
Abstract
BACKGROUND AND PURPOSE: Petrous apex cephaloceles (PACs) are uncommon lesions that are usually incidental but may be symptomatic. We reviewed MR and CT studies in 10 patients with PACs to identify characteristic imaging features that facilitate their diagnosis.
METHODS: MR and CT studies from 10 patients with PACs were reviewed retrospectively. In each case the PAC was characterized by lesion center, signal intensity or attenuation, adjacent petrous apex pneumatization, and its relationship to Meckel's cave. Intraoperative findings were reviewed in the three cases in which surgery was performed.
RESULTS: All 10 patients had lobulated expansile cystic petrous apex lesions centered along the posterolateral margin of Meckel's cave. All cysts were contiguous with Meckel's cave. Three patients had bilateral PACs. Four patients had symptoms that could potentially be explained by the PAC, while findings in the other six were incidental observations. Three patients underwent surgery, during which two lesions were diagnosed as meningoceles while the third was diagnosed as an arachnoid cyst protruding through a dural defect.
CONCLUSION: PACs represent a protrusion of meninges and CSF from the posterolateral portion of Meckel's cave into the petrous apex, which is their characteristic imaging appearance. PACs are usually incidental but may be symptomatic. Surgical intervention should be approached cautiously and undertaken only when symptoms are clearly linked to the presence of this lesion.
Although the petrous apex is a small area in the skull base, it displays myriad anatomic and pathologic variations. The petrous apex cannot be directly examined, so imaging plays a primary role in the evaluation of lesions in this area. Most petrous apex lesions are readily characterized as either surgical lesions (neoplastic lesions, inflammatory complications of air cell disease) or incidental nonoperative findings (asymmetric fatty marrow, trapped fluid) (1, 2). The majority of nonneoplastic petrous apex lesions are inflammatory complications of air cell disease (cholesterol granuloma, cholesteatoma, or mucocele).
Petrous apex cephalocele (PAC) is a rare lesion of the petrous apex (3–5). The pathologic explanation for this herniation from the posterolateral portion of Meckel's cave into the petrous apex has varied from meningocele to arachnoid cyst. Although case reports describing the diagnosis and management of this entity have appeared sporadically in the clinical literature, PACs have not been reported in the radiologic literature.
Prior reports of PACs have focused on the symptomatic subset of lesions requiring surgical intervention. In this report, we describe characteristic radiologic findings that mark a petrous apex lesion as a PAC. In addition, we establish the idea that PACs may frequently be asymptomatic, incidental observations made on brain MR images obtained for other clinical indications.
Methods
A retrospective review of two university medical center imaging archives (patients imaged between October 1990 and March 1997) produced 10 patients (eight female and two male; mean age, 48 years; range, 5 to 82 years) with PACs.
All 10 patients underwent MR imaging at 1.5 T. Nine patients (cases 1–5 and 7–10) were studied with conventional imaging (axial T1-weighted sequences without and with intravenous contrast material; coronal contrast-enhanced T1-weighted sequences; and axial and/or coronal T2-weighted fast spin-echo [FSE] sequences) using a standard head coil. Two patients (cases 6 and 7) underwent high-resolution T2-weighted FSE temporal bone imaging in the axial and coronal planes with a slice thickness of 2 mm with a 1-mm overlap, a matrix of 512 × 384–512, and a field of view of 20 × 10 cm using a 3-inch temporomandibular joint phase-array surface coil. Six patients (cases 1–4, 7, and 8) had high-resolution temporal bone CT in the axial and coronal planes with a slice thickness of 1 mm and a bone algorithm. One patient (case 4) underwent additional CT cisternography in the coronal plane with postprocessed axial reformations, a slice thickness of 1 mm, a field of view of 20 cm, and a bone algorithm. All imaging studies were examined for cyst center, lesion margins, and relationship to Meckel's cave and other adjacent structures. Lesion attenuation and signal intensity were noted.
