
Abstract
BACKGROUND AND PURPOSE: There is scarcity of data on the comparative efficacy between bone biopsy drill systems across various types of bone lesions. Our aim was to investigate differences in diagnostic yield, scanning time, and radiation dose between manual and battery-powered bone biopsy systems in CT-guided biopsies of lytic, sclerotic, and infectious bone lesions.
MATERIALS AND METHODS: This was a retrospective single-center institutional review board–approved study. A total of 585 CT-guided core needle biopsies were performed at 1 institution from May 2010 to February 2019. Classification of bone lesions, location, bone biopsy system, suspected origin of primary disease, final pathologic diagnosis, diagnostic yield, presence of crush artifacts, radiation dose, and scanning times were collected. For the battery-powered system, OnControl was used. For the manual drill system, Bonopty, Osteo-site, and Laurane drill systems were used. Comparisons in lytic and sclerotic lesions and suspected discitis/osteomyelitis were made using the Fisher exact test. Subgroup analysis of the drill systems for scanning time and radiation dose was performed by 1-way ANOVA.
RESULTS: Our patient cohorts consisted of a total of 585 patients with 422 lytic, 110 sclerotic, and 53 suspected infectious lesions. The mean age was 62 ± 13 years with a male/female ratio of 305:280 for all lesions. The diagnostic yield was 85.5% (362/422) for lytic, 82.7% (91/110) for sclerotic, 50.9% (27/53) for infectious lesions, and 82.1% (480/585) for all lesions. No statistical difference was found when comparing diagnostic yields of powered drills with the manual systems for lytic, sclerotic, and infectious lesions. However, in a subgroup analysis, radiation dose and scanning time were significantly lower for powered drill compared with manual drill systems in lytic (P = .001 for both) and sclerotic lesions (P = .028 and P = .012, respectively). No significant differences were seen between the drill systems for suspected infectious lesions.
CONCLUSIONS: Our findings demonstrate that there was no statistically significant difference in diagnostic yield when comparing battery-powered and manual bone biopsy systems for CT-guided bone biopsies; however, the use of the power drill system resulted in significantly reduced scanning time and radiation dose in lytic and sclerotic lesions.
Image-guided percutaneous bone biopsies have become the preferred method of acquiring tissue biopsies from bone lesions. The procedure is noninvasive and generally well-tolerated, with lower complication rates compared with open biopsies.1⇓⇓⇓-5 Bone lesions can vary greatly in density and location, which can affect the choice of biopsy equipment used. Drill systems can be categorized into either manual or battery-powered systems. In a manual drill system, a needle is manually rotated to reach the desired depth of the lesion. Manual biopsy has been shown to have low complication rates and good diagnostic yield, ranging from 66% to 98%.3,5⇓-7 In 2007, a reusable lithium battery–powered drill device, OnControl (Vidacare, Shavano Park, Texas), was approved as an alternative without the need for a manual drill system. Prior comparative studies of drill performance in high-density bone lesions have shown that the battery-powered drill may offer greater ease of use with higher diagnostic yield.8⇓-10
However, there is scarcity of data when it comes to assessing the comparative efficacy of these drill systems in lytic and suspected infectious lesions. In lytic lesions, prior studies have shown the diagnostic yield ranging from 70% to 96%;3,11,12 however, these studies have predominantly assessed the manual drill systems. One prior study13 reported the diagnostic yield and radiation dose for battery-powered drill systems, however, without comparison with manual systems. No prior studies have compared the performance of battery-powered with manual drill systems in lytic lesions. In sclerotic lesions, studies have shown that the battery-powered drill system has higher diagnostic yield but with varying differences in procedural times compared with the manual systems.5,14 In suspected discitis/osteomyelitis, a prior small-scale study (n = 41)15 showed a significantly shorter median duration of conscious sedation with battery-powered systems compared with manual systems, without significant differences in diagnostic yield.
In this study, we investigated differences in diagnostic yield, scanning time, and radiation dose between manual and battery-powered drill systems in 3 different lesion classes: lytic, sclerotic, and suspected infectious lesions.
