that are moderately sized T1 or greater. Tumors with volumes <1 mL may be detected with FDG, however, the sensitivity decreases with decreasing size. PET also has the ability to detect metastatic cervical lymph nodes, which may be both clinically occult and not detected by CT or MR. In light of these potential benefits, there is debate as to how to use PET-CT for the initial staging of HNSCCA. The current consensus does not support the use of CT-PET for routine staging of all newly diagnosed squamous cell carcinomas. The intent of this manuscript is to propose potential indications for performing PET-CT for initial staging of HNSCCA before treatment.
One potential application is to perform PET-CT in advanced stage HNSCCA to evaluate for occult distant metastases to the lungs or bones. The presence of pulmonary metastases upstages a patient from M0 to M1 and alters treatment intent (Fig 1). The likelihood of pulmonary metastases is low in patients with early-stage disease and the routine imaging work-up for pulmonary metastases is conventional radiography of the chest at most institutions. An argument can be made to perform chest CT in all patients with advanced stage disease; however, if a solitary nodule is identified, it is often unclear whether this is metastasis or a granuloma. PET may help in this evaluation as a FDG-positive nodule will likely require biopsy, whereas an FDG-negative nodule (>8 mm) likely indicates a granuloma, and a biopsy may be avoided.
Various studies have been performed to evaluate the diagnostic accuracy of PET-FDG for detecting metastatic cervical lymph nodes. The consensus of the current literature suggests that sensitivity ranges of 70%–90%, whereas the specificity is slightly higher (80%–95%). The negative predictive value (NPV) is approximately 90%. This is because >40% of metastatic lymph nodes are <7 mm in diameter. As a result, PET-CT has not gained widespread acceptance to be used to exclude the presence of metastases in the clinically N0 neck. In fact, there is currently no imaging study that has a negative predictive value that has been shown to be consistently >95%. It is conceivable that future advances in CT detector technology in PET-CT units will permit diagnostic CT (<2.5 mm and gantry angulation) to be performed. If so, PET-CT may have greater impact on management of the N0 neck as the NPV of this technique will increase if both studies (PET and CT) are of diagnostic quality and both yield normal results.
Numerous investigators have documented the ability of PET-CT to detect unknown primary tumors of the upper arodigestive tract. The current literature suggests that PET can detect HNSCCA in 30%–50% of patients presenting with an unknown primary tumor (Fig 2). At most institutions, PET-CT is performed after confirming the presence of metastatic HNSCCA and following a negative endoscopy. PET is usually performed before endoscopic biopsies to help improve the yield of the speculative tissue sampling. The diagnostic yield will likely increase with PET-CT because this technique improves accurate anatomic localization of areas of abnormal FDG uptake.
An area of potential utilization of PET-CT currently under investigation is in determining response to nonsurgical treatment modalities, either chemotherapy and/or radiation. Comparison of pretreatment standard uptake values to SUVs 2 weeks into treatment can allow measurement of the speed of response and the sensitivity of the tumor to the treatment technique. Poorly responsive tumors can then be treated to higher effective tumor doses of radiation, for example, or surgery can be performed. Furthermore, initial results suggest that PET-CT can be used to assist in defining primary site and nodal tumor targets for intensity-modulated radiation therapy approaches.
There are numerous professional and financial issues surrounding PET-CT that will require further discussion. Important topics that will need to be addressed include
Who should interpret PET-CT? Should these be interpreted by a nuclear medicine physician (PET-CT), the subspecialist who would usually interpret the CT (CT-PET), or some form of joint interpretation?
Should intravenous contrast routinely be given for the CT portion of the CT-PET?
How should the CT component of the PET be interpreted? Will this only be used as an “anatomic localizer,” or will all PET-CT studies need to be interpreted for unsuspected findings, which would be akin to “screening CT”?
How will we bill for PET-CT? The CT technology of earlier versions of CT-PET consisted of 2 or 4 detector rows, which were unable to obtain images to obtain thin sections (<5 mm). Newer versions of PET-CT now integrate state-of-the-art CT 16- and 64-row detector configurations, so it is possible that the PET-CT will provide diagnostic quality CT studies. Will we have one code for a combined PET-CT study; will we bill for a PET study with a modifier for the CT component, or will we independently bill for both the CT and PET components? How will this affect states that have certificate of need requirements that regulate the number of CT scanners that an institution may have at any one time?
