
Abstract
BACKGROUND AND PURPOSE: Although coiling has been favorably comparable with clipping for treatment of most intracranial aneurysms, there is a controversy on which modality is safer for anterior choroidal artery (AchoA) aneurysm. We retrospectively evaluated the clinical outcomes and treatment-related complications after surgical clipping and endovascular coiling of AchoA aneurysms.
MATERIALS AND METHODS: Seventy-three AchoA aneurysms were recruited from 1895 intracranial aneurysms, which were treated either by surgical clipping or by endovascular coiling in 4 institutions between May 1999 and December 2006. The AchoA aneurysms were dichotomized according to the modality of treatment, the coil group (37 patients; 38 aneurysms) and the clip group (35 patients; 35 aneurysms). Clinical outcomes and incidence of treatment-related complications between 2 groups and the factors influencing the clinical outcomes were evaluated.
RESULTS: There was no rebleeding in both groups during follow-up, for 4–72 months (mean, 27 months) in the coil group and for 3–84 months (mean, 34 months) in the clip group. In the coil group, 31 patients (83.8%) had favorable outcome (modified Rankin Scale score [mRS], 0–3). In the clip group, 31 patients (88.6%) had favorable outcome. The complication of coiling was transient contralateral hemiparesis in 2 patients, who recovered completely. The complications of clipping were permanent contralateral hemiparesis due to AchoA infarction in 4 patients and third-nerve palsy in 1 patient. Hunt and Hess grade 4 or 5 and AchoA infarction were significantly correlated with poor outcome (mRS, ≤4). Clipping had significantly higher incidence of AchoA infarction than coiling (P < .05).
CONCLUSION: Coiling of AchoA aneurysms appears comparable with clipping in clinical outcome and prevention of rebleeding, with significantly lower incidence of AchoA infarction than clipping.
Anterior choroidal artery (AchoA) aneurysms are relatively rare and account for 2%–5% of all intracranial aneurysms.1 Because AchoA is a small branch, but supplies critical territory, including posterior limb of the internal capsule, impairment of this artery may produce debilitating postoperative AchoA syndrome, including contralateral hemiparesis. The mortality rate and the treatment-related permanent morbidity rate of surgical clipping of AchoA aneurysms range from 6% to 33% and 10% to 28.6%, respectively.2–5 To our knowledge, there has been only 1 small series focused on coiling of the AchoA aneurysms.6 The purpose of this study was to retrospectively evaluate and compare the clinical outcomes and treatment-related complications after surgical clipping and endovascular coiling of AchoA aneurysms.
Materials and Methods
The institutional review boards of the 4 hospitals approved this retrospective study, and informed consent was not required. Seventy-three AchoA aneurysms were recruited from 1895 intracranial aneurysms, which were treated either by surgical clipping or by endovascular coiling in 4 institutions between May 1999 and December 2006. One patient had bilateral AchoA aneurysms. The aneurysms were sorted into 2 groups according to the technique of treatment, the coil group and the clip group. The coil group (n = 38; ruptured = 23; unruptured = 15) was composed of those who underwent endovascular coiling and included 14 men and 23 women with ages ranging from 23 to 78 years (mean, 54 years). The clip group (n = 35; ruptured = 30; unruptured = 5) was composed of those who underwent surgical clipping and included 15 men and 20 women with ages ranging from 25 to 63 years (mean, 45 years). Aneurysms associated with arteriovenous malformation and aneurysms involving distal AchoA were excluded. Informed consent was obtained and preceded treatment. An interventional neuroradiologist and a neurosurgeon reviewed the angiograms, operative records, and medical records to obtain the relevant clinical and angiographic information.
Coil Embolization and Surgical Clipping
Coiling was conducted under general anesthesia. Anticoagulation was initiated by injection of a bolus of 3000–5000 IU of heparin intravenously at the beginning of the procedure, followed by continuous infusion of heparin by rate of 1000 IU/h. Heparin was continued for 24–48 hours after embolization. Activated coagulation time was maintained between 2 and 3 times above the normal value. Coiling was generally performed by a standard single-microcatheter technique. Double-microcatheter technique was used in 4 aneurysms due to the wide neck and/or incorporation of the AchoA into the aneurysm (Fig 1). Stent-assisted technique was used in 2 aneurysms due to the wide neck.