MATERIALS AND METHODS
Study Population
This was a single-center retrospective study, which was approved by the local institutional review board, with a waiver of informed consent. From May 2010 to February 2019, a total of 1767 CT-guided bone biopsies were performed at our institution in a total of 1454 patients (difference accounting for multiple biopsy cases in 313 patients). Patients were included under the following circumstances: 1) They had pathology reports, 2) had clear documentation and/or hub visualization of the bone drill system, and 3) bone biopsy performed by the 2 fellowship-trained neuroradiologists (6 and 10 years of experience) and 2 fellowship-trained musculoskeletal radiologists (8 and 9 years of experience) chosen on the basis of the highest number of cases at our institution, to reduce operator dependence. These criteria yielded a cohort of 751 patients. Cases with only fine-needle aspiration were excluded from the study. We excluded 72 patients with lesions containing mixed lytic and sclerotic components because these lesions were qualitatively difficult to categorize and the sample size was too small for analysis after further subdivision into predominantly lytic, sclerotic, or ambiguous. Our final cohort included 585 cases with 422 lytic, 110 sclerotic, and 53 infectious lesions.
Procedure
All CT-guided spine biopsies were performed on a 40-section CT scanner (Somatom Definition AS; Siemens, Erlangen, Germany) in the helical mode. Patients all underwent a standard course for these biopsies similar to that in a prior study.16 A Fast Find Grid (Webb Medical, Philadelphia, Pennsylvania) was placed over the general biopsy site for localization. A scout was obtained using a standard biopsy protocol (initial scout at 120 kV[peak] and 60 mAs with subsequent scans at 120 kVp and 220 mAs) for all cases. Skin was prepped and draped in normal sterile fashion. One percent lidocaine was infiltrated into tissues for local and deep anesthesia. For the battery-powered system, OnControl was used with a coaxial 13-ga biopsy needle. For the manual drill system, Bonopty (AprioMed, Londonderry, New Hampshire), Osteo-site (Cook, Bloomington, Indiana), and Madison (Laurane Medical; Westbrook, Connecticut) drill systems were used with a coaxial biopsy needle ranging from 11 to 14 ga. The biopsy needle was advanced into the lesion with conventional CT guidance, and images were obtained after each needle advancement (Fig 1). CT fluoroscopy cases were not included in this study. Once the needle was confirmed within the lesion, CT scans were obtained after each biopsy pass. In each patient, 1 final postbiopsy scan was obtained after the needle was removed to assess postprocedural complications.

Bone biopsy of lytic bone lesions with manual and battery-powered drills. A, A 74-year-old man with multiple myeloma undergoing CT-guided biopsy of a right iliac lytic lesion with the Osteo-site manual system. CT image shows placement of the needle into the right iliac lytic lesion. B, A 58-year-old man with multiple myeloma undergoing CT-guided biopsy of a lytic L3 lesion with the OnControl battery-powered system. CT image shows placement of needle into the L3 vertebral body.
Data Collection
Classification of bone lesions, location, bone biopsy system, radiation dose, and scanning times were collected from our PACS reporting system. The attenuation of each sclerotic bone lesion and adjacent normal trabecular bone was obtained and averaged over 3 consecutive slices by a senior radiology resident (A.L.) with the requirement that the slices should be at least be 250 HU and twice that of the adjacent normal trabecular bone. Suspected radiologic disease, final pathology diagnosis, diagnostic yield, and the presence of crush artifacts were collected from the clinical notes and pathology reports from our Electronic Medical Records system. Diagnostic yield, the presence of crush artifacts, radiation dose, and scanning time were collected independently and blinded to the drill system used. Diagnostic yield was defined as the number of diagnostic biopsies divided by the total number of biopsies. A biopsy was considered diagnostic when a distinct pathologic diagnosis could be rendered from the surgical pathology, which explained the lesion clinically and through imaging, as defined in multiple past studies.3,5,16,17 Surgical pathology was the only source of diagnostic yield for infection, and microbiology results were not used in this study. CT scanning time and radiation dose were assessed from the radiology images, radiology reports, and clinical notes. Scanning time was defined as the interval CT imaging time from the first scout image to the final postbiopsy scan.
Statistical Analysis
The SPSS statistical package for Windows, Version 25 (IBM, Armonk, New York) was used for statistical computations. A 1-sided Fisher exact test was performed for comparison of diagnostic yields among drill systems in lytic and sclerotic lesions and suspected discitis/osteomyelitis. These were further subgrouped in a layered analysis to assess whether there was a statistically significant difference in drill performance affected by sex, lesion location, and suspected origin of the primary disease. Subgroup analysis of the drill systems for radiation dose and procedural time was made by 1-way ANOVA. A separate analysis was performed for sclerotic lesions to assess the effect of density on diagnostic yield using 1-way ANOVA.
