
Abstract
Summary: Lyme disease is a multi-system organ disease caused by Borrelia burgdorferi. Although ocular manifestations have been reported, these remain a rare feature of the disease. To our knowledge, the radiology literature has not documented orbital Lyme disease both before and after treatment. We present the MR imaging findings of florid Lyme disease affecting the extraocular muscles in a 46-year-old man. A follow-up MR imaging study performed 6 months after a course of antibiotic therapy revealed complete resolution of the myositic changes.
Lyme disease is caused by the spirochete Borrelia burgdorferi and is, at present, the most common arthropod-borne infectious disease in Europe and the United States. It is transmitted primarily by Ixodes dammini ticks, or deer ticks, in the northeast and upper midwest United States, by Ixodes pacificus in the western United States, and by Ixodes ricinus in Europe. The disease is transmitted to humans primarily in the spring, summer, and early fall. Lyme disease can affect the skin, nervous system, heart, eyes, and joints and is diagnosed in patients based on exposure to an endemic area, a skin rash, and usually a positive serologic test for B burgdorferi ≥6 weeks after infection. Lymphadenopathy, if present, is usually in regional draining nodes (1–4).
Ocular findings associated with Lyme disease were first noted by Steere et al (2) who reported conjunctivitis and periorbital edema. Since then, there have been isolated reports of Lyme disease causing belpharospasm, iridocyclitis, panophthalmitis, optic neuritis, and orbital myositis (3, 4).
We report a case of Lyme disease involving the extraocular muscles with successful resolution of the myositic changes after treatment with docycycline. To our knowledge, this is the first case report in the radiology literature documenting complete disease resolution.
Case Report
A 46-year-old man presented with a 2-week history of headache and diplopia. He had no orbital pain or conjunctival injection, and he had no history of thyroid disease, granulomatous disease, or trauma. He lived in New Jersey, near a heavily wooded area, and his medical history was significant for a skin rash on the right arm accompanied by slight fever and chills 3 weeks before presentation. The patient had received no treatment for the rash other than acetaminophen. His remaining medical history was otherwise unremarkable.
Physical examination revealed normal visual acuity in both eyes. Marked restriction of lateral gaze and 3-mm proptosis of the right eye were noted. A corneal reflex was present. The pupils were briskly reactive, and there was no afferent pupillary defect. The remaining results of the ophthalmic and physical examinations were normal. No evidence of focal neurologic deficit was detected. Thyroid function test results were normal, and complete blood count and differential blood count were normal.
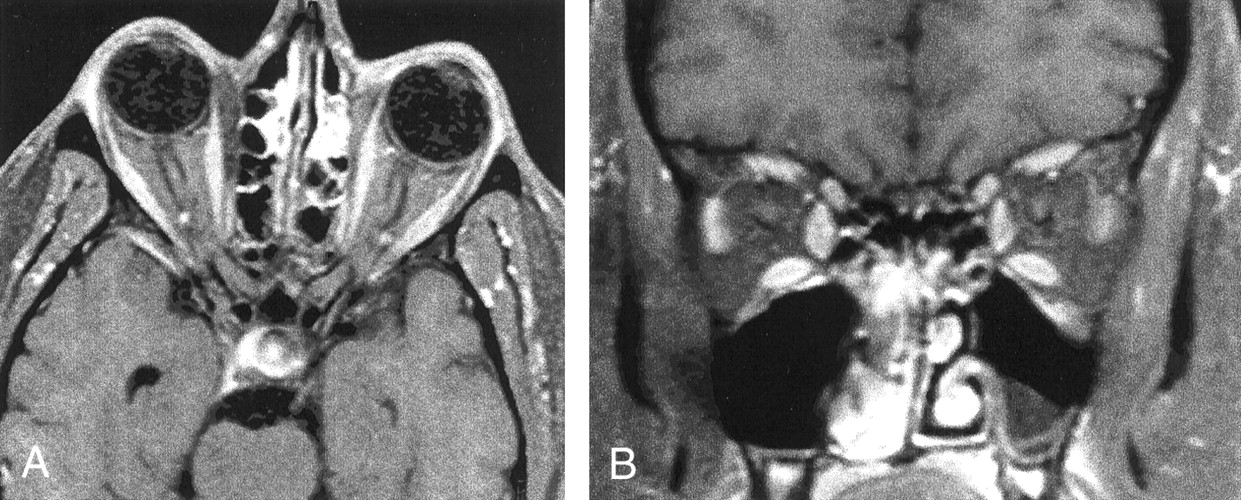
MR imaging showed diffuse thickening of the extraocular muscles with some tapering near their tendinous insertions (Fig 1). No focal mass was seen. There was no evidence of an abscess. The bony walls of the orbit appeared intact, and the paranasal sinuses had only minimal inflammatory type mucosal thickening. The visualized brain parenchyma was normal.

