
Abstract
BACKGROUND AND PURPOSE: Traumatic brain injury (TBI) is a classic model of monophasic neuronal and axonal injury, in which tissue damage mainly occurs at the moment of trauma. There is some evidence of delayed progression of the neuronal and axonal loss. Our purpose was to test the hypothesis that quantitative MR imaging techniques can estimate the biologic changes secondary to delayed neuronal and axonal loss after TBI.
MATERIALS AND METHODS: Nine patients (age, 11–28 years; 5 male) who sustained a moderate or severe TBI were evaluated at a mean of 3.1 years after trauma. We applied the following techniques: bicaudate (BCR) and bifrontal (BFR) ventricle-to-brain ratios; T2 relaxometry; magnetization transfer ratio (MTR); apparent diffusion coefficient (ADC); and proton spectroscopy, by using an N-acetylaspartate/creatine (NAA/Cr) ratio measured in normal-appearing white matter (NAWM) and the corpus callosum (CC). The results were compared with those of a control group.
RESULTS: BCR and BFR mean values were significantly increased (P ≤ .05) in patients due to secondary subcortical atrophy; increased T2 relaxation time was observed in the NAWM and CC, reflecting an increase in water concentration secondary to axonal loss. Increased ADC mean values and reduced MTR mean values were found in the NAWM and CC, showing damage in the myelinated axonal fibers; and decreased NAA/Cr ratio mean values were found in the CC, indicating axonal loss.
CONCLUSIONS: These quantitative MR imaging techniques could noninvasively demonstrate the neuronal and axonal damage in the NAWM and CC of human brains, secondary to moderate or severe TBI.
Traumatic brain injury (TBI) is among the most frequent causes of neurologic morbidity and mortality, mainly in young adults. In the United States, the annual incidence of closed TBI is estimated at 130–150 per 100,000 people per year.1 TBI is classically a model of a monophasic neuronal lesion, in which brain tissue damage, including neuronal and glial cells injury, results from transfer of kinetic energy to the brain. Neuronal and axonal damage may result from a direct lesion at the moment of impact, often found in gray and white matter (WM) at the site of impact and on the contralateral side.
WM tracts can have diffuse axonal injury (DAI) as a result of traumatic shearing forces that occur when the head is rapidly accelerated or decelerated. It usually results from twisting or rotational forces. The true extent of axonal injury typically is worse than that visualized by using current imaging techniques. DAI typically occurs in the corpus callosum (CC), brain stem, and subcortical WM regions.
It is logical to believe that neuronal injury is limited to the acute and subacute phases after the traumatic event, followed by a short time of subsequent retrograde and anterograde (or wallerian) axonal degeneration. Once this process ends, stabilization of the neuronal injury would be expected. However, experimental studies have shown that delayed cerebral changes occur after TBI, particularly demonstrated by progression of cerebral atrophy, proposing a delayed progressive neuronal loss.2,3
Delayed neuronal loss after TBI is similar to other neurodegenerative processes. Previous studies have suggested that there is an association of TBI and an increasing incidence of delayed neurodegenerative diseases (particularly Alzheimer disease) in this group of patients.4,5 It thus becomes clear that evaluation and quantification of this delayed neuronal loss after TBI could play an important part of the clinical survey.
Recently, MR imaging has been considered as a promising noninvasive technique to evaluate axonal and neuronal injury, by using special sequences with quantitative analysis, such as volumetric measurement, ventricle-to-brain ratio, relaxometry, proton MR spectroscopy (1H-MR spectroscopy), magnetization transfer, and diffusion-weighted imaging (DWI).
The purpose of this study was to test the hypothesis that these noninvasive MR imaging quantitative techniques can identify and estimate the following biologic changes involved with neuronal and axonal loss after moderate and severe TBI: cerebral atrophy, assessed with bicaudate (BCR) and bifrontal (BFR) ventricle-to-brain ratios; extracellular-space enlargement and gliosis, assessed with apparent diffusion coefficient (ADC) and T2 relaxometry; damage to the cytoskeleton of axonal fibers and demyelination, assessed with ADC and magnetization transfer ratio (MTR); and N-acetylaspartate (NAA) reduction, assessed with 1H-MR spectroscopy.
Materials and Methods
Approval for this study was obtained from the Institutional Research Ethics Committee at Medical College of Ribeirão Preto, University of São Paulo, and written informed consent was obtained from all subjects.