Results
Clinical Findings
Patient information, including presenting clinical signs and symptoms, is provided in Table 1. We found inconsistent correlation between reported signs and symptoms and imaging findings. Four patients (cases 1–4) presented with clinical findings ipsilateral to the PAC. The remaining six patients (cases 5–10) displayed contralateral or nonspecific clinical findings that did not correspond to the presence of the PAC.
Patient data
Imaging Findings
The imaging findings in the positive apices were consistent among all 10 patients and easily distinguished from normal temporal bone studies (Fig 1) and inflammatory lesions (Fig 2). Thirteen of 20 apices had PACs. Seven patients manifested unilateral lesions, and three patients had bilateral abnormalities. All lesions were centered in the posterolateral portion of Meckel's cave and had sharply defined osseous margins with homogeneous central low attenuation on bone algorithm CT scans. In all patients, the trigeminal notch was eroded and the cysts extended a variable distance into the anterosuperior petrous apex. Once in the apex, the cysts redirected posteriorly and inferiorly, sometimes extending caudally as far as the posterior petrous internal carotid artery canal wall (cases 3, 4, 7, and 10). No cyst extended into the cerebellopontine angle or into the inner or middle ear structures. T1-weighted MR images showed a thin wall of intermediate signal intensity encircling each cyst, with mild rim enhancement. T2-weighted MR images revealed homogeneous hyperintensity characteristic of fluid. In all cases, the cyst appeared contiguous with Meckel's cave.
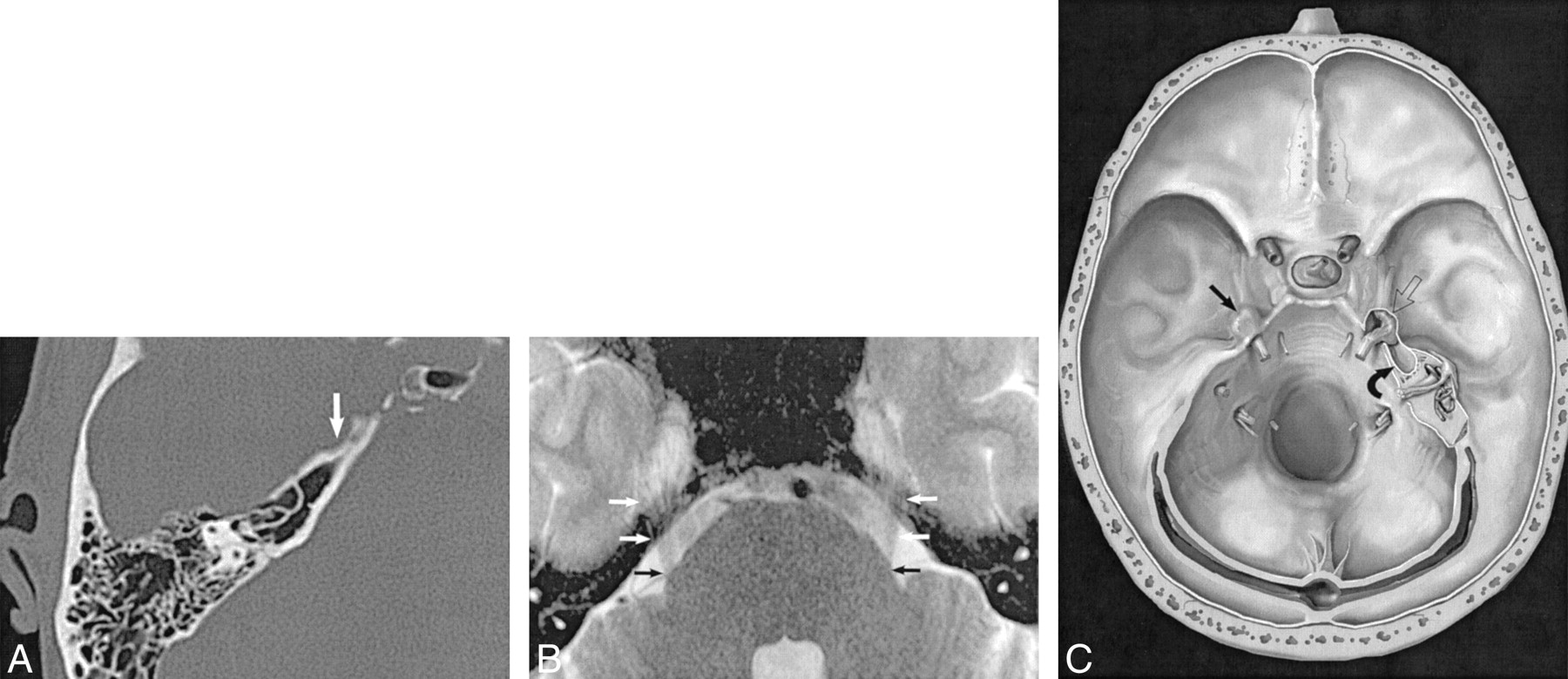
Normal appearance of Meckel's cave.