Contrast-enhanced fat-suppressed T1-weighted MR images obtained through the orbits show diffuse homogeneous thickening of the medial, lateral, and inferior rectus muscles of the right orbit. Minimal thickening of the superior muscle group can be seen. The tendinous insertions are not involved. Scattered inflammatory changes in the ethmoid sinuses and the left maxillary sinus can be seen.
A, Axial view.
B, Coronal view.
Based on the clinical history of the skin rash and the patient’s living in an endemic area, a working diagnosis of Lyme disease with orbital involvement was established. Doxycycline (100 mg twice a day for 3 weeks) was administered. During the treatment period, there was a gradual decrease in the limitation of extraocular movements and a slow resolution of the proptosis. At the completion of this course of antibiotic, the patient experienced complete clinical resolution of the orbital symptoms and the results of a physical examination were unremarkable. Three months after the completion of therapy, a follow-up MR imaging study (Fig 2) revealed complete resolution of the previously noted myositic changes.
Contrast-enhanced fat-suppressed T1-weighted MR images obtained through the orbits after treatment with doxycycline show complete resolution of the previously noted homogeneous muscle thickening. Scattered inflammatory changes in the ethmoid sinuses and the left maxillary sinus remain.
A, Axial view.
B, Coronal view.
Discussion
Lyme disease is the most common arthropod-borne infection in the United States (5). The disease can be divided into three clinical stages (6). Stage I is classically characterized by a centrifugally expanding erythematous annular rash, erythema migrans, that occurs at the site of the tick bite. Stage II begins weeks to several months after initial infection, with multi-organ involvement and a predilection for the cardiovascular system and CNS. Stage III, the chronic phase of Lyme disease, occurs months after the initial onset and is characterized by involvement of the joints, peripheral nervous system, and subcutaneous tissues.
Ocular involvement is not commonly observed in association with Lyme disease. It has been reported that the spirochete may be responsible for an acute orbital presentation during its early stage of dissemination, but the spirochete may also remain dormant in the eye, accounting for late ocular manifestations (7). The various orbital findings reported in association with Lyme disease include follicular conjunctivitis, occurring in 10% of the patients (8); keratosis, the most common orbital finding (7); inflammatory syndromes, involving all or parts of the eye (9); and neuro-ophthalmologic manifestations, including neuroretinitis, involvement of multiple cranial nerves, optic atrophy, and disc edema (7).
The criteria used for establishing orbital Lyme disease include lack of evidence of other diseases, other clinical findings consistent with Lyme disease, occurrence in patients living in endemic areas, positive serology, and response to prescribed treatment.
In our case, on basis of the MR images, multifocal disease was affecting the extraocular muscles. Although the tendon insertions did not appear to be involved, the possibility of pseudotumor or even lymphoma had to be considered. The involvement of the extraocular muscles with streakiness of retrobulbar fat also raised the possibility of thyroid ophthalmopathy. The lack of involvement of the lacrimal glands, the absence of pathologic lymphadenopathy, systemic symptoms such as weight loss, and normal blood test results made the diagnosis of lymphoma unlikely. The normal thyroid function tests and a normal thyroid examination made thyroid ophthalmopathy less likely. The excellent response to the appropriate antibiotic in a patient with a known rash living in an endemic area established the diagnosis of Lyme disease. There was also no history, symptoms, or imaging findings to suggest a granulomatous-type process.
Biopsy findings from cases of Lyme myositis involving peripheral musculature showed infiltration of lymphocytes, plasma cells, and macrophages with or without atrophic fiber change (10–13). The Dieterle silver stain has been successful in revealing B burgdorferi in most biopsy specimens (14, 15). Recently, polymerase chain reaction studies have been used to confirm the presence of Lyme disease.
The pathophysiology regarding Lyme myositis remains unclear. A hematogenous dissemination to the involved musculature with a subsequent immunologically mediated muscle reaction seems to be the most likely cause for the inflammation.
In summary, orbital involvement by B burgdorferi is an unlikely occurrence. However, in the appropriate clinical presentation and lacking evidence of other disease conditions, Lyme disease should be considered in the differential diagnosis of ocular lesions. Imaging further helps in establishing the diagnosis. Also, follow-up MR imaging studies, as in our case, can be used to document resolution of the disease process.
References
- Received September 25, 2001.
- Accepted after revision November 9, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}