Nine subjects (5 male; age, 21.1 ± 5.0 years; range, 11–28 years) with a history of moderate or severe TBI and good recovery were evaluated after >2.5 years from the traumatic event by using MR imaging. All subjects were recruited as volunteers to participate and undergo the MR imaging examination; they were exclusively devoted to this study. The eligible subjects were interviewed by the principal investigator before inclusion. Subjects with drug addiction, alcoholism, or any comorbidity were excluded.
Severity of TBI was defined as follows: severe TBI, Glasgow Coma Scale (GCS) score of ≤8; moderate TBI, a GCS score of 9–12. The results were compared with those of a control group comprising 9 healthy volunteers with a matched age and sex distribution (5 male; age, 21.8 ± 4.8 years; range, 13–28 years). The mean interval time between TBI and MR imaging evaluation was 3.1 years (range, 2.5–4.4 years). The primary causes of TBI were accidents involving automobiles (33.3%), bicycles (11.1%), and pedestrians (22.2%); assaults (22.2%); and falls (11.1%).
GCS scores ranged from 4 to 11 immediately after hospital admission on the date of trauma. TBI was classified as moderate (GCS score of 9–12) in 6 patients (66.7%) and severe (GCS score of ≤8) in the other 3 (33.3%). CT scans at the date of the trauma showed lesions suggesting DAI in 5 patients, contusion in 3, brain swelling in 2, subdural hematoma in 1, and hydrocephalus secondary to intraventricular hemorrhage in 1.
All of the images were acquired on a 1.5T MR imaging scanner (Magneton Vision; Siemens, Erlangen, Germany). Image assessment and postprocessing were performed with a Silicon Graphics O2 Workstation (SGI, Sunnyvale, Calif). Measurement and placement of regions of interest were performed by only 1 radiologist in a nonblinded fashion.
MR Imaging Acquisition Sequences and Quantitative Postprocessing Techniques
Fluid-Attenuated Inversion Recovery.
Subjects were scanned with fluid-attenuated inversion recovery (FLAIR; TR/TE = 7700/119 ms, TI = 2200 ms, FOV = 230 mm, matrix = 112 × 256, section thickness = 5 mm) images for qualitative assessment of morphologic evaluation of the brain and for spectroscopy volume-of-interest (VOI) positioning. These images were also used to measure and calculate BFR and BCR ratios. The BFR was measured by dividing the widest distance between the outer margins of the frontal horns of the lateral ventricle by the brain diameter along the same line. BCR was measured in the same way but with the minimal distance between the caudate indentations as the numerator (Fig 1).