A, CT scan of temporal bone shows smooth anterior petrous apex scalloping at the trigeminal notch and inferior border of the porus trigeminus that delimits the posterior margin of Meckel's cave. The trigeminal notch is a smoothly scalloped area of the petrous apex on bone windows (arrow) that encloses the posterior portion of Meckel's cave.
B, High-resolution MR image shows CSF signal intensity in Meckel's cave and the contiguous porus trigeminus, the CSF portal by which the trigeminal nerve courses from the prepontine cistern over the petrous apex into Meckel's cave. This axial T2-weighted FSE (4000/94/4) MR image shows the cisternal trigeminal nerves (arrows) as they cross over the petrous apex into Meckel's cave to form the gasserian ganglion.
C, Artist's rendering of temporal bone portrays the normal appearance of the right Meckel's cave (straight black arrow) with dural covering in place. The left petrous apex depicts a PAC. The dura has been removed to demonstrate the gasserian ganglion within Meckel's cave (open arrow) in direct contiguity with the CSF-filled PAC extending posteriorly into the petrous apex (curved arrow). (Reproduced with permission from Electronic Medical Education Resource Group, 2001.)

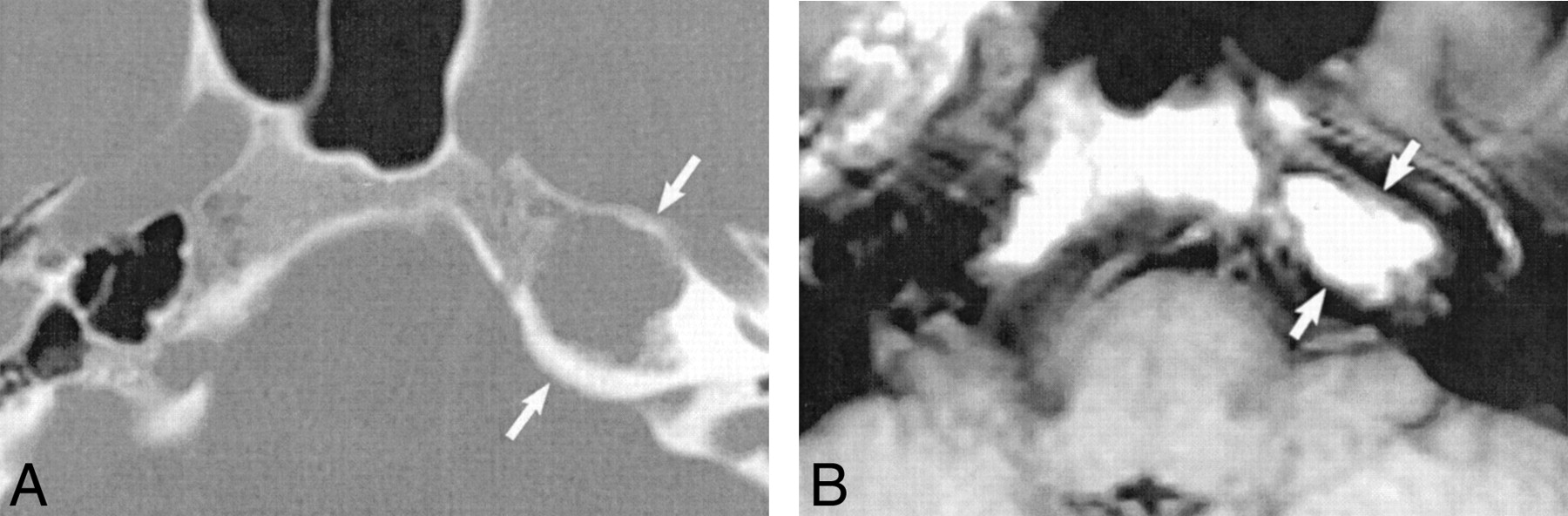
Cholesterol granuloma.
