
Abstract
Summary: Two cases of a second dural arteriovenous fistula (DAVF), both developing in different locations after selective transvenous embolization of the first DAVF, are presented. One recurrent DAVF developed on the sigmoid sinus 5 months after transvenous embolization of a DAVF in the paratransverse sinus channel, and the other recurrence developed around the jugular bulb 5 months after transvenous embolization of a cavernous DAVF. The former was obliterated by a second embolization, and the latter disappeared spontaneously at 20 months.
Transvenous embolization has been widely accepted as an effective treatment for dural arteriovenous fistulas (DAVFs). A DAVF completely occluded by transvenous embolization rarely recurs. A few cases of development of a second DAVF in a different location after transvenous embolization of the first DAVF have been reported (1–4). We report an additional two cases with recurrent DAVF in different locations and discuss the pathogenesis of the fistula.
Case Reports
Case 1
A 62-year-old man presented with pulsatile tinnitus in his left ear. Angiography demonstrated DAVF of a venous pouch adjacent to the transverse sinus (Fig 1A), fed by the left middle meningeal artery, the bilateral occipital arteries, the left posterior meningeal artery, and the meningohypophyseal artery. The DAVF was draining into the left jugular vein and into the contralateral transverse sinus. Selective transvenous embolization of the venous pouch was performed via the right femoral vein. A microcatheter (Rapid Transit; Cordis, Johnson & Johnson, Miami, FL) was introduced into the venous pouch, and it was packed with detachable coils (Detach-18, Detach-11; Cook Europe, Bjaerverskov, Denmark) and fibered platinum coils (Trüfil; Cordis). Angiography after selective transvenous embolization showed complete obliteration of the DAVF with preservation of normal venous drainage (Fig 1B and C). The tinnitus disappeared immediately after transvenous embolization.

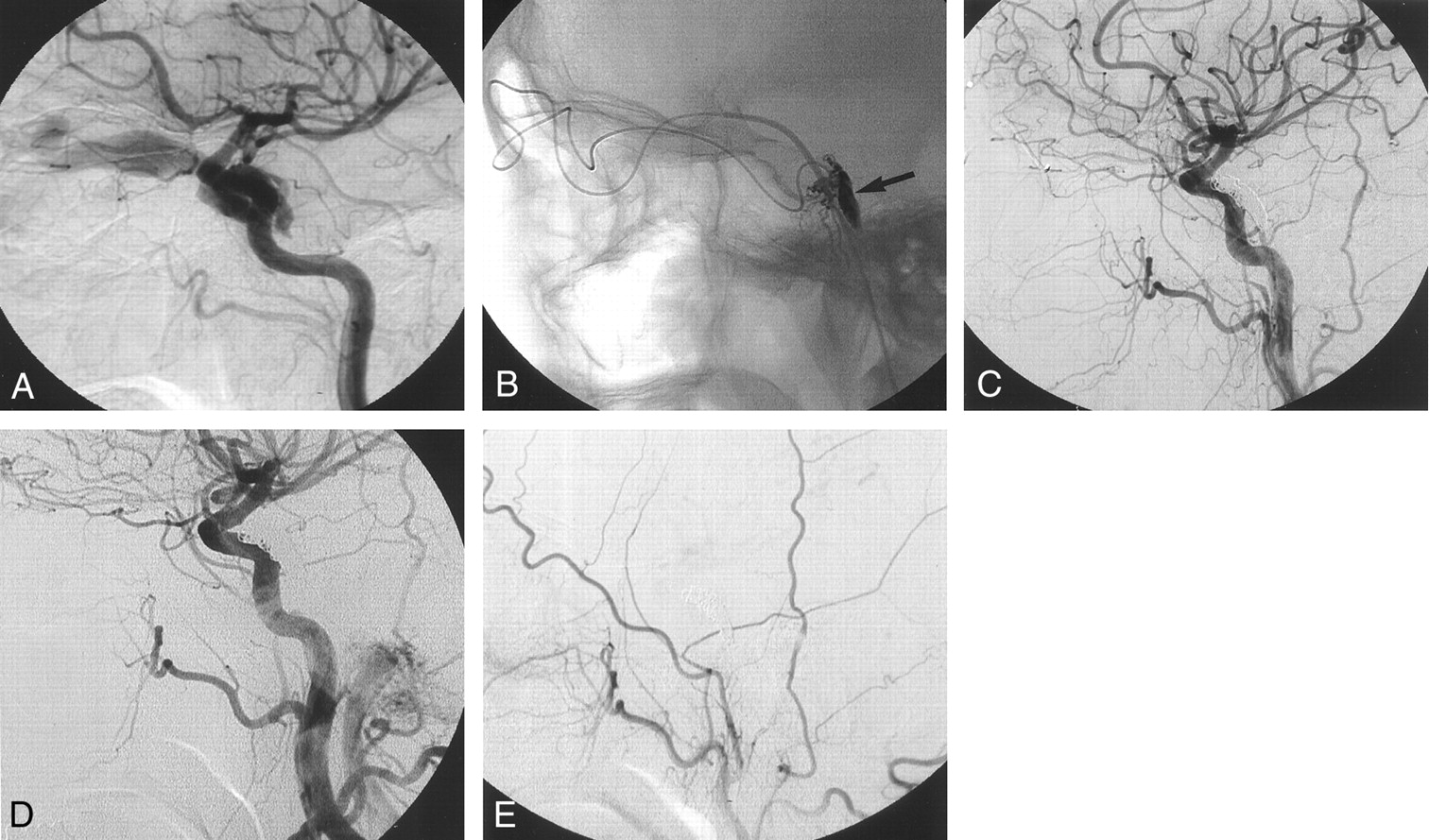
Images in a 62-year-old man who developed a second DAVF at the left sigmoid sinus after selective transvenous embolization of the first DAVF within or adjacent to the transverse sinus wall.
