
Abstract
SUMMARY: A 69-year-old woman had a symptomatic cervical carotid stenosis coupled with a coincidental unruptured cerebral aneurysm in the carotid distal segment. She underwent endovascular coiling for the aneurysm and then carotid stent placement (CAS) 1 month later. Both lesions were treated successfully and neither complications nor strokes occurred after the procedures. Staged endovascular treatment of coiling and subsequent CAS may be safe for patients with a cervical carotid stenosis coupled with cerebral aneurysms.
Patients with a symptomatic cervical carotid bifurcation stenosis coupled with a coexisting cerebral aneurysm in the carotid distal segment present a therapeutic dilemma.1 Relief of the carotid stenosis, leading to a sudden rise in perfusion pressure, might increase the potential risk of aneurysm rupture.1-4 Conversely, repair of aneurysms with the patients under general anesthesia may increase the risk of strokes because of decreased cerebral blood flow (CBF) imposed by the carotid stenosis.1,2 Although endovascular therapy may be essential for patients with a symptomatic carotid stenosis coupled with an unruptured cerebral aneurysm in the distal segment, a therapeutic strategy has not yet been established. If a carotid stenosis is dilated by stent placement first, a sudden rise in perfusion pressure and subsequently required high-dose antiplatelets may increase the risk of aneurysm rupture. Even though aneurysm coiling first is a rational approach, there are technical problems concerning how to embolize aneurysms through the cervical carotid bifurcation stenosis.
We hereby report a case of successful staged endovascular treatment of aneurysm coiling and subsequent carotid stent placement (CAS).
Case Report
A 69-year-old woman experienced a transient episode manifesting as a right-sided hemiparesis. She had a history of hypertension and diabetes mellitus for at least 10 years, which had been under fair control with multiple medications. She also had unstable angina and was treated by percutaneous coronary intervention. Her father died of subarachnoid hemorrhage. Findings of a neurologic examination on admission were normal. MR imaging showed a mild ischemic change in the territory of the left middle cerebral artery, and MR angiography showed a high-grade stenosis of the left internal carotid artery (ICA) and an incidental intracranial aneurysm of the ipsilateral ICA. Left carotid angiography revealed an 80% stenosis of the left ICA (Fig 1A) and a coincidental unruptured intracranial aneurysm (6 × 4 mm) in the distal segment (Fig 1B).

Left common carotid angiography (anteroposterior projection) shows a high-grade carotid bifurcation stenosis (A) and a coincidental unruptured intracranial aneurysm (6 × 4 mm) (B).
With the patient's fully informed consent, staged endovascular procedures were attempted. On June 27, 2007, coiling of the aneurysm was performed first under local anesthesia. A guiding catheter (6F Shuttle-SL guide sheath with 0.087 internal diameter; Cook, Bloomington, Ind) was positioned in the left common carotid artery proximal to the left carotid bifurcation stenosis. For the stability of the guide catheter during the procedures, a guidewire (0.014 inch, 300 cm in length, Right Away Super Hard; Piolax, Kanagawa, Japan) was inserted into the external carotid artery (ECA) (Fig 2A). Then, a microcatheter (Excelsior SL-10; Boston Scientific, Fremont, Calif) was placed through the carotid bifurcation stenosis, and there was still adequate flow into the ipsilateral cerebral hemisphere. No ischemic symptoms occurred after insertion of the microcatheter into the carotid bifurcation stenosis and during the procedures. The microcatheter was navigated into the cerebral aneurysm through the carotid bifurcation stenosis, and aneurysm coiling was performed with Guglielmi detachable coils (Boston Scientific) and Trufill coils (Cordis, Miami Lakes, Fla) and was accomplished successfully. She received 2 antiplatelet agents (aspirin, 100 mg/day, and clopidogrel, 75 mg/day) orally 2 days before and continuing after the procedure.
