
Abstract
Summary: We report a case of Whipple disease involving the brain, optic chiasm, posterior fossa, and spinal cord. We evaluate the role of MR imaging for initial evaluation and for long-term follow-up of Whipple disease involving the CNS. We also discuss the semiologic characteristics of the lesions.
Whipple disease is a systemic disorder affecting particularly the small bowel and inducing a malabsorption syndrome (1). Osteoarticular, cardiac, and CNS involvements are also common (1, 2). The responsibility of a gram-positive bacillus, Tropheryma whippelii, has been recently shown (3). The pathogenesis and epidemiology, however, remain obscure. The most common neurologic symptoms include cognitive changes, supranuclear gaze palsy, altered level of consciousness, psychiatric signs, and upper motor neurons signs (4). Postmortem studies (5) have shown that these neurologic symptoms are associated with a granulomatous infiltration of the different levels of the CNS, particularly the brain, chiasm, pituitary gland, pons, and spinal cord. The brain lesions are essentially confined to the gray matter, preferentially the basal part of the telencephalon, the hypothalamus, and the thalamus (6).
However, diagnosis of Whipple disease involving the CNS remains difficult. It is often delayed, particularly if it occurs without digestive signs, because 20% of the patients present with neurologic features alone and no other manifestations of the disease (4, 7–9). In these cases, neuroimaging, and particularly MR imaging, has been able to reveal, in a noninvasive manner, involvement of the CNS (7, 10–12). We report the first case of Whipple disease in which MR imaging revealed lesions affecting the different levels of the CNS simultaneously; namely the chiasm, brain, posterior fossa, and spinal cord.
Case Report
A 68-year-old man was admitted for walking difficulties, memory loss, and incontinence that had been progressing for 5 months. For 12 years, he had complained of arthralgias of the hands and wrists. The diagnosis of rheumatoid polyarthritis had been made.
A neurologic examination revealed a tetrapyramidal syndrome associated with apathy and memory loss. Blood tests indicated an inflammatory syndrome with an elevation of the erythrocyte sedimentation rate (80 mm at the first hour) and an increase of proteins. The results of antinuclear antibody, HIV, B and C hepatitis, latex, and Waler Rose tests were negative. The CSF test showed an increase in the protein rate (1.95 g/L) with an absolute increase of immunoglobulin G (205 mg/L), but the cell count and glucose level were normal. Polymerase chain reaction for Tropheryma whippelii was negative.
MR images of the brain (Fig 1A–D and F) had areas of T2 hyperintensity in the right and left mediobasal temporal lobe, anterior commissure, right and left mamillary bodies, left cerebral peduncle, right middle cerebellar peduncle, bulb, right lobe of the cerebellum, and optic chiasm. These lesions showed no mass effect. After IV infusion of a contrast agent, mild enhancement of the right temporal lesion could be seen. MR imaging of the spinal cord was also performed, showing T2 panmedullary central hyperintensity.

Images from the case of a 68-year-old man who was admitted for walking difficulties, memory loss, and incontinence that had been progressing for 5 months.
A, Axial T2-weighted MR image (4347/100/4) of the brain shows hyperintensity in the mediobasal part of the right and left temporal lobes (arrows), in the mamillary bodies (star), and in the optic chiasm (arrowhead).
B, Axial T2-weighted fluid-attenuated inversion recovery MR image (11000/140/2 [TR/TE/excitaitons]) of the brain shows diffuse hyperintensity involving the right mediobasal and left mediotemporal lobes (arrows), as well as involvement of the left cerebral peduncle (arrowhead). Note the lack of mass effect despite the size of the lesion.
C, Coronal fluid-attenuated inversion recovery MR image (11000/140/2) of the brain shows hyperintensity in the mediobasal part of right and left temporal lobes (arrows), brain stem (star), and right middle cerebellar peduncle (arrowhead).
D, Coronal T1-weighted MR image (535/14/2) of the brain shows mild enhancement of the right temporal lesions after the IV administration of a contrast agent (arrow).
E, Sagittal T2-weighted MR image (2745/120/6) of the spine shows hyperintensity in the central part of the spinal cord (arrow).
F, Coronal T2- weighted fluid-attenuated inversion recovery MR image (11000/140/2) of the brain, obtained after 1 year of treatment, shows nearly complete resolution of the right temporal lesion (arrow).
The patient underwent a duodenal biopsy, which showed macrophages that stained positively with periodic acid-Schiff stain (Fig 2). Polymerase chain reaction for Tropheryma whippelii was positive on the duodenal biopsy.