At our institution, we are now routinely administering intravenous contrast for all PET-CT performed of the extracranial head and neck. The studies are jointly interpreted by faculty members of the divisions of neuroradiology and nuclear medicine. It is our belief that PET-CT is a useful adjunct to initial clinical staging of HNSCCA for specific indications and utilization of pretreatment PET-CT will continue to increase with advances in PET-CT technology.

T3N2 pyriform sinus carcinoma.
A, Axial PET-CT demonstrates avid FDG uptake in a right pyriform sinus carcinoma and a metastatic right cervical lymph node.
B, PET-CT of the chest shows a mediastinal mass with focal increased uptake. This was not detected on conventional radiography of the chest.
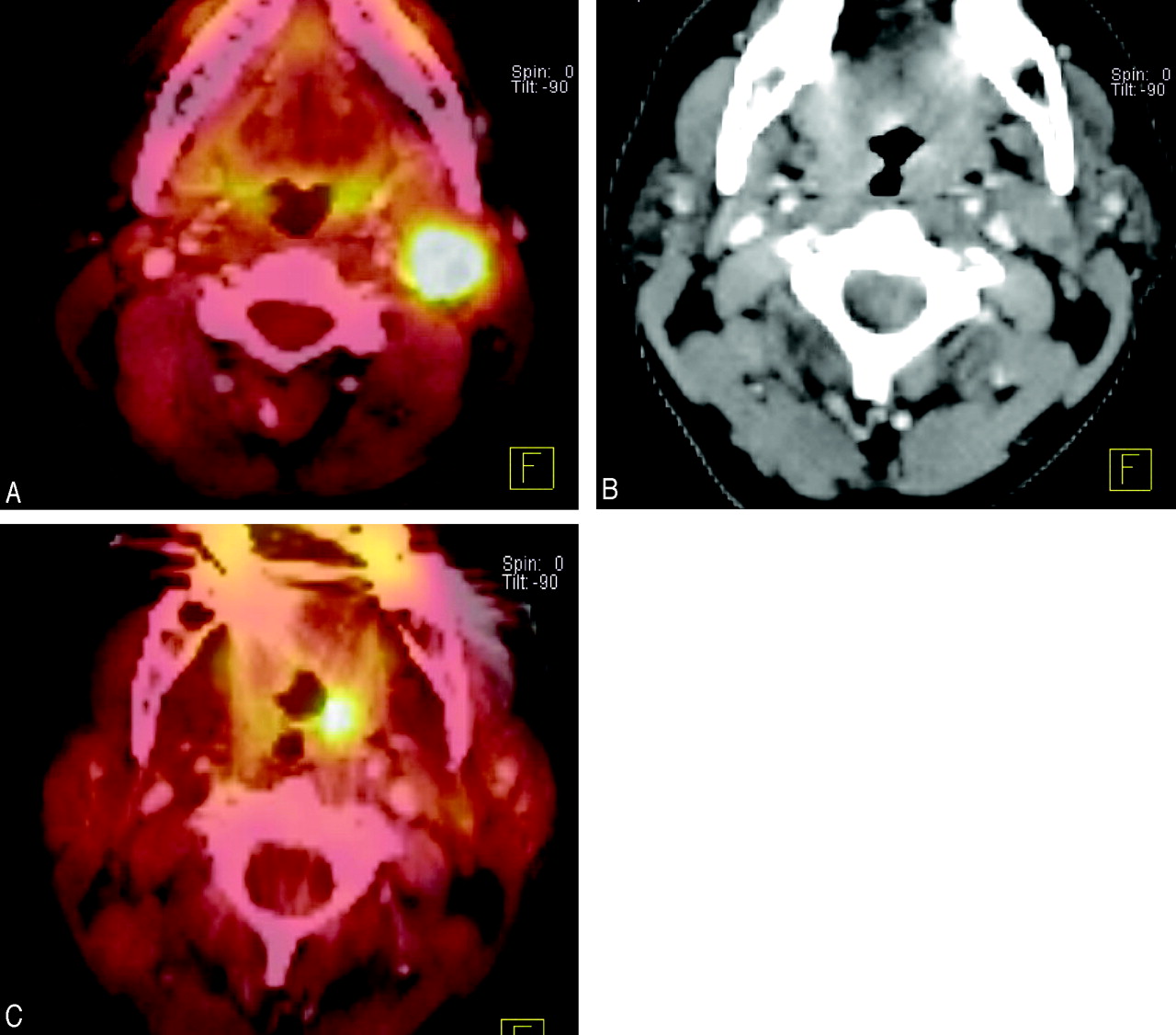
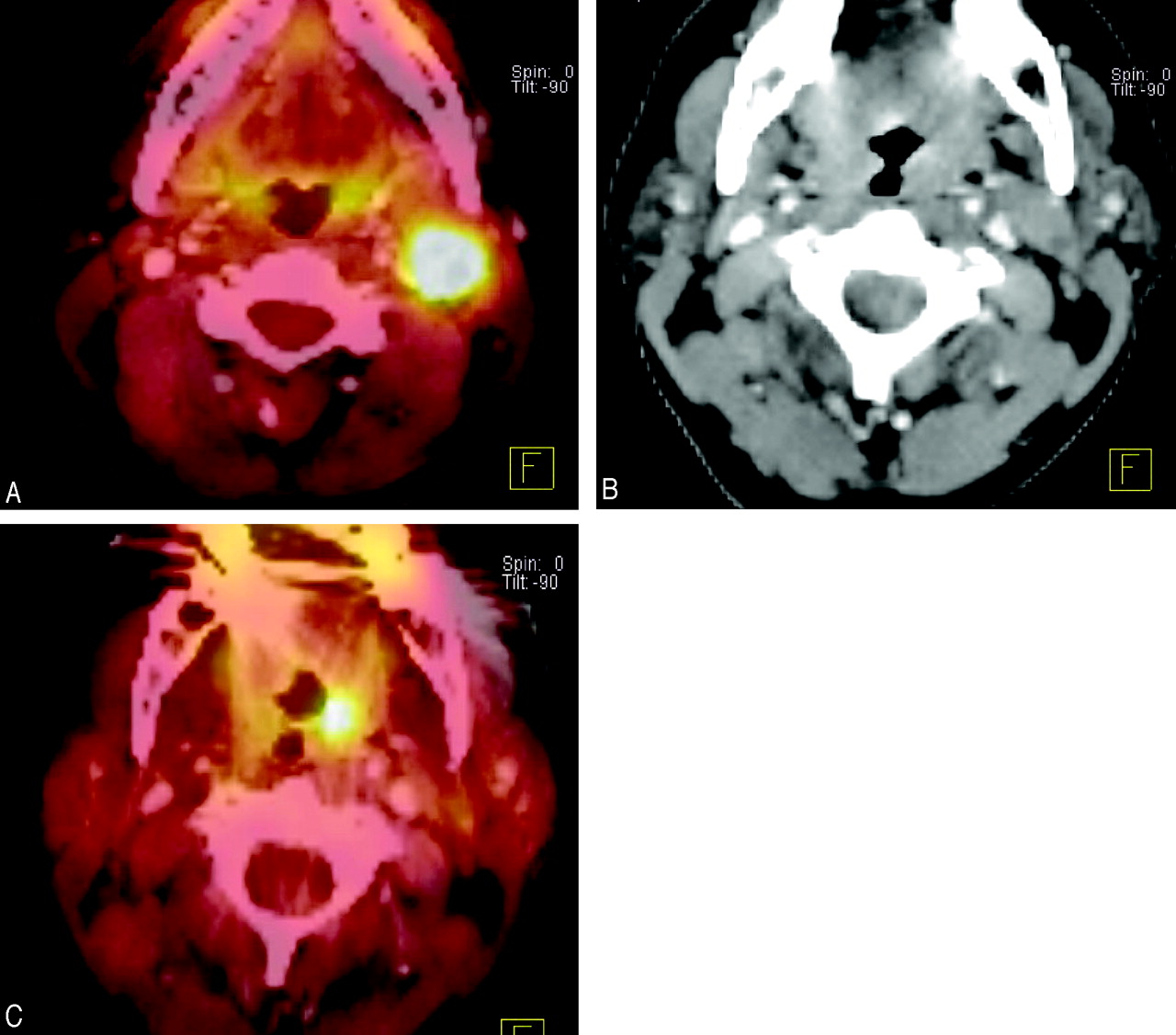
Unknown primary detected with PET-CT.
A, Axial PET demonstrates and enlarged left-sided lymph node with avid FDG uptake. Biopsy revealed squamous cell carcinoma but there was no mass seen at endoscopy.
B, Contrast-enhanced CT shows no evidence of an aggressive focal mass.
C, PET-CT demonstrates abnormal focal uptake in the left tonsil. The patient underwent a left tonsillectomy and the pathology revealed squamous cell carcinoma.
References
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}