A, Axial CT scan shows a smoothly marginated expansile lesion (arrows) centered within the petrous apex, in contradistinction to a PAC, in which the mass is centered within the posterior portion of Meckel's cave and secondarily extends into the petrous apex.
B, Axial T1-weighted MR image confirms marked T1 shortening within the lesion (arrows), characteristic of cholesterol granuloma. Diagnosis was proved at surgical exploration.
Surgical Findings
Three patients underwent surgery because of trigeminal neuropathy (case 1), CSF otorrhea (case 2), and trigeminal neuralgia (case 3). In cases 1 and 3, a preoperative diagnosis of petrous apex cholesteatoma was made on the basis of imaging findings. No inflammatory change or cholesteatoma was found at surgery. In all three of these cases the cyst was followed from the petrous apex into Meckel's cave.
Case 1
A 25-year-old woman presented to the emergency room with a severe headache of 4 weeks' duration, left-sided facial numbness, and left lateral gaze palsy. Imaging revealed a cystic-appearing lesion centered over the left posterior portion of Meckel's cave, eroding into the petrous apex (Fig 3). A preoperative diagnosis of cholesteatoma was made on the basis of clinical signs and symptoms and imaging features.

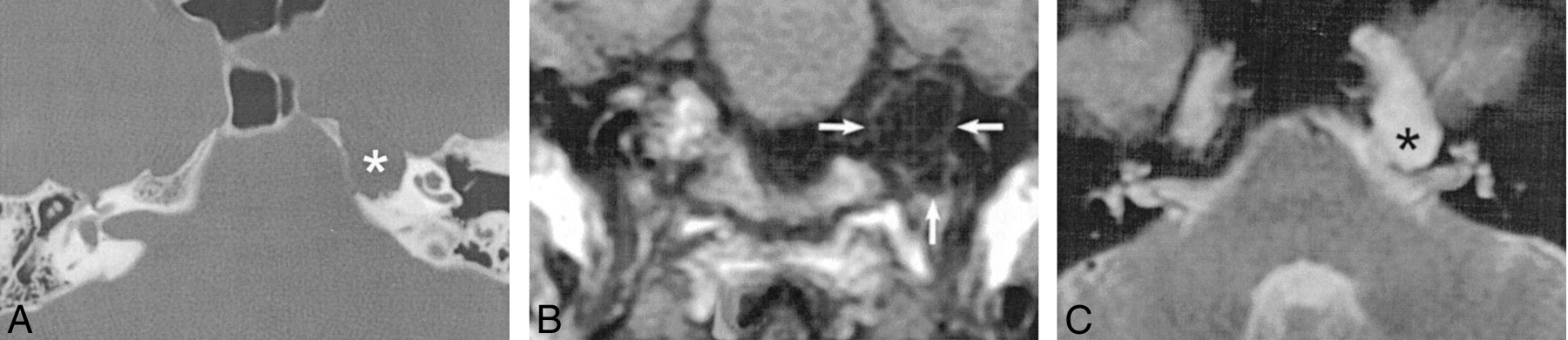
Case 1: 25-year-old woman with meningocele.