A, Right anterior oblique arteriogram with simultaneous injection from the bilateral external carotid artery shows a DAVF adjacent to the left transverse sinus, fed by the bilateral occipital arteries and the left middle meningeal artery. A fistulous channel (arrows) exists alongside the patent transverse sinus and drains into the sinus.
B and C, Arterial phase (B) and venous phase (C) left common carotid arteriograms obtained immediately after selective transvenous embolization of the fistulous pouch show complete obliteration of the DAVF and patent transverse sinus. Arrows indicate the coils.
D, Left external carotid arteriogram obtained 5 months after transvenous embolization shows a new DAVF at the sigmoid sinus, draining into the left superior petrous sinus. Occlusion of the left sigmoid-jugular junction is also noted.
E, Lateral view of selective injection from a microcatheter advanced via the inferior petrous sinus and superior petrous sinus into the sigmoid sinus. Occlusion of the left sigmoid-jugular junction is noted.
F, Left common carotid arteriogram obtained 8 months after the second transvenous embolization shows disappearance of the DAVF.
Five months after transvenous embolization, the patient presented with slight tinnitus in the left ear. Angiography revealed a new DAVF involving the left sigmoid sinus, fed by the left occipital artery and the left middle meningeal artery (Fig 1D). Occlusion of the proximal end of the left sigmoid sinus and the distal end of the left jugular vein was noted (Fig 1E), and the DAVF was mainly drained through the left superior petrous sinus and inferior petrous sinus into the suboccipital venous plexus. Transvenous embolization was again performed via the right femoral vein. A microcatheter (Excelsior; BSJ, Tokyo, Japan) was advanced via the inferior petrous sinus and superior petrous sinus into the sigmoid sinus because of the difficulty of advancing the microcatheter through the occluded jugular-sigmoid junction into the sigmoid sinus. Detachable coils were introduced into the sinus by means of the microcatheter. Angiography after the second transvenous embolization showed nearly complete obliteration of the DAVF. The patient returned to a normal everyday life. Follow-up angiography 8 months after the second embolization showed disappearance of the DAVF without new lesions (Fig 1F).