Images of a 63-year-old woman who presented with subarachnoid hemorrhage. A, 3D volume-rendering image in oblique projection reveals an anterior choroidal artery aneurysm with daughter sac. The anterior choroidal artery is incorporated into the aneurysm neck. B, Unsubtracted image in working-projection obtained during the procedure. The aneurysm is treated with the double-catheter technique. Note 2 radiopaque markers of the tip of the microcatheter near the aneurysm neck. C, Postembolization control angiography in working-projection reveals near complete occlusion of the aneurysm sac.
Surgical clipping was performed with a standard technique. In most cases, microvascular Doppler ultrasonography was used to identify the flow into the AchoA. Monitoring of intraoperative motor-evoked potentials (MEPs) was not used.
Clinical and Angiographic Follow-up
The patients were clinically assessed before and after the treatment by the neurosurgeons and/or the interventional neuroradiologists. The coil group was clinically followed up for a mean ± SE of 27 ± 22 months (range, 4–72 months) and the clip group for a mean of 34 ± 25 months (range, 3–84 months).
Each patient’s outcome at the latest clinical follow-up was evaluated and graded according to the modified Rankin scale score (mRS).7 For the patients who were not followed up at our institutions, clinical outcome was evaluated with a telephone interview. If the patient’s clinical condition became worse because of causes unrelated to the procedure or the aneurysm during the follow-up, the patient’s outcome at discharge was determined as the final outcome.
In the coil group, angiographic follow-up after coiling was conducted as our routine schedule for intracranial aneurysms at the other sites. In the clip group, angiographic follow-up was not routinely performed.
Statistics
All of the statistical analyses were performed using SPSS for Windows (version 10.0; SPSS, Chicago, Ill). The factors influencing clinical outcome and treatment-related AchoA infarction were evaluated. Univariable analyses for age, sex, aneurysm size, neck type, presence of subarachnoid hemorrhage (SAH), Hunt and Hess grade, treatment modality, and treatment-related AchoA infarction were separately performed modeling poor outcome (mRS, ≥4) using a χ2 test. All of the variables with P < .2 in univariable analysis were entered into separate multivariable logistic regression models. Incidence of treatment-related complications was compared between the coil group and the clip group by using a χ2 test. Statistical significance was determined by P < .05 for a 95% confidence interval.
Results
Characteristics of the Patients and AchoA Aneurysms: Coil Group Versus Clip Group
The coil group was significantly older in age than the clip group. There were no significant differences between the 2 groups in sex, size of aneurysms, diameter of aneurysm neck, incidence of rupture, and Hunt and Hess grade (Table 1).
Characteristics of the enrolled patients and anterior choroidal artery aneurysms
Clinical Outcome
Clinical outcomes (mRS) are summarized in Table 2 according to the Hunt and Hess grading (HH) system and the treatment modality. None of the 72 patients treated either by coiling or by clipping rebled during follow-up. Of the patients with HH 0–3, all (n = 30) of those in the coil group had favorable outcome, whereas 2 patients in the clip group (n = 32) had poor outcome (mRS, ≥4) due to treatment-related AchoA infarction to result in grade 2 contralateral hemiparesis.
Clinical outcome in relation to Hunt and Hess grade on admission
HH 4 or 5 and treatment-related AchoA infarction were significantly correlated with poor outcome (P < .05). Age, sex, aneurysm size, neck type, presence of SAH, and the type of treatment modality were not significantly correlated with clinical outcome (Tables 3 and 4).
Univariable analyses modeling poor outcome
Multivariable logistic regression analysis modeling poor outcome (modified Rankin scale score ≤4)
Treatment-Related Complications
In the coil group, transient AchoA flow insufficiency occurred in 5 patients during the procedure. However, the patency of the AchoA was restored within 30 minutes in all 5 of the patients by using intravenous bolus injection of 5000 IU of heparin (n = 1), infusion of 5–10 mg of abciximab through the guiding catheter (n = 2), or papaverine infusion through the microcatheter (n = 2). In 2 of the 5 patients, transient contralateral hemiparesis occurred after the procedure but resolved within 1 week. Follow-up CT of the 2 patients revealed no evidence of AchoA infarction. The other 3 patients had no postprocedural adverse symptoms. In addition, there were no access related complications.