RESULTS
Clinical Characteristics of the Patient Population
Our patient cohorts consisted of 585 cases with 422 lytic, 110 sclerotic, and 53 suspected infectious lesions. There were 314 patients in total with manual drill systems and 271 patients in total with the powered drill system (Table 1). The mean age was 62 ± 13 years with a median of 61 years with a male/female ratio of 305:280 for all lesions. Approximately 47.0% (275/585) of the lesions were located in the vertebral column; 36.9% (216/585), in the pelvic bones; and 8.4% (49/585), in the long bones such as the humerus, femur, and tibia. At the biopsy, 41.7% of bone lesions were suspected of being primary bone lesions. This predominantly included multiple myeloma based on previous laboratory work-up. Additional suspected origins of metastasis included breast (10.4%), prostate (3.8%), lung (2.9%), and bladder (1.7%). Furthermore, 27% of lesions had no definite site or suspicion of malignancy at the time of biopsy. Subgroup analysis revealed no statistical difference (P < .05) among patients between the drill systems when comparing age, sex, suspected origin of primary disease, and lesion location (Table 1).
Demographic characteristics of patients undergoing bone biopsiesa
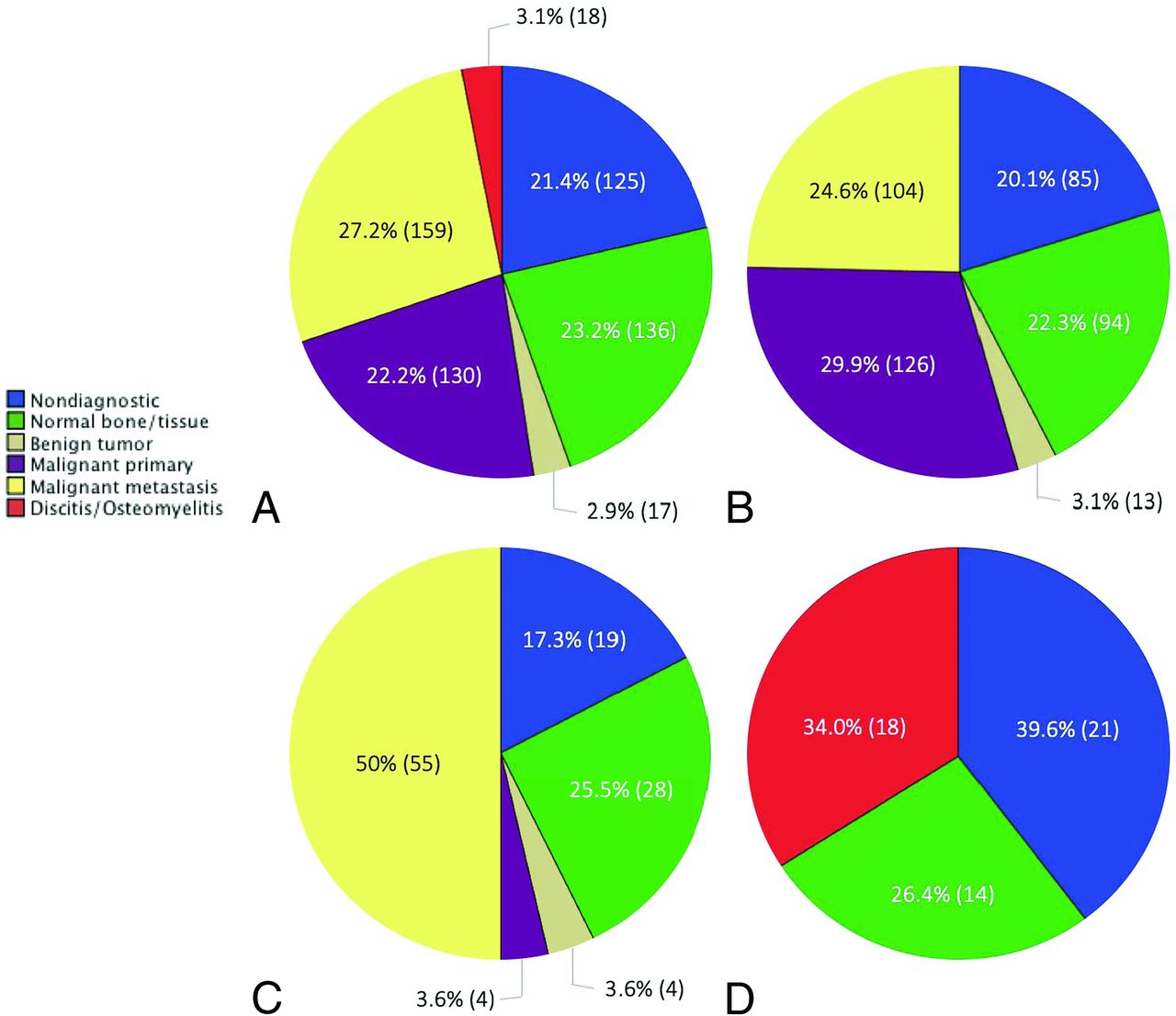
The final pathologic diagnosis revealed 27.2% of cases with metastasis and 22.2% of cases with primary bone malignancy (Fig 2).