Case 2
A 66-year-old woman had a 2-year history of left proptosis chemosis at presentation. MR imaging showed abnormal flow voids representing the left cavernous sinus and the left superior ophthalmic vein. Angiography demonstrated a DAVF at the left cavernous sinus (Fig 2A), fed by the middle meningeal artery, the ascending pharyngeal artery, and the meningohypophyseal artery. The left inferior petrous sinus was occluded, and the DAVF drained via the left superior ophthalmic vein and the angular vein to the superficial temporal vein. Transvenous embolization was performed from the right femoral venous approach. First, a transvenous approach via the occluded left inferior petrous sinus was attempted, but this attempt failed. A microcatheter (Rapid Transit; Cordis) was advanced through the left superficial temporal vein, angular vein, and superior ophthalmic vein into the cavernous sinus (Fig 2B). The shunt portion of the cavernous sinus was packed with detachable coils (IDC-18; BSJ) and fibered platinum coils. Angiography performed after transvenous embolization showed complete obliteration of the cavernous DAVF with no other DAVFs appearing (Fig 2C), and the patient’s symptoms disappeared within 1 month.

Images is a 66-year-old woman with development of a second DAVF around the left jugular bulb after transvenous embolization of a cavernous DAVF.
A, Left common carotid arteriogram shows a DAVF at the left cavernous sinus, draining into the left superior ophthalmic vein.
B, Lateral view of selective injection from a microcatheter advanced through the left superficial temporal vein and angular vein into the left cavernous sinus. Arrow indicates tip of the microcatheter.
C, Left common carotid arteriogram obtained immediately after transvenous embolization shows complete obliteration of the cavernous DAVF.
D, Left common carotid arteriogram obtained 5 months after transvenous embolization shows a new DAVF around the left jugular bulb. Cavernous DAVF reveals stable occlusion.
E, Left external carotid arteriogram obtained 20 months after transvenous embolization shows spontaneous occlusion of the second DAVF.
Follow-up angiography performed 5 months after transvenous embolization showed development of a new DAVF around the left jugular bulb (Fig 2D), fed by the left occipital artery and the left ascending pharyngeal artery, and draining into the jugular vein. Normal venous drainage via the left transverse-sigmoid sinus to the left jugular vein was also noted. Because she had no clinical symptoms, she was observed without further treatment. Follow-up angiography at 20 months after transvenous embolization showed spontaneous disappearance of the second DAVF (Fig 2E).
Discussion
Although a DAVF is generally thought to be an acquired lesion without an intervening nidus, its pathogenesis has not been established. DAVFs are frequently associated with the restrictive change of the sinus adjacent to the fistula, and several reports have suggested that a DAVF is formed after recanalization of the thrombosed sinus (5, 6). However, sinus thrombosis was observed less frequently at histopathologic examinations. Hamada et al (7) investigated the histopathologically resected specimens of nine patients with DAVF. Sinus occlusion was seen on angiograms in six of nine cases; however, sinus thrombosis was histopathologically confirmed in only four cases, including one in which thrombus was caused by transvenous coil embolization. Dural artery and dilated venules directly communicated within the sinus wall.
Similar results of a histopathologic study were reported by Nishijima et al (8). According to their study, arteriovenous fistulas located in the dural sinus wall and/or the adjacent dura mater and stenosis or occlusion of the sinuses occurred mainly due to the marked thickening of their intima and the development of abnormal vascular networks within their walls. Some cases of DAVF confirmed radiologically or surgically to be located in the sinus wall have been reported (9, 10). These cases were thought to be an unusual variant. However, Nishijima et al (8) suggested that these arteriovenous fistulas within the wall of affected sinuses develop in the early stage of the disease.
