
Abstract
Summary: We report serial MR findings in a middle-aged woman with a neurenteric cyst involving the cerebellopontine angle cistern with xanthogranulomatous changes. On the initial gadolinium-enhanced T1-weighted MR images, the solid portion of the lesion had homogeneously strong enhancement. Follow-up MR images obtained 6 months later showed that the mass had increased in size; however, the solid portion decreased in size. The enhancing solid portion corresponded to the xanthogranulomatous changes on pathologic correlation.
Neurenteric cysts are congenital endothelium-lined structures that are most commonly located in the cervical and thoracic spinal canal ventral to the spinal cord. Intracranial lesions are rare and located mainly in the posterior cranial fossa, often near the midline in the fourth ventricle. Although histologically benign, intracranial lesions can cause major neurologic deficits, and they can be the source of serious infection if detection and treatment are delayed (1). We describe the serial MR findings correlated with the pathologic findings of this rare lesion involving the cerebellopontine angle cistern.
Case Report
A 35-year-old woman presented with a 3-year history of headache. Physical and neurologic examinations revealed no abnormalities.
MR imaging at 1.5 T revealed a well-circumscribed mass in the left cerebellopontine angle cistern. The mass was homogeneously hyperintense relative to CSF on T1-weighted MR images (Fig 1A and B) and isointense relative to CSF on T2-weighted MR images (Fig 1D). A small solid portion abutted the pons, which had homogeneously strong enhancement on gadolinium-enhanced T1-weighted MR images (Fig 1C). Follow-up MR images obtained 6 months later shows that the entire mass had markedly increase in size; however, the solid portion decreased in size (Fig 2A) and (2B) and had subtle enhancement (Fig 2B). On CT scans (not shown), the mass was slightly hyperattenuating relative to the cerebellar parenchyma, but lesion demarcation was not clear because of the prominent beam-hardening artifact. On angiograms (not shown), the mass showed no evidence of vascularity from either an intra- or extracranial supply. The mass displaced the basilar artery to the right side. The preoperative diagnosis was an arachnoid cyst or epidermoid cyst, although the high signal intensity that reflected a large protein contents and the strong enhancement were unusual.
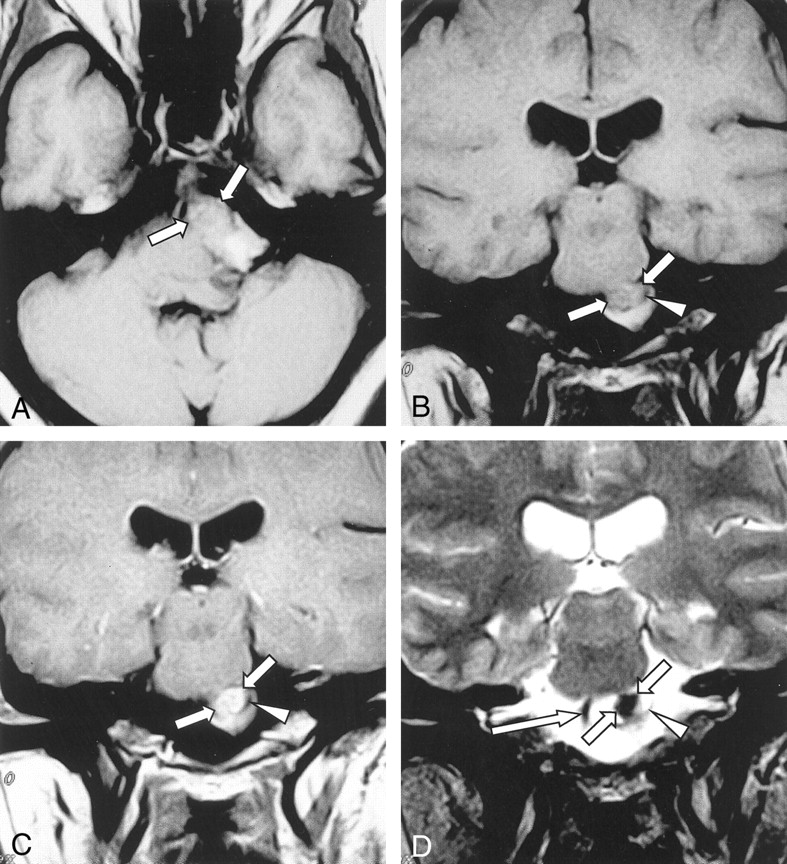
Initial MR images in a 35-year-old woman with headache.
A, Axial T1-weighted (520/20) image shows a well-circumscribed mass in the left cerebellopontine angle cistern. It is hyperintense to CSF; this finding suggests a high-protein-content cystic mass. Several hypointense areas are present in the mass, with a large solid area (arrows) in the anterior portion of the mass.