A, Axial bone algorithm CT scan reveals scalloping of the trigeminal notch and a sharply marginated lesion extending into the left petrous apex (asterisk).
B, Axial contrast-enhanced fat-saturated T1-weighted SE (650/16/2) MR image reveals a low-signal-intensity cyst with mild rim enhancement within the left petrous apex (arrow).
C, Axial T2-weighted FSE (4350/90/2) MR image confirms hyperintense fluid signal within the apex lesion (arrow).
Surgical exploration of the left temporal bone using an infratemporal postauricular surgical approach revealed a large dura-covered cyst contiguous with Meckel's cave. The dura was incised and the cyst entered, revealing prolapsed white fibrous neural strands splayed along the cyst wall. Because the dural lining was traversed to enter this lesion, the surgeon characterized it as a meningocele. Postoperatively, the patient's lateral gaze palsy improved but there was no significant improvement in trigeminal nerve symptoms.
Case 2
A 5-year-old boy presented with progressive conductive hearing loss in the right ear. Myringotomy produced CSF otorrhea. Preoperative imaging revealed a cystic-appearing right petrous apex lesion contiguous with Meckel's cave and an ipsilateral mastoid effusion (Fig 4). A right temporal craniotomy was performed, and an arachnoid-lined cyst was entered. The cyst extended from Meckel's cave into the petrous apex and drained into the mastoid air cell system. The surgeon concluded that the cyst was most characteristic of a petrous apex arachnoid cyst. Surgical repair of dural and osseous defects was performed with subsequent postoperative resolution of the CSF otorrhea.

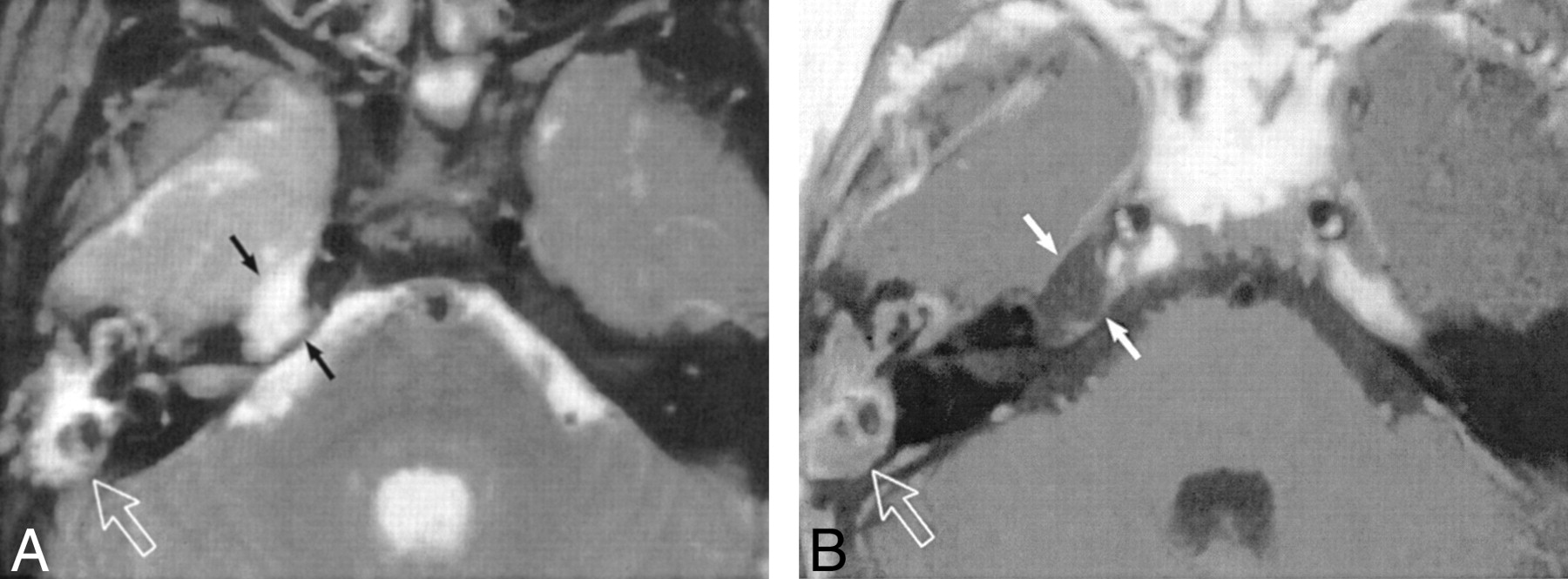
Case 2: 5-year-old boy with arachnoid cyst.