In case 1, a DAVF was located adjacent to the patent transverse sinus and drained into the sinus. Although histologic confirmation was not obtained, a venous pouch was demonstrated along the sinus at angiography, which suggested the DAVF was located in the sinus wall. After transvenous embolization, a second DAVF developed in the sigmoid sinus. The first DAVF may represent the early stage of the disease, a supposition that is supported by the hypothesis of Nishijima et al, previously described. To our knowledge, four cases of development of a second DAVF after successful transvenous embolization have been reported in the English language literature (1–4). In all of these cases, the first DAVF was located in the cavernous sinus, and the second DAVF was located in the ipsilateral sigmoid sinus, around the ipsilateral jugular bulb. Several hypotheses with regard to the pathogenesis of the second or multiple DAVFs were considered. The shunt flow from a DAVF might cause turbulence of the normal venous flow, which could lead to stagnation and thrombosis at a site away from the original DAVF. A second lesion might then develop by recanalization. However, in case 2, no signs of sinus thrombosis were observed during the follow-up period.
In all of the cases previously reported on, including our two cases, in which development of a second DAVF occurred at the ipsilateral side to the first DAVF after transvenous embolization, a microcatheter and/or microguidewire were manipulated around the site where the second DAVF developed. There is a possibility that these manipulations played a role in the development of the second DAVF. However, development of a second DAVF could occur after transarterial embolization or spontaneous regression of the first DAVF (11, 12). There is another possibility that the template of the second fistula already existed in the vasculature, but was an angiographically occult lesion at the initial embolization and had to mature over time with or without stimulation by the initial embolization.
Studies using a rat model demonstrated that DAVFs formed in a group with venous hypertension and no DAVF formed in a group without venous hypertension (with sinus thrombosis) (13, 14). A few animal and human studies regarding an angiogenic cause of DAVFs have been reported (13, 15). Uranishi et al (15) demonstrated excessive expression of angiogenic factors, including vascular endothelial growth factor (VEGF) and basic fibroblast growth factor, in the wall of DAVFs in humans. According to these studies, venous hypertension and angiogenesis might play a more important role than sinus thrombosis, and sinus thrombosis might contribute to venous hypertension.
More recently, Sure et al (16) investigated the proliferative and angiogenic capacities of endothelium of cerebrovascular malformations including 13 cavernomas and 25 arteriovenous malformations (AVMs). In 18 of 25 cases of AVMs in their study, transarterial embolization was performed before surgery. VGEF was expressed in a much higher percentage of cases in which the patient underwent preoperative embolization (72.2%) compared with cases without embolization (28.5%). VEGF is the main cytokine secreted during wound healing or tissue hypoxia. The authors concluded that (partial) embolization of cerebral AVMs leads to a local endothelial hypoxia within the AVM nidus, which mediates the neovasculalization and growth of the malformation. Endovascular treatment, especially transvenous embolization, and DAVF itself might change the dural venous circulation and increase venous hypertension. Furthermore, expression of angiogenesis might occur due to tissue hypoxia as a result of venous occlusion created by the initial transvenous embolization. Venous hypertension and angiogenesis will promote the progression of the disease process and will play an important role in the development of the second fistula. The presence or development of sinus thrombosis might contribute to this process.
In our two cases, the recurrent DAVF in the first case was treated with transvenous embolization because of the presence of tinnitus and retrograde venous drainage, and the recurrence in the second case spontaneously regressed. These second DAVFs could be treated for the same indication and by the same strategy as the first DAVFs. However, careful follow-up of patients is needed.
References
- Received March 29, 2001.
- Accepted after revision August 29, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Progressive versus Nonprogressive Intracranial Dural Arteriovenous Fistulas: Characteristics and Outcomes
- Clinical and Angiographic Characteristics of Multiple Dural Arteriovenous Shunts
- Onyx 18 embolisation of dural arteriovenous fistula via arterial and venous pathways: preliminary experience and evaluation of the short-term outcomes
- Efficacy of DynaCT Digital Angiography in the Detection of the Fistulous Point of Dural Arteriovenous Fistulas