A, The BFR is measured by dividing the widest distance between the outer margins of the frontal horns of the lateral ventricle (small continuous line) by the brain diameter along the same line (large traced line). B, The BCR is measured by dividing the minimal distance between the caudate indentations (small continuous line) by the brain diameter along the same line (large traced line).
T2 Relaxometry
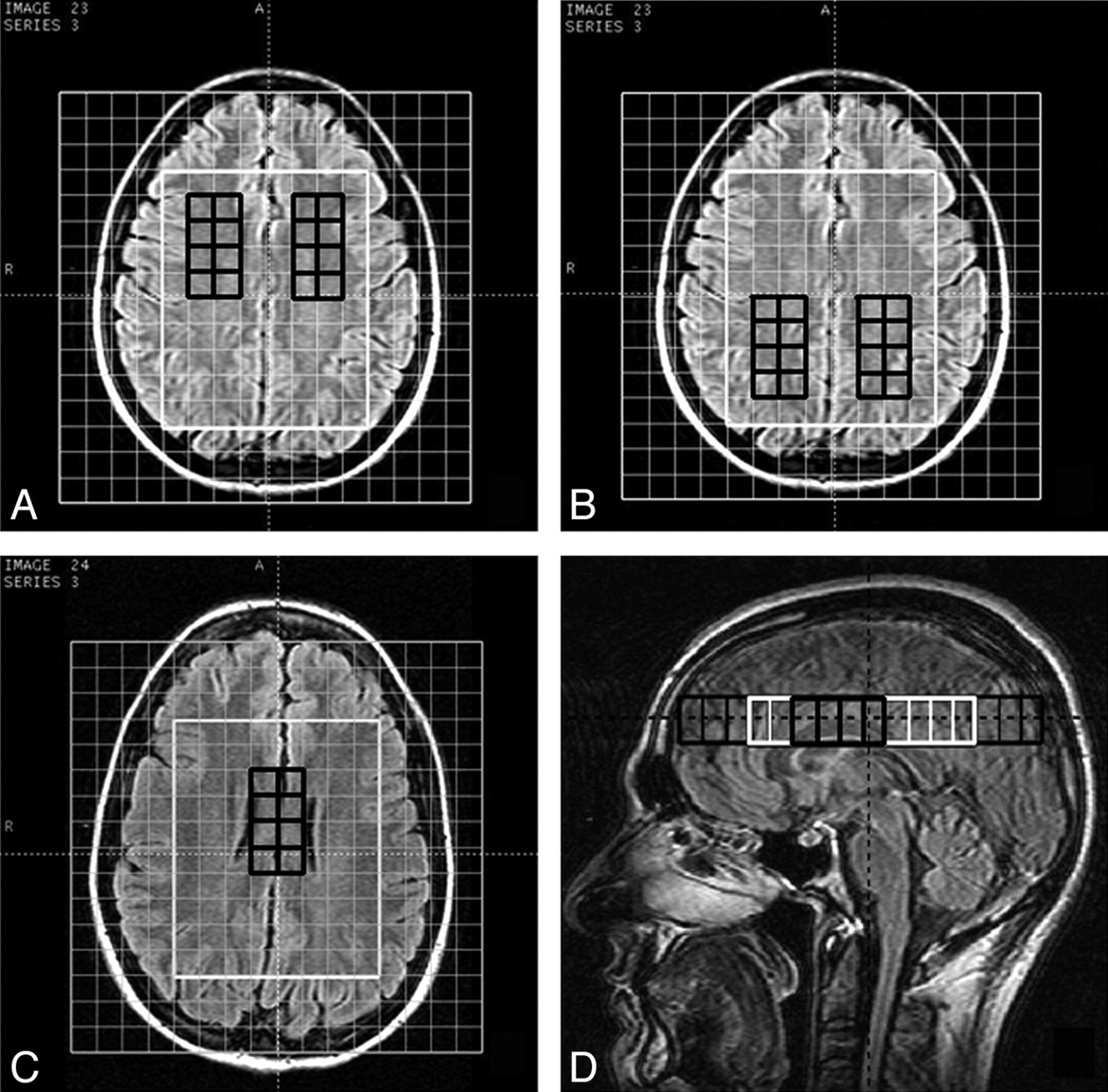
A double-echo sequence (TR = 2700 ms, TE = 17 ms and 102 ms, FOV = 240 mm, matrix = 140 × 256, section thickness = 3 mm) was performed to assess T2 relaxometry. Postprocessing and measurement of estimated T2 relaxation time were executed with software developed in our university, by using Matlab (MathWorks, Natick, Mass) already validated in previous studies. Axial sections were subdivided into 6 regions of interest for measurement: bilateral frontal and parietal normal-appearing WM (NAWM) and genu and splenium of the CC (Fig 2).

A−D, Regions of interest for measurement of T2 relaxation time, MTR, and ADC are shown in the frontal and parietal NAWM (white regions of interest in A−C) and in the genu and splenium of the CC (white regions of interest in D).
MTR
Two consecutive sets of axial T1-weighted 3D gradient-echo pulse images (TR/TE = 34/11 ms, flip angle = 30°, FOV = 256 mm, matrix = 175 × 256, section thickness = 3 mm) were acquired, the first without and the second with an off-resonance saturation pulse to assess magnetization transfer images.
MTR maps were calculated by using the following equation: [(M0 − Ms) / M0] × 100, where M0 is the image obtained by using the sequence without, and Ms is the image obtained by using the sequence with the magnetization transfer saturation pulse. The equation was applied pixel by pixel, forming an MTR map. Regions of interest were the same as those used in relaxometry (Fig 2).
DWI and ADC Maps
The isotropic DWI included an axial echo-planar spin-echo sequence (TR = 5100 ms, TE = 137 ms, FOV = 240 mm, matrix = 96 × 128, section thickness = 5 mm, 3 orthogonal planes; 4 b-values of 0, 50, 500, and 1000 s/mm2). The ADC map was calculated, and regions of interest were the same as those used in relaxometry and MTR (Fig 2).
1H-MR Spectroscopy
A multivoxel point-resolved spectroscopic sequence, with a TE of 270 ms, TR of 1500 ms, and a 16 × 16 transverse phase-encoding matrix, was performed. The VOI was positioned to include the CC and corona radiata. The VOI dimensions were as follows: thickness = 20 mm, anteroposterior dimension = 100 mm, and right-left dimension = 80 mm. The VOI was divided into 80 voxels of 20 × 10 × 10 mm (2.0 mm3). Spectroscopic data were processed with software provided by the MR imaging vendor (Siemens). NAA/creatine (NAA/Cr) ratios were calculated on both sides of the frontal and parietal WM and in the region of the CC (Fig 3).