A, Axial T2-weighted FSE (4000/92/2) MR image reveals a cystic-appearing right petrous apex lesion with CSF signal intensity contiguous with Meckel's cave (black arrows). Also noted is an ipsilateral mastoid effusion (open arrow).
B, Enhanced axial T1-weighted SE (450/12/2) MR image shows a lesion in the apex with CSF signal intensity (white arrows). Open arrow denotes complex effusion.
Case 3
A 48-year-old woman presented with left third and fifth cranial neuropathies. Preoperative imaging (Fig 5) revealed a sharply marginated expansile left petrous apex mass on CT scans and fluid signal intensity characteristics (low T1, high T2 signal intensity) on MR images. A preoperative diagnosis of cholesteatoma was made. At surgery, a CSF-filled petrous apex cyst was identified with a surrounding dural membrane, most characteristic of a meningocele.
Case 3: 48-year-old woman with meningocele.
A, Axial CT scan shows a sharply marginated, expansile left petrous apex mass (asterisk).
B, Coronal T1-weighted (350/10/2) MR image shows a cyst of CSF signal intensity extending inferiorly into the petrous apex (arrows).
C, Axial T2-weighted FSE (2800/90/1) MR image confirms that the expansile mass revealed on CT studies is a cyst with CSF signal intensity (asterisk) extending from Meckel's cave into the petrous apex.
Discussion
Petrous apex lesions are uncommon and represent a spectrum of pathologic and incidental entities (1, 2). Traditional diagnoses to consider when a cystic petrous apex lesion is discovered include benign obstructive lesions of air cells (cholesterol granuloma, mucocele), congenital or acquired cholesteatoma, and apical petrositis (6–9). Petrous apex effusion, an incidental “leave-me-alone” lesion must also be considered (2). In this report, we introduce another imaging diagnosis to this list, the PAC.
Several characteristic imaging findings differentiate inflammatory lesions (Fig 2) from PACs (Table 2). A unilateral or bilateral fluid-intensity mass (on MR images) with smooth, noninvasive bony excavation of the petrous apex bone (on CT studies) that originates from the ipsilateral Meckel's cave defines this lesion (Fig 1). PACs arise outside of, and secondarily erode into, the petrous apex from the adjacent Meckel's cave, whereas inflammatory lesions arise from and expand the petrous apex from within. Placing the center of a low T1 signal intensity lesion outside the petrous apex makes a mucocele or cholesteatoma very unlikely. Also, middle ear or mastoid effusions are atypical of PAC unless the patient presents with CSF otorrhea. The distinctive imaging appearance of this petrous apex cystic lesion allows the radiologist to make this diagnosis with a high degree of certainty. Nevertheless, having described this lesion precisely, its pathophysiology still remains unclear.