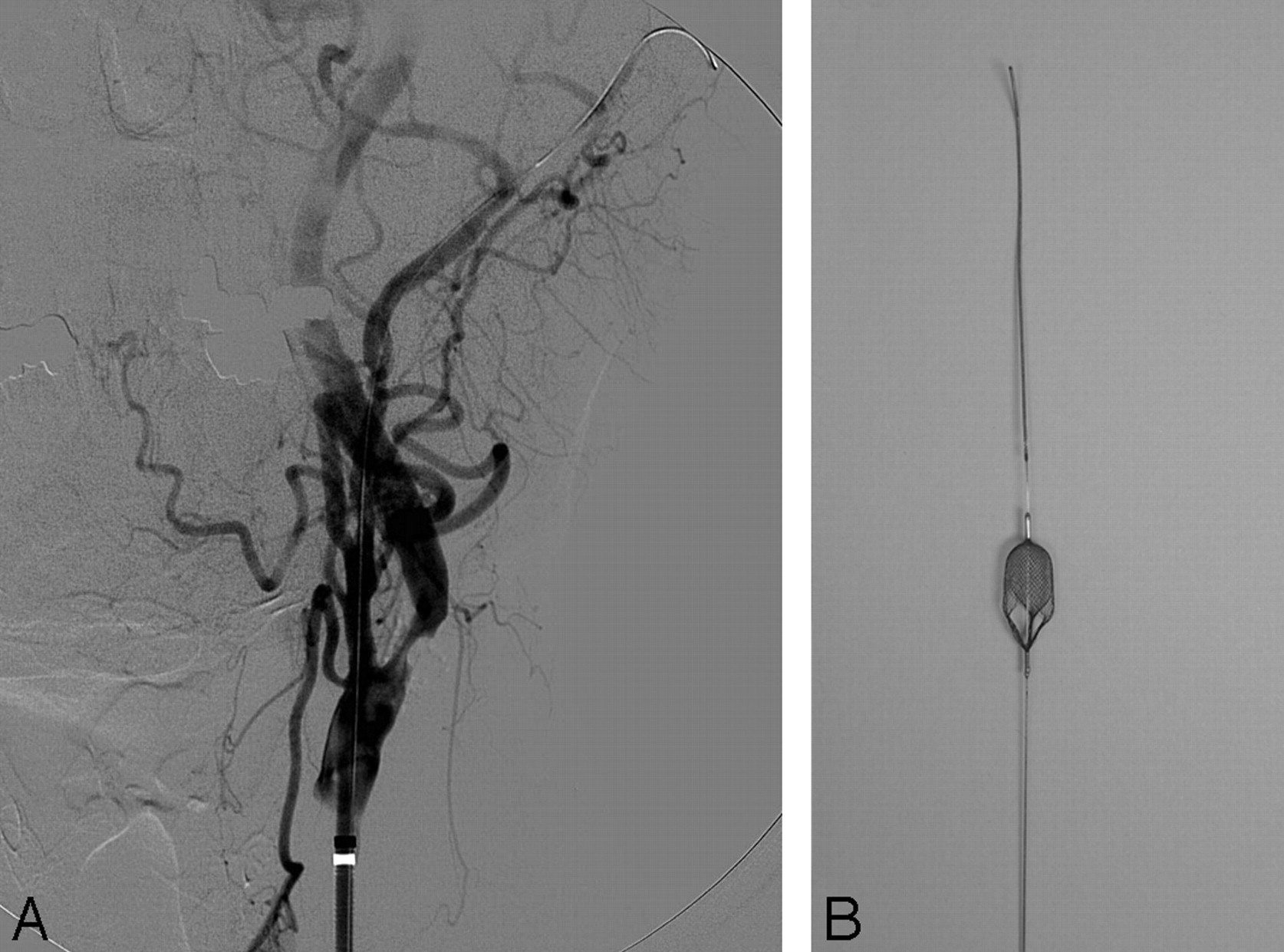
A, Left common carotid angiography (anteroposterior projection) after positioning the guide-catheter (6F Shuttle-SL guide sheath) demonstrates the support-wire (0.014-inch Right Away Super Hard) inserting into the left ECA and a high-grade carotid bifurcation stenosis. B, MintCatch filter-type catheter with a 5-mm diameter.
On July 25, 2007, CAS was performed. A guiding catheter (6F, Shuttle-SL guide sheath) was positioned in the left common carotid artery. A filter-type catheter (5-mm in diameter and 300 cm in length, MintCatch; IR Medical Koubou, Koriyama, Fukushima, Japan) (Fig 2B) was navigated through the carotid bifurcation stenosis and positioned in the distal ICA as a distal protection device. A low-profile 4.0-mm-diameter balloon catheter (Gateway; Boston Scientific) was advanced to the carotid stenosis over the filter wire and dilated up to 6 atm. The balloon catheter was replaced by a self-expandable stent (8 × 40 mm Precise; Cordis), which was deployed over the residual stenosis. No complications occurred during and after the procedures. Neither transient ischaemic attacks nor strokes occurred during the follow-up. On October 30, 2007, left carotid angiography showed complete obliteration of the aneurysm and sufficient dilation of the carotid artery after CAS (Fig 3A, -B).