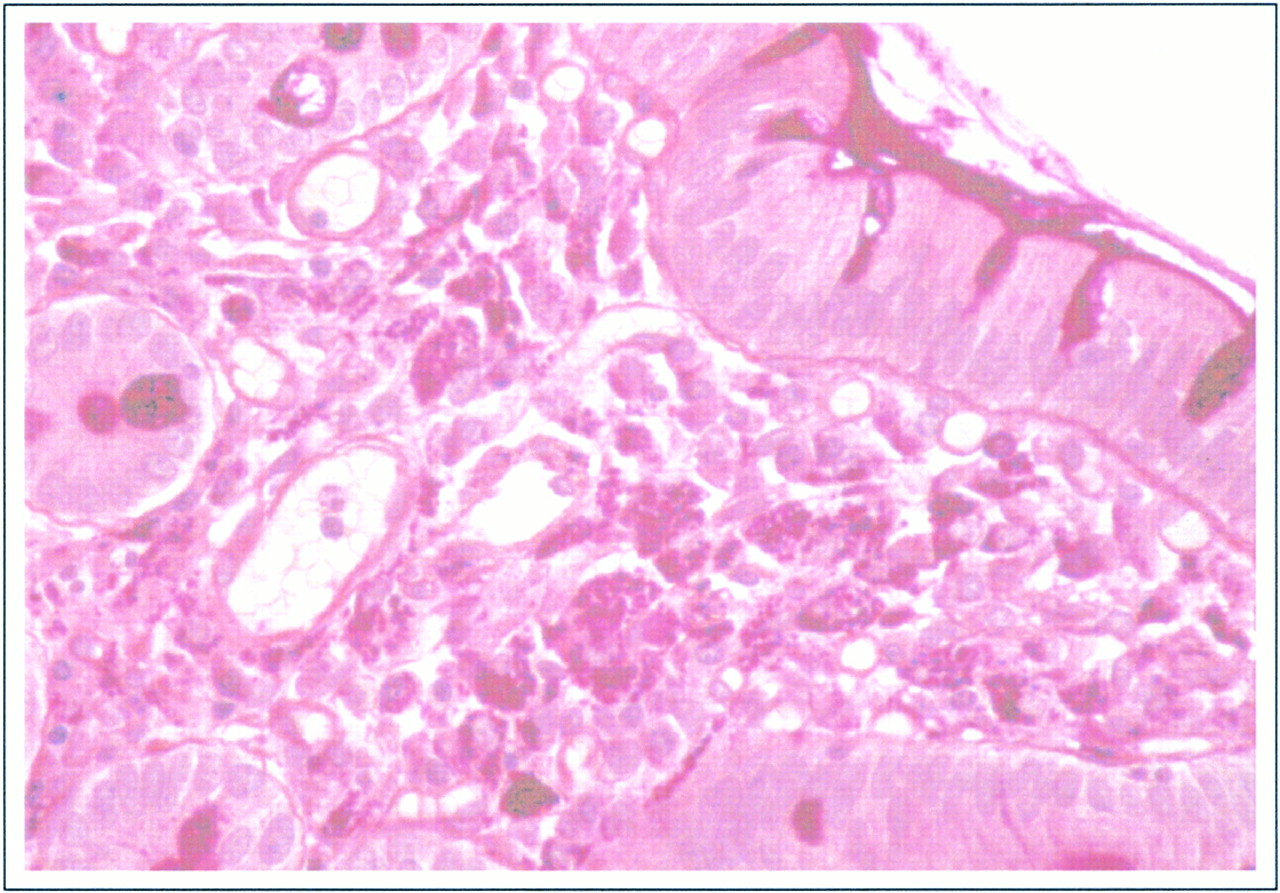
Duodenal biopsy was performed. Note the characteristic foamy macrophages containing periodic acid-Schiff stain-positive rod-shaped structures in the submucosal region
The patient was treated for 2 weeks with the IV administration of amoxicillin and amikacin sulfate and then with continuous orally administered sulfamethoxazole-trimethoprim. One year later, the neurologic abnormalities had improved, with nearly complete resolution of the tetrapyramidal syndrome and complete resolution of the cognitive disorders. This clinical improvement correlated with MR investigations that showed nearly complete regression of the right temporal lesion (Fig 1F). Complete resolution of the posterior fossa, optic chiasm, and spinal cord lesions was shown. Moderate cerebral and optic chiasm atrophy remained.