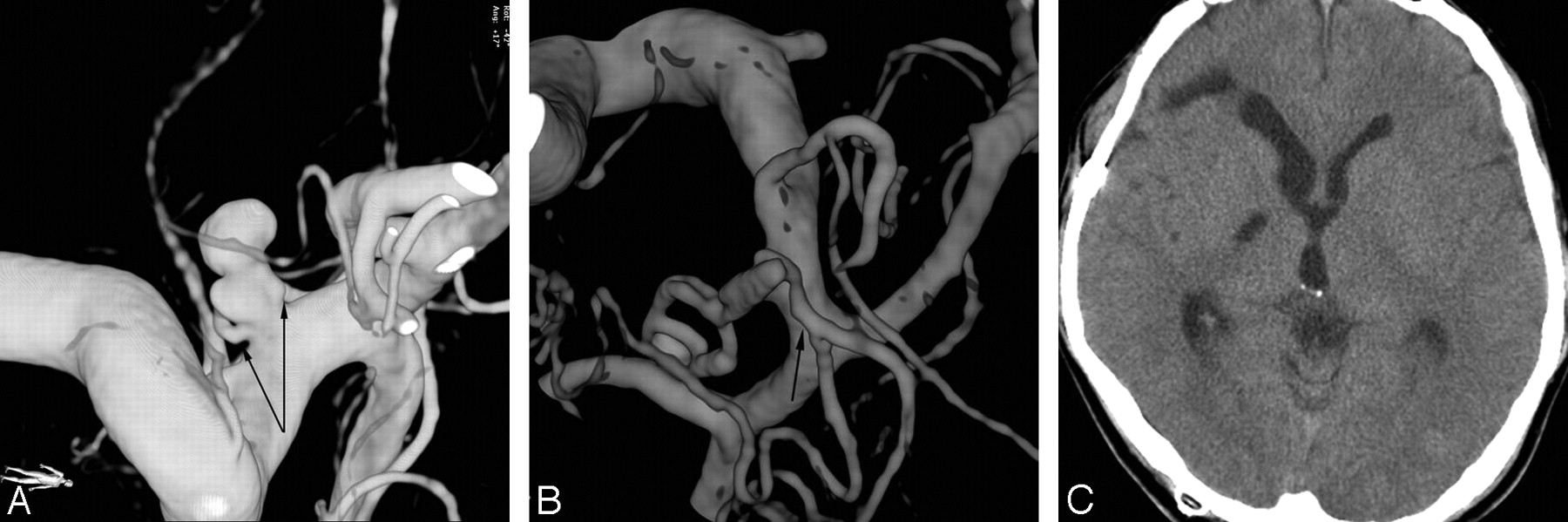
In the clip group, permanent contralateral hemiparesis due to the AchoA infarction occurred in 4 patients, and third-nerve palsy occurred in 1 patient (Table 5). All 4 of the patients with permanent contralateral hemiparesis revealed infarction in the posterior limb of ipsilateral internal capsule on CT (Fig 2). Clipping had significantly higher incidence of treatment-related AchoA infarction than coiling (Table 5).

Images of a 46-year-old man who presented with subarachnoid hemorrhage. A, 3D volume-rendering image reveals anterior choroidal artery aneurysm with the daughter sac. B, The anterior choroidal artery is well preserved on follow-up angiography performed due to the postoperative contralateral hemiparesis. C, Follow-up CT reveals low attenuation in the ipsilateral anterior choroidal artery territory, posterior limb of right internal capsule.
Treatment-related complications
Results of Follow-up Angiography
Twenty-nine aneurysms (76.3%) in 28 patients of the coil group were followed up with 1 or more angiographies. Recurrence was found in 5 (17.2%) of the 29 aneurysms in angiographic follow-up performed 6-45 months (mean ± SE, 18 ± 12) after treatment. Four recurrences were found in the first year of follow-up, and 1 in the second year. Of the 5 recurred aneurysms, a second coil embolization was performed with results of near-complete occlusion in 2 aneurysms, both of which were stable on the next 2 follow-up angiographies. The other 3 aneurysms were not retreated because of the small size of the recurrent sac.
Three patients of the clip group underwent immediate follow-up angiography on the following day after surgery due to symptoms of AchoA infarction. One patient revealed AchoA occlusion, and 2 patients revealed patent AchoA (Fig 2). No patient in the clip group underwent late follow-up angiography.