Left common carotid angiography 3 months after CAS (anteroposterior projection) shows complete obliteration of the embolized aneurysm (A) and no restenosis of the carotid bifurcation (B).
Discussion
Cerebral aneurysms are incidentally found at autopsy in approximately 5% of adults.5 As for the treatment of unruptured cerebral aneurysms, neurosurgical clipping has been indicated for patients with a life expectancy of more than 5 years, younger than 70 years of age, and harboring an aneurysm of ≥5 mm.6-9 It is reported10 that endovascular coiling can allow more patients with ruptured intracranial aneurysms to become independent at 1 year than neurosurgical clipping. van Rooij et al11 also reported that coiling should be the first treatment option in incidental aneurysms. Results of cooperative studies have clearly demonstrated the benefit of surgery for patients with severe symptomatic carotid stenosis.12,13 Among patients with severe carotid artery stenosis and coexisting high-risk conditions, CAS with the use of an emboli-protection device is not inferior to carotid endarterectomy (CEA).14,15
Cerebral unruptured aneurysms ipsilateral to a carotid lesion producing symptoms are often found incidentally in the most common situation. Of the 2885 patients participating in the North American Symptomatic Carotid Endarterectomy Trial (NASCET), 51 (1.7%) had ipsilateral unruptured intracranial aneurysms.2 Patients with a symptomatic cervical carotid bifurcation stenosis coupled with a coexisting cerebral aneurysm in the carotid distal segment present a therapeutic dilemma.1 Relief of the carotid stenosis, leading to a sudden rise in perfusion pressure, might increase the potential risk of aneurysm rupture.1-4 Conversely, repair of the aneurysm with the patient under general anesthesia may increase the risk of strokes because of decreased CBF imposed by the carotid stenosis.1,2
By analyzing the results of NASCET,13 a previous study reported2 that 25 patients with ipsilateral unruptured aneurysms underwent CEA on the side of their symptomatic artery without having them repaired and that subarachnoid hemorrhage occurred in 1 (4%) of the 25 patients 6 days after CEA. The patient died 4 days after subarachnoid hemorrhage. This result suggests that a 4% aneurysm-rupture rate is high, and repair of unruptured aneurysms before CEA is a rational approach. In patients with a severe carotid stenosis, however, neurosurgical clipping of an unruptured intracranial aneurysm with the patient under general anesthesia may increase the perioperative risk of ischemic stroke. Even though CAS before neurosurgical clipping is preferred, a sudden rise in perfusion pressure and subsequently required high-dose antiplatelets may increase the risk of aneurysm rupture. Although aneurysm coiling first is a rational approach, particularly in case of procedures performed under local anesthesia, there are technical problems concerning how to embolize aneurysms through the cervical carotid bifurcation stenosis. Unless the ipsilateral intracranial arteries are opacified well after placing a microcatheter through the severe carotid stenosis (≥95%), dilation of the carotid stenosis before coiling is required. If the intracranial arteries are opacified well even after placing a microcatheter through the severe carotid stenosis, the ipsilateral aneurysm can be treated first.
Treatment strategy must be planned regarding safety, which is the highest priority, particularly in an elective procedure in a patient with a carotid stenosis coupled with an ipsilateral unruptured aneurysm. To reduce the risk of aneurysm rupture following carotid dilation, complete repair of aneurysms before carotid dilation is expected. Aneurysms do not heal immediately after coiling; a few months are required for complete repair. After angiographically confirming that the aneurysm is still obliterated at least 1 month after coiling, carotid stent placement is performed.
In case of a symptomatic cervical carotid bifurcation stenosis coupled with a coexisting cerebral aneurysm in the carotid distal segment, staged endovascular treatment is a rational option, and a support-wire technique through a guide catheter with a large internal diameter is very useful for stability of the procedures during aneurysm coiling, unless peripheral blood flow of the distal ICA is disturbed during the procedures.
Acknowledgments
We acknowledge the secretarial assistance of Nozomi Chiba and the specialized assistance of nurses and radiologic technicians in our neuroendovascular catheterization department.
References
- Received March 10, 2008.
- Accepted after revision April 16, 2008.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Tandem cervical carotid stenting for stenosis with flow diversion embolisation for the treatment of intracranial aneurysms
- Safety and effectiveness of emergency carotid artery stenting for a high-grade carotid stenosis with intraluminal thrombus under proximal flow control in hyperacute and acute stroke