Discussion
A review of 84 cases described in the literature (4) revealed that clinically detectable involvement of the CNS ranges from 6% to 43% of patients suffering from Whipple disease. In 43 of the 84 reported cases, CT or MR imaging of the head was performed, and in 23, focal abnormalities were found (4).
However, Dobbins (1) postulates that all patients suffering from Whipple disease have anatomic-pathologic CNS involvement (13). It consists of multiple small circular or oval lesions, measuring an average of 2 mm in diameter, disseminated throughout the gray matter and characterized by the accumulation of macrophages, staining very intensely with periodic acid-Schiff stain, as shown in postmortem studies (6). Electron microscopy shows that the macrophages contain a bacilliform organism, named Tropheryma whippelii by Relman et al (3), revealing the bacterial cause of the disease (2, 6). The same lesions are found in other organs when they are affected by the disease (2, 6). Recently, molecular biology allowed the detection of the presence of Tropheryma whippelii in the affected organs by using polymerase chain reaction (3). Previous studies have shown a good correlation between preferential sites of anatomic-pathologic lesions and the lesions revealed by MR imaging and CT (5, 8, 9, 14).
The first neuroradiologic descriptions of CNS involvement were reported as seen on CT scans (8, 14), and they presented no specific characteristics (2). The CT scan can be normal, regardless of the clinical features, or can reveal focalized lesions, which can be hypo- or hyperdense, contrast enhanced or not, and with or without mass effect (2). However, MR imaging has proved its superiority for the detection of small lesions (3). In a review of the literature presented by Louis et al (4), 43 patients had undergone CT or MR imaging and three patients with normal CT findings had focal abnormalities on their MR images (4).
These lesions, which occur in 53% of the cases (4), often consist of T1 hypointensity and T2 hyperintensity, show no mass effect, and are located in the medial part of the temporal lobes, in the hypothalamic region, or in the pons (9, 10). These lesions are sometimes enhanced after infusion of contrast media (4, 8, 9, 14). Moreover, associated moderate atrophy occurs in 42% of the cases (4).
Multiple mass lesions have rarely been described. They usually appear hypointense on T1-weighted images and hyperintense on T2-weighted images and enhance after infusion of contrast media (12). However, a small number of patients have normal-appearing MR images (4).
The involvement of the spinal cord has rarely been reported. We found only one report of myelopathy secondary to Whipple disease, diagnosed by using MR imaging (11). It was located in the cervical region, and it appeared hyperintense on T2-weighted images after IV injection of gadolinium.
Involvement of the optic chiasm has also rarely been revealed by neuroradiologic examination, although it is more often discovered during postmortem studies (9). We found only one report with an increased T2 signal intensity located in the optic tracts (9). However, clinical optical manifestations are common in cases of Whipple disease (4, 5).
Early treatment of Whipple disease leads to improvement of the lesions revealed by neuroradiologic examination (4, 9, 12), as shown in our case, but diagnosis is often difficult. Diagnosis is often difficult to determine on the basis of polymerase chain reaction or histologic findings (98%); more precisely, 63% of patients underwent biopsy (88% of which were obtained from the small bowel (4). More rarely, the diagnosis is made based on lymph node biopsy or cerebral biopsy. However, polymerase chain reaction has shown sensitivity and specificity to confirm a diagnosis of Whipple disease (15), and recent studies have revealed genetic material of Tropheryma whippelii in peripheral blood mononuclear cells and in cells of pleural effusion (16), suggesting that the diagnosis can sometimes be made on the basis of polymerase chain reaction of peripheral blood (17). The diagnosis can also be obtained by conducting an analysis of the CSF for periodic acid-Schiff stain-positive cells (2), but the value of polymerase chain reaction in CSF has not yet been evaluated because of the rarity of the disease.
Treatment is often delayed, however, resulting in death or irreversible cerebral lesions, such as atrophy (9, 13). Moreover, relapse of the disease is frequent, leading to the reappearance of the CNS lesions on MR images (4).
In conclusion, this case report shows the importance of neuroradiologic examinations, particularly MR imaging, for the detection of CNS lesions in the initial evaluation of patients suspected of having Whipple disease and for the long-term follow-up of these patients. It is necessary to perform MR imaging of the brain and spinal cord to ascertain the different locations of these lesions.
Footnotes
↵1 Address reprint requests to Dr. Sylvie Grand, Magnetic Resonance Imaging Unit, Centre Hospitalier et Universitaire de Grenoble, Hôpital Michallon, 38043 Grenoble Cedex 09, France.
References
- Received March 7, 2000.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}