Discussion
The perforating branches of AchoA passing through the anterior perforating substance to the globus pallidus and posterior limb of the internal capsule do not receive any significant collateral supply.8 Impairment of the AchoA during treatment may result in serious clinical consequences, called the AchoA syndrome, which consists of contralateral hemiparesis, hemisensory loss, and homonymous hemianopsia. Therefore, although coiling has been favorably comparable with clipping for the treatment of most of intracranial aneurysms,9 there is a controversy on which technique is safer for the treatment of AchoA aneurysms. The surgical literature distinguishes the AchoA aneurysms from other intracranial aneurysms.2–5 Friedman et al5 reported, to our knowledge, the largest surgical series in the surgical literature. They treated 51 AchoA aneurysms in 50 patients, among whom 33 patients presented with SAH. Three (6%) of the 50 patients died, among whom 2 (4%) died from treatment-related complications. Eight (16%) of the 50 patients had postoperative clinical and CT evidence of an AchoA infarction. Of the 8 patients with AchoA infarctions, 1 patient died, and 5 patients had major neurologic deficits.
Recently, a series of 18 AchoA aneurysms treated by endovascular technique in 18 patients was reported, of which 14 patients (77.8%) presented with SAH, and 13 AchoA aneurysms (72.2%) were the source of SAH. One patient (5.5%) died due to aneurysm perforation during the procedure. Another patient (5.5%) had a transient contralateral hemiparesis.6
In our study, clinical outcome of coiling for AchoA aneurysms was comparable with clipping. However, the incidence of treatment-related AchoA infarction was significantly lower in the coil group than in the clip group. Moreover, treatment-related AchoA infarction was also significantly correlated with poor outcome. One of the advantages of coiling for the AchoA aneurysm is that we can make certain of the patency of the AchoA during the entire procedure. During surgery, it is often difficult to verify the patency of the AchoA by microscopy because of the small size of the artery and site of origin, usually behind the internal carotid artery, as viewed surgically. Although the surgeons were confident of their patency at completion of the operation, the AchoA was occluded in 2 (28.6%) of the 7 aneurysms4 and in 6 (11.8%) of the 51 aneurysms.5 Shibata et al10 reported that the use of intraoperative microvascular Doppler sonography (MDS) decreased the incidence of postoperative AchoA syndrome from 16% to 5%. More recently, Suzuki et al11 reported that intraoperative monitoring of MEPs in 108 patients with ICA aneurysms was reliable for detecting insufficiency of AchoA perfusion intraoperatively. In our study, intraoperative monitoring of MEPs was not routinely used, but intraoperative MDS was used. Intraoperative insufficiency of perfusion to the AchoA was suspected in only 1 patient, but ipsilateral infarctions in the posterior internal capsule were detected on follow-up CT in all 4 of the patents with resultant contralateral hemiparesis. Moreover, of the 3 patients who underwent follow-up angiography within 24 hours after completion of clipping, only 1 patient revealed AchoA occlusion, whereas the other 2 patients revealed patent AchoA. These suggest that postoperative AchoA infarction may result from transient insufficiency, as well as permanent occlusion. The possible mechanisms of transient or permanent insufficiency during or immediately after surgery include clipping of the parent artery, thromboembolism during manipulation of the AchoA, vasospasm, glial edema, clip torsion due to postoperative edema of neighboring structures, or a combination of those.5,6 AchoA is usually small, and its perforating branches had poor collateral supply.8 Therefore, transient insufficiency of flow for more than a certain period of time may lead to critical ischemia of the AchoA territory. Endovascular treatment has the advantage that it is possible to promptly detect insufficiency of flow in the AchoA during the procedure. In our study, prompt detection of transient AchoA flow insufficiency during endovascular treatment made it possible to restore its flow by immediate management. As a result, of the 5 patients who had transient AchoA insufficiency, none had permanent neurologic deficit.
Because follow-up angiography was seldom performed in the clip group, comparing the recurrence rates of the AchoA aneurysms between the clip group and the coil group will be difficult. However, it is probable that recurrences are more frequent after coiling than after clipping,12–14 and follow-up angiographies were more frequently performed for the coil group in this study. Therefore, it may be required to routinely follow-up with angiography after coiling the AchoA aneurysm. In addition, because there is a small but significant risk of de novo aneurysm formation or growth of remnant aneurysm after clipping, clinical follow-up should be applied to both the coil group and the clip group over an extended period of time.14,15
The results of this study suggest that coiling for AchoA aneurysms is comparable with clipping in clinical outcome and prevention of rebleeding, with significantly lower incidence of AchoA infarction, which will potentially result in poor outcome.
References
- Received June 21, 2007.
- Accepted after revision July 12, 2007.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}