B and C, Coronal T1-weighed (B) and contrast-enhanced T1-weighted (C) images (520/20) show homogeneous, strong enhancement of the solid nodule (arrows) surrounded by a thin low-signal-intensity rim (arrowhead).
D, On this coronal T2-weighed (3600/105) image, the center of the solid nodule is hypointense (short arrows), whereas the peripheral portion of the solid nodule is hyperintense. A thin low-signal-intensity rim (arrowhead) is also depicted. The mass displaced the basilar artery (long arrow) to the right side.

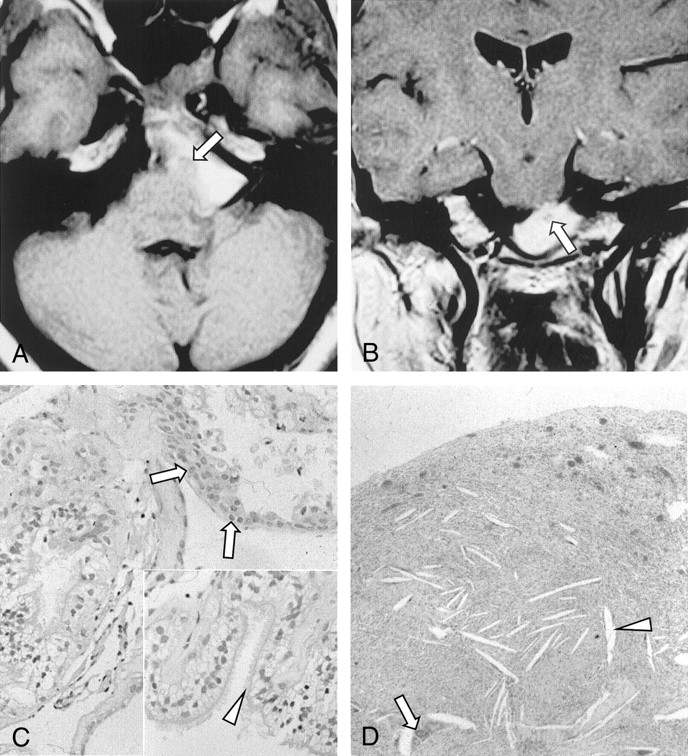
Follow-up MR images obtained 6 months after the initial MR images and a pathologic photomicrograph.
A, Axial T1-weighted (520/20) MR image shows a marked increase in the size of the mass. However, the solid nodule (arrow) has decreased in size.
B, Coronal contrast-enhanced T1-weighted (520/20) MR image shows a decrease in size as well as subtle enhancement of the solid nodule (arrow).
C, Photomicrograph demonstrates ciliated columnar epithelium. Squamous metaplasia (arrows) lining the wall of the cyst (hematoxylin-eosin, original magnification ×100). Inset: High-power photomicrograph clearly demonstrates ciliation (arrowhead) (original magnification ×200).
D, Photomicrograph of the solid nodule demonstrates xanthogranulomatous change, with foamy macrophages, chronic inflammatory cells, multinucleated giant cells (arrow), and a cholesterol cleft (arrowhead) (hematoxylin-eosin stain, original magnification ×100).
Excision of the mass was performed via a far-lateral suboccipital approach. The mass was extra-axial and intradural. It was lined with a thin translucent membrane and contained a greenish, turbid, mucoid fluid. An 8-mm, well-circumscribed, ovoid solid nodule adhered to the left side of the pons and left sixth cranial nerve. The solid nodule was gray-tan and rubbery firm. Microscopically, the thin membrane was composed of ciliated columnar epithelium and some squamous metaplasia; it resembled bronchial epithelium (Fig 2C). The solid nodule was composed of foamy histiocytes, chronic inflammatory cells, multinucleated giant cells, and cholesterol clefts, and the photomicrograph showed a xanthogranulomatous reaction (Fig 2D). Immunohistochemical studies revealed positive staining of the epithelial cell lining with cytokeratin, epithelial membrane antigen, and carcinoembryonic antigen, but staining with S-100 protein was negative. The histopathologic differential diagnosis included a colloid cyst and Rathke cleft cyst; however, these diagnoses were easily excluded because of the location of the lesion in the cerebellopontine angle cistern. Therefore, this cystic lesion was diagnosed as a neurenteric cyst on the basis of the histologic findings as well as its location.
Discussion
Neurenteric cysts arise secondary to the persistence of the neurenteric canal, which is the temporary connection between the amniotic and yolk sacs during the third week of embryogenesis. Persistent endoectodermal adhesions or a persistent adhesion between the notochord and the endoderm may produce a notochordal dysgenesis such as diastematomyelia, and a neurenteric cyst may result (2–4).