1H-MR spectroscopy VOIs are positioned to include the CC and corona radiata. NAA/Cr ratios are calculated in the frontal (black voxels in A) and parietal (black voxels in B) WM and in the region of the CC (black voxels in C and D).
Statistical Analysis
To assess differences of BFR, BCR, T2 relaxation time, MTR, ADC, and NAA/Cr ratio parameters between study groups, we used unpaired t tests. The Statistical Package for the Social Sciences (SPSS, Chicago, Ill) was used for all tests. P values < .05 were considered to indicate a significant difference.
Results
BFR, BCR, T2 relaxation time, and ADC values of the test group were higher and MTR values were lower than those of the control group in both the NAWM and CC, and the differences were statistically significant. The NAA/Cr ratio measured at the CC was lower and statistically significant in the test group, but no significant difference was found at NAWM. These results are described and summarized in the Table.
BFR and BCR, T2-relaxation time, ADC, MTR and NAA/Cr ratio mean value differences between the test and control groups, measured at the NAWM and CC
In 1 patient, conventional MR images showed many areas of signal-intensity loss at the CC, in the subcortical WM and in the deep WM, which corresponded to hemosiderin deposition secondary to DAI. In this case, regions of interest were placed to avoid these signal-intensity-loss areas and to include only NAWM. Focal atrophy associated with gliosis was observed at the left temporal lobe in 2 patients secondary to traumatic brain contusion, and these areas were also not included in our data (Fig 4). No focal lesions were observed in the other subjects.

A and B, Conventional MR images (transversal T2-weighted turbo spin-echo [TSE] sequence in A and coronal FLAIR sequence in B) show focal atrophy and gliosis in the left temporal lobe (white arrow) secondary to a traumatic brain contusion in a 24-year-old female patient. C and D, MR images (transversal T2-weighted TSE sequence in C and saggital FLAIR sequence in D) demonstrate many areas of signal-intensity loss at the CC (black arrows) and at the subcortical and at deep WM (white curved arrows in C), which correspond to hemosiderin deposition secondary to diffuse axonal injury in a 22-year-old male patient.
Discussion
Conventional MR imaging sequences are qualitative techniques that allow quick subjective interpretation for the diagnosis of various central nervous system anomalies with proved efficacy. However, some mild microstructural changes may not be discernible in these sequences. Thus, delayed neuronal and axonal damage after TBI in NAWM would only be confirmed with histologic analysis of brain tissue fragments, obviously impracticable in human beings. Some quantitative MR imaging techniques have the potential to evaluate and estimate this mild microstructural damage after TBI.
Brain atrophy secondary to neuronal damage and loss after TBI has already been reported in human and animal model research.2,3,6,7 The brain atrophy progression is faster in the first year after the traumatic event, and there is evidence that this process continues for up to 3 years, but at a slower rate. This delayed progression of the brain volume loss may be related to neuronal apoptosis unleashed by TBI.8,9 Ventricular dilation is the most frequent abnormality found after TBI and is directly related to the degree of WM loss and inversely related to cognitive outcome.8 In our study, significantly higher ventricle-to-brain ratio (BFR and BCR) mean values were also observed in the test group, compared with the controls, reflecting ventricular enlargement secondary to subcortical atrophy due to axonal damage after TBI.
T2 relaxation time directly corresponds to water concentration in tissue. The main etiologies of increased water concentration in central nervous parenchyma are inflammatory processes, edema, demyelination, gliosis, or neuronal loss.10–12 A higher mean value of T2 relaxation time was observed in the NAWM and CC of the test group in our study, compared with the control group, demonstrating higher water concentration in these regions. The cause of this increased water concentration is thought to be axonal loss (with concomitant myelin sheath loss) and gliosis, secondary to TBI. Certainly, no edema or inflammatory process was present at time of examination, because the traumatic event occurred ≥2.5 years before MR imaging evaluation and all subjects had no symptoms of acute disease or comorbidity.