Breakdown of the final pathology diagnosis in various bone lesion classes: all bone lesions (A), lytic lesions (B), sclerotic lesions (C), and suspected infectious lesions (D).
Comparison of Drill Systems in Lytic Lesions
A total of 422 lytic lesions included 241 cases with manual drills and 181 cases with the battery-power drill systems. No statistical difference was noted among the suspected origins of primary disease or lesion location (P = .063 and P = .316, respectively) (On-line Table 1). Diagnostic yields of the manual and powered drill systems were 83.4% and 89.0%, respectively (Table 2). Crush artifacts were present in 5% and 7.7% of manual and battery-powered drills, respectively. No statistically significant difference in diagnostic yield or crush artifacts was noted between the drill systems. However, radiation dose and scanning time were significantly lower for the battery-powered drill compared with the manual drill (P = .001 for both). The mean radiation doses for the manual and powered drills were 845 mGy × cm2 and 657 mGy × cm2, respectively. The mean scanning time for manual and powered drills was 42 and 35 minutes, respectively.
Comparative performance of the drill systems in various lesion classificationsa
Comparison of Drill Systems in Sclerotic Lesions
A total of 110 patients had sclerotic lesions, with 55 undergoing manual drill biopsies and 55 undergoing battery-powered drill biopsies. No statistical difference was noted among the suspected origins of primary disease or lesion location (P = .691 and P = .355) (On-line Table 2). The diagnostic yields of the manual and powered drill systems were 76.4% and 89.1%, respectively, and crush artifacts were present in 7.3% for both systems (Table 2). No statistically significant difference was noted among diagnostic yields or crush artifacts between the drill systems. Radiation dose and scanning time were significantly lower for the battery-powered drill compared with the manual drill (P = .028 and P = .012, respectively). The mean radiation doses were 1061 mGy × cm2 and 804 mGy × cm2, respectively. The mean scanning times for manual and powered drills were 44 and 37 minutes, respectively.
The mean density of sclerotic lesions was 663 HU, with a median density of 649 HU, ranging from 251 to 1412 HU (On-line Table 2). Average densities of sclerotic lesions in the manual and battery-powered system cohorts were 641 HU and 682 HU, respectively, without a statistically significant difference. In a subgroup analysis of biopsies, in manual drill systems, there was no significant difference found in performance based on density in sclerotic lesions. However, in the battery-powered drill system, there was a significantly longer average scanning time for sclerotic lesions of >700 HU compared with sclerotic lesions below 700 HU (P = .026), with a scanning time of 41 minutes compared with 35 minutes, respectively (Table 3). Additionally, there were higher crush artifacts with sclerotic lesions of >700 HU compared with lower density sclerotic lesions (P = .025), with crush artifacts present in 20% (4/20) and 0% (0/28), respectively. No statistically significant difference was noted for diagnostic yield or radiation dose based on density in the battery-powered drill system.
Comparative performance of drill systems in sclerotic lesions based on densitya
Comparison of Drill Systems in Suspected Infectious Lesions
A total of 53 patients had suspected discitis/osteomyelitis, with 18 manual drill biopsies and 35 battery-powered drill biopsies. No statistical difference was noted among the lesion locations. Diagnostic yields of the manual and powered drill systems were 50.0% and 51.4%, respectively, and crush artifacts were present in 11.1% and 0%, respectively (Table 2). No statistically significant differences were noted for diagnostic yield, crush artifacts, scanning time, or radiation dose between the drill systems. On the final pathology report, 34.0% were found to have the diagnosis of discitis/osteomyelitis (Fig 2).
DISCUSSION
In our study, we compared the differences in efficacy between manual and battery-powered drill systems in various lesion classes by assessing the diagnostic yield, radiation dose, and scanning time. To our knowledge, this is the first combined, large-scale study assessing comparative performances of drill systems in various bone lesion classes. In our study, we showed that there was a significant decrease in radiation dose and scanning time when using a battery-powered drill compared with a manual system in lytic and sclerotic bone lesions. Most interesting, there were no statistically significant differences in diagnostic yield or crush artifacts in any class of bone lesion, though the diagnostic yield was generally higher with the use of a battery-powered drill system.