A xanthogranulomatous change is a nonspecific chronic cellular reaction with prominent lipid-laden histiocytes or macrophages, the so-called foam or xanthoma cells (5). In addition to xanthogranulomatous pyelonephritis and cholecystitis, the occurrence of a xanthogranulomatous reaction is known to be occur in benign, noninflammatory cystic or cystlike lesions, such as a neurenteric cyst, colloid cyst, epidermoid cyst, cholesterol granuloma, choroid plexus, and even renal or pancreatic cyst, although this is very rare (6–8). Moreover, MR imaging or CT findings of a xanthogranulomatous reaction in noninflammatory cystic or cystlike lesions are rarely reported, and descriptions of it are poor (8). In this case, the associated hypervascularity of the inflamed tissue indicates the strong enhancement of the xanthogranulomatous reaction in the solid nodule (5). To our knowledge, MR images of enhanced neurenteric cysts have not been reported. The signal intensity of xanthogranulomatous reaction in the solid nodule was low on T2-weighted MR images; this finding reflected the high cellularity due to the presence of compact foamy histiocytes and chronic inflammatory cells. This size and degree of enhancement of the solid nodule decreased on follow-up MR images obtained 6 months later, probably as the chronic xanthogranulomatous inflammatory change underwent an atrophic change in volume and the active inflammation that accompanied the hypervascularity decreased. This organization to chronic and atrophic change is consistent with the hard nature of the gross specimen of the solid nodule of the cyst. Interestingly, the solid nodule that showed the xanthogranulomatous reaction adhered to the adjacent pons in the surgical field, making complete dissection difficult. These surgical findings may reflect focal rupture of the contents of the cyst as in a previously reported case of xanthogranulomatous colloid cyst (7), although the evidence of frank rupture could not be found during surgery or pathologic evaluation of the specimen.
Neurenteric cysts are usually isointense or slightly hyperintense relative to CSF on T1-weighted MR images and isointense relative to CSF on T2-weighted MR images (2). However, they may produce a higher signal intensity than CSF on T1-weighted MR images, and their size may fluctuate depending on hemorrhage and their protein content (1, 3, 4, 6, 9). On CT scans, a neurenteric cyst usually appears as a low-attenuating nonenhancing lesion (3, 10). However, as in our case, a slightly high attenuation can be seen on CT scans; this finding reflects its protein-rich and possibly hemorrhagic contents. A neurenteric cyst is avascular, and angiographic findings are usually normal except for a displacement of adjacent vessels (11).
A number of cystic structures can arise in the cerebellopontine angle cistern, including an arachnoid cyst, epidermoid cyst, dermoid cyst, cholesterol granuloma, cysticercosis, and cystic tumors (2, 3). An arachnoid cyst is isointense to CSF on MR images obtained with all sequences. Therefore, its differentiation from a neurenteric cyst is difficult when the neurenteric cyst has the same signal intensity as CSF. An epidermoid cyst is usually isointense to CSF on all MR images. However, diffusion MR imaging is helpful in its diagnosis. A dermoid cyst has high signal intensity similar to that of fat; however, frequent heterogeneity and its midline location make the diagnosis of dermoid cyst unlikely in this case. A cholesterol granuloma has high signal intensity on T1- and T2-weighted MR images due to the blood breakdown products (12). However, it is usually extradural, especially in the petrous apex, and bone destruction is common (12). Cysticercosis can appear as a cystic lesion with an enhancing mural nodule that represents a scolex; however, a frequently enhancing rim and multiplicity are helpful in the diagnosis of cysticercosis. In cystic tumors, such as a schwannoma or meningioma, clear peripheral or intratumoral enhancement is certainly present.
A neurenteric cyst is analogous to a colloid cyst and Rathke cleft cyst from a histopathologic point of view; they are lined by a columnar epithelium of presumed endodermal origin (4). Therefore, imaging studies can be used to confirm the final diagnosis by determining the location of the lesion. For example, a colloid cyst is located in the third ventricle, and a Rathke cleft cyst is in the midline near the sellar area.
The treatment of choice for a neurenteric cyst is surgical removal of the cyst wall. The location of the cyst determines the feasibility of surgery, and its prognosis depends on the size and location of the cyst (3). Recurrence is rarely reported, and the clinical course is usually benign, even after subtotal removal of the lesion (1).
Acknowledgments
We are very grateful to Bonnie Hami, MA, Department of Radiology, University Hospitals of Cleveland, Ohio, for her editorial assistance.
References
- Received August 8, 2001.
- Accepted after revision September 10, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.