Differential imaging findings
This lesion has been inconsistently referred to as both a meningocele and an arachnoid cyst (3–5). We chose the more generic term PAC because the lesion is either a congenital or acquired herniation of the posterolateral Meckel's cave margin and contents into the petrous apex, and depending on what the surgeon discovers as the wall of this lesion is traversed, either the term meningocele or arachnoid cyst may be most applicable.
More important than the actual descriptive term is that this lesion is often identified as an asymptomatic incidental finding on brain MR images. Correctly identifying it as a PAC and not a cholesteatoma in such a circumstance avoids unnecessary surgical intervention (3). None of the other cystic lesions of the petrous apex (cholesteatoma, cholesterol granuloma, mucocele, apical petrositis, and petrous apex effusion) arise from Meckel's cave, as PAC does, and this single imaging feature allows PAC to be distinguished from these other entities.
Once the definitive diagnosis of PAC is made, the lesion must be sorted into one of two groups: either a symptomatic lesion, requiring possible surgical intervention, or an asymptomatic and incidental finding, requiring no treatment. Unfortunately, the only published PAC cases currently reside within the clinical literature and were deemed symptomatic enough to require surgery. Conversely, from our case material, the majority of lesions were imaged for reasons clearly unrelated to PAC. Merging these experiences suggests that a careful assessment of each PAC within an objective clinical context is critical to an informed decision to treat this lesion, and in many cases a bias toward watchful waiting is probably prudent.
We recognize three possible limitations to our study. First, we describe a small, highly selected tertiary patient population and do not attempt to statistically evaluate the incidence or prevalence of noninflammatory petrous apex cysts in the general population. Also, we do not have a sufficiently large group to statistically derive sensitivity and specificity for MR imaging and CT in this population. Nevertheless, although our sample size is too small to draw statistical inferences, our data show that the diagnosis of a cystic apex lesion does not necessarily imply that surgical intervention is required. Rather, correct diagnosis of a noninflammatory apex cyst may prevent surgery that is based on the erroneous presumption of an inflammatory lesion. Second, although MR imaging can usually identify herniated brain elements that distinguish a meningoencephalocele from a meningocele, it is difficult to ascertain the presence or absence of a dural lining on MR imaging studies to distinguish between a meningocele and an arachnoid cyst. Compounding this problem is the unfortunately frequent colloquial interchange of the terms meningocele and arachnoid cyst when describing these lesions, although it is probably not clinically important to distinguish between these two entities on imaging studies, because the operative approach in cases requiring surgery is unlikely to be significantly altered. Third, we did not have a diffusion-weighted imaging sequence available at the time of data collection. There may be a future role for diffusion-weighted imaging to distinguish a PAC from an inflammatory lesion when the primary clinical question leading to imaging rests on making this distinction.
Conclusion
PACs are considerably less common than inflammatory cystic apex lesions arising from complications of air cell disease. PACs represent arachnoid cysts and meningoceles arising from Meckel's cave that secondarily erode into the petrous temporal bone. They can usually be differentiated from inflammatory air cell complications that require surgical treatment by careful consideration of the lesion center, osseous margins, and relationship to adjacent structures. Their behavior is more benign than that of inflammatory lesions; unlike inflammatory apex cysts, noninflammatory cysts may not require operative treatment, and a decision to operate should be carefully made on an individual basis. Longitudinal study of these patients, including attention to operative outcome if applicable, will clarify their clinical significance and natural history.
Footnotes
1 Address reprint requests to Kevin R. Moore, MD, Department of Radiology, Section of Neuroradiology, University of Utah School of Medicine, 50 N Medical Dr, 1A–71 SOM, Salt Lake City, UT 84132.
- Received September 27, 2000.
- Accepted after revision June 14, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Rare case of bilateral petrous apex cephalocele
- Pearls & Oy-sters: A rare presentation of chronic intracranial hypertension with concurrent deafness and blindness
- Dilation of the Subarachnoid Spaces Surrounding the Cranial Nerves with Petrous Apex Cephaloceles in Usher Syndrome
- Imaging of the petrous apex: a pictorial review