Although there are few prior data on the comparative efficacy of these drill systems in lytic and suspected infectious lesions, Cohen et al5 reported a significantly higher diagnostic yield for battery-powered systems compared with manual drill systems in sclerotic lesions (P = .047), with diagnostic yields of 73% and 55.9%, respectively. In our study, although diagnostic yield was generally higher for the battery-powered drill system compared with manual systems, with diagnostic yields of 89.1% and 76.4, respectively, the difference was not statistically significant. Of note, the diagnostic yield reported in our study for manual systems is in keeping with most prior studies reporting approximately 75%.18,19
The diagnostic yield of a bone biopsy has been shown, in the past, to be inversely associated with the density of a bone lesion.18,20,21 This finding is explained by increased trabecular bone density associated with increased bone tissue stiffness and lowered diagnostic yield.22 It was observed in our study because the diagnostic yield was higher for lytic lesions compared with sclerotic lesions, regardless of the bone biopsy system used. In sclerotic lesions, we further observed that there was a decrease in diagnostic yield, with higher density lesions of >700 HU. We used the density cutoff of 700 HU in keeping with Chang et al23 reporting difficulty with biopsies of densely sclerotic lesions of >700 HU and Chang et al14 demonstrating differences in diagnostic yield at this threshold. Although there was no statistically significant difference in diagnostic yield at this threshold in our study, most interesting, for the battery-powered drill system, there was significantly shorter scanning time and a lower prevalence of crush artifacts for lower density sclerotic lesions. Anecdotally, this outcome is likely due to the increased difficulty in drilling into denser lesions; furthermore, increased crush artifacts have been shown to be associated with biopsies of higher density lesions in the past.3,5
A multitude of factors can affect the diagnostic yield independent of operator control. These include the histologic architecture of the bone lesion, nonspecific pathology of the biopsy specimen, and the presence of necrosis or crush artifacts, which can render the sample nondiagnostic. In our study, we show that the choice of a bone biopsy system does not significantly impact diagnostic yield, regardless of the bone lesion classification; however, it can impact the radiation dose and overall scanning time. Although many other factors dictate the choice of a bone biopsy system not assessed in this study, such as operator preference, availability, and cost, understanding the difference in efficacy is clinically significant and beneficial to patient care.
Of note, prior studies have shown that location1,24 and primary origin of disease20,25 of the bone lesions can affect the diagnostic yield. For example, Hau et al1 reported a lower diagnostic yield for vertebral lesions compared with lesions in the pelvis or extremity. Tsukushi et al25 showed that there was a higher diagnostic yield for metastatic bone lesions compared with primary bone tumors. In our study, these factors did not significantly impact the comparative performance between the bone biopsy systems because there were no significant differences in the distribution of lesion location or primary origin of disease between the cohorts.
There are several limitations to our study. First, it was retrospective. A prospective study would facilitate obtaining an equivalent number of cases for each drill system. Furthermore, because the patients were not randomized by drill systems, an inherent bias in drill system selection by the operator cannot be excluded. Additionally, although this study took place at a single institution, the study spanned 9 years, and with technologic advancements and software upgrades, there was likely a progressive decrease in scanning time and radiation dose. This factor would likely result in overestimating the actual reduction in scanning time and radiation dose for the battery-powered drill system, which was introduced 2 years after the start of the study at our institution and was used increasingly more frequently in recent years compared with the manual system. However, neither scanner nor scanning parameters were changed during the study.
Additionally, we acknowledge that there can be operator variability in drill performances. We attempted to reduce this by limiting the study to cases performed by only 2 neuroradiologists and 2 musculoskeletal radiologists. Limiting the operator number also ensured that the drill was used in most cases, though not in every case, which is a considerable limitation. Another limitation is the incongruency between scanning time and procedural time. Although scanning time was used as a surrogate for procedural time in this study, we acknowledge that there is likely a delay in the start of the procedure after the initial scan and between the end of procedure and the postbiopsy scan. Finally, only 1 attending radiologist and pathologist determined lesion classification and pathology diagnosis, respectively. We acknowledge that having multiple readers would improve the accuracy and reliability of this study.
CONCLUSIONS
We demonstrated that there was no statistically significant difference in diagnostic yield when comparing battery-powered with manual bone biopsy systems for CT-guided bone biopsies. However, the use of the power drill system resulted in a significantly reduced radiation dose and scanning time in lytic and sclerotic lesions, without significant differences in suspected infectious lesions.
Footnotes
Paper previously presented as Oral Presentation No. 19005412 at: Annual Meeting of the Radiological Society of North America, December 1–6, 2019; Chicago, Illinois.
References
- Received October 23, 2019.
- Accepted after revision January 11, 2020.
- © 2020 by American Journal of Neuroradiology









{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.