In the MR imaging sequences with the magnetization transfer saturation pulse directed to protons linked to macromolecules, the signal intensity decreases proportionally to concentration of these macromolecules. This loss of signal intensity is quantifiable by calculating the MTR between saturated and nonsaturated images. Thus, when the concentration of macromolecules is reduced in an evaluated tissue, a decrease in MTR value is expected. The main macromolecules of the cerebral WM are proteins and sphingolipids of the axonal membranes and myelin. So, in WM lesions in which demyelination or axonal loss is present, the MTR values decrease, even before conventional MR imaging sequences reveal visible signal-intensity change in the damaged areas.13–15 Reduction of MTR values measured in WM after TBI was already demonstrated13,16 and also at the CC in victims of mild TBI.17 We also observed a significantly lower MTR mean value measured at the NAWM and CC of the test group compared with the control group, probably secondary to axonal loss and demyelination, indirectly showing the axonal microstructural damage in these regions after TBI.
The integrity of the cytoskeleton of axonal fibers and myelin sheaths is a natural restraint to water diffusibility in the brain. For this reason, DWI shows an anisotropic conformation, where water diffusion direction is predominantly parallel to axonal tracts.18 Thus, anisotropy is more evident in WM, where axonal fiber concentration is higher. For global diffusion evaluation, independent of its direction, isotropic DWI is used with ADC maps.
Appraised ADC values are inversely proportional to the restriction of water diffusibility. Axonal damage or demyelination, with disruption of the axonal cytoskeleton and myelin sheath, causes a reduction in the diffusion restriction, resulting in an increase of ADC values and decreased anisotropy.19–22 In the present study, ADC mean values measured at the NAWM and CC of the TBI victim group were higher than those measured in the test group, reflecting loss of myelinated axonal fibers secondary to trauma.
Raised ADC values at NAWM, >11 months after TBI, were already demonstrated in 2 patients studied by Rugg-Gunn et al.23 These authors concluded that the increase of ADC values would suggest an expansion of the extracellular space due to neuronal or glial loss, not discernible in the conventional MR imaging sequences.
Another way to evaluate axonal damage is by using diffusion tensor imaging parameters, such as fractional anisotropy (FA), not used in our study. Decreased FA value in the WM reflects axonal damage with loss of structural integrity of the myelinated fibers. Reduced FA values in the CC and other WM areas after mild, moderate, and severe TBI were already demonstrated in both early and late (or chronic) phases.19,23–27
NAA is a metabolite produced exclusively in neurons,28 synthesized from acetyl-CoA and L-aspartate in the mitochondria. NAA is found in high concentration in the neuronal cytosol and is second only to glutamate in terms of concentrations.29 This metabolite is also present in the axonal fibers,28 taking part in the synthesis process of myelin in developing brain and, probably, in the axonal repairing process in adults. Thus, NAA is considered a neuronal and axonal marker, and its concentration decreases in brain lesions that cause neuronal or axonal loss.
Decreased NAA after TBI was already demonstrated in the WM,30–34 CC,13,35 gray matter,30–32,36 thalamus,37 and hippocampus and basal ganglia,38 in both subacute28,30,33 and late phases.31–35,38
Our results showed a significantly decreased NAA/Cr ratio mean value in the CC of the posttraumatic patient group, reflecting axonal loss in this location due to TBI. Opposed to the results of other previous studies that reported decreased NAA in WM after TBI,30–34 no significant difference of NAA/Cr ratio values in the NAWM between the test and control groups was observed in our study. Although there was no statistically significant difference, a lower NAA/Cr ratio mean value was observed in the test group, but the small number of patients evaluated here would be inadequate to establish this difference. Thus, on the basis of our results, we could not assert that the NAA/Cr ratio could evaluate axonal damage in the NAWM, and a larger sample size would be necessary to answer this question. Kampfl et al39 evaluated patients with a persistent vegetative state after severe closed TBI and reported that the CC was the region most commonly affected in subjects with diffuse WM lesions. This could be the reason that NAA/Cr ratio mean values were statistically different in the CC but not in the NAWM in our study.
We used strict inclusion and exclusion criteria to minimize the possibility that other factors could be involved in the neuronal damage besides TBI effects, resulting in a small sample size.
Conclusions
Correlation between the results achieved in this study and the microstructural changes secondary to neuronal and axonal loss without histologic confirmation is just speculation. However, on the basis of histologic findings reported in other studies showing neuronal and axonal lesions after TBI,40–42 our results allow us to assert that these quantitative MR imaging techniques could noninvasively demonstrate delayed neuronal and axonal damage in the CC and NAWM after moderate and severe TBI.
References
- Received October 7, 2008.
- Accepted after revision December 3, 2008.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}