
Abstract
Summary: A new CT perfusion technique providing extended anatomic coverage was evaluated in 12 patients with suspected acute middle cerebral artery ischemia. With a multidetector CT scanner, scans were obtained in an alternating fashion at two distinct “toggling” table positions (two 1-cm sections each) during a 40-mL contrast agent bolus (approximately 5 seconds per image), and perfusion parameter maps were created. The CT perfusion results were compared with follow-up images.
Nine patients showed focal perfusion abnormalities in at least one section, most commonly on mean transit time maps. Using a single table location would have underestimated or missed the involved tissue in most cases. In three of 12 patients, perfusion maps failed to delineate any abnormality. In two patients, perfusion and diffusion MR imaging confirmed the absence of perfusion abnormality and tissue injury, respectively. In one case, a small ischemic injury was revealed by diffusion MR imaging.
By using the toggling-table approach, perfusion images can be obtained over an extended anatomic area and, thus, reveal the presence and the extent of presumed tissue injury.
Perfusion- and diffusion-weighted MR imaging is a valuable tool for the assessment of suspected stroke (1), but it has limitations for severely ill patients or might not be available in an emergency. In the current era of thrombolytic therapy, rapid identification of the presence and extent of ischemia is essential (2, 3). Given its widespread availability and tolerability, research has been redirected toward CT to obtain physiological information about ischemic tissue. In particular, dynamic CT perfusion techniques have been advocated, yielding perfusion information comparable to that provided from MR images (4–11). One disadvantage of the CT perfusion techniques is the limited anatomic coverage of single-section data acquisition. Even multidetector scanners do not fully address this issue; anatomic coverage is still limited to 2 cm (using the Lightspeed scanner; General Electric Medical Systems, Milwaukee, WI). Among patients with suspected acute ischemic stroke, the noncontrast CT scans might be normal, and a single-location perfusion scan has been shown to miss a pathologic area (10).
We implemented a technique to expand the anatomic coverage of CT perfusion acquisition, by toggling the table between two locations during dynamic scanning. Although this compromises temporal resolution somewhat, useful and predictive perfusion parameters can, nevertheless, be derived.
Description of the Technique
Data acquisition was performed with a multidetector CT scanner (Lightspeed; General Electric Medical Systems, Milwaukee, WI).
After a noncontrast CT scan of the whole brain, the dynamic CT perfusion series was performed (field of view, 25 cm; 120 kV; 30–60 mA; matrix, 512 × 512; injection, 40 mL nonionic contrast agent with a flow rate of 3–4 mL/s; delay, 9 seconds; data acquisition, 40–60 seconds). Two locations with two sections each (all 1 cm thick) were scanned in an alternating fashion with “toggling-table” movement. The whole dynamics of a contrast agent transit curve can be observed in two distinct, 2-cm–thick locations representing the middle cerebral artery (MCA) territory. The locations were typically chosen first at the level of the insula/basal ganglia and third ventricle, then through the centrum semiovale and deep white matter. Temporal resolution occurred in approximately 5 seconds. (Note: according to our own experience, two sections with 1-cm thickness in each location are more practical for data analysis; however, in a similar fashion, four sections with 0.5-mm thickness might be chosen at each location, leading to a total of eight sections.)
The CT perfusion images were analyzed off-line on a Sun Ultra 1 Workstation (Sun Microsystems; Palo Alto, CA) using the MRVision software package (The MRVision Company, Wakefield, MA). From the obtained density values, the following perfusion parameter maps were calculated on a pixel-by-pixel basis from the four sections at the two distinct locations: peak density change (peak), time to peak (TTP), the relative cerebral blood volume (rCBV) computed from the integral under the contrast agent transit curve, the mean transit time (MTT) estimated from the full width of the contrast agent transit curve at half height, and the relative cerebral blood flow (rCBF) calculated as the ratio of rCBV and MTT, according to the central volume theorem.
Patients and Methods
Twelve patients with suspected acute cerebral ischemia in the MCA territory were included. In all patients, the CT study was performed within 6 hours of symptom onset. The CT perfusion parameter maps were compared with noncontrast follow-up CT scans (at least 3 days after the acute event, n = 7) or MR perfusion and diffusion images (acquired between 1 and 4 days after the CT perfusion study, n = 5).
Discussion
The CT perfusion technique with toggling-table movement yields four distinct imaging sections (each 1 cm thick), covering the presumed ischemic area in the MCA territory. Using multidetector CT scanners, two distinct locations (each 2 cm thick, separated into 1-cm–thick sections) can be scanned, with an effective section-to-section temporal resolution of approximately 5 seconds. A similar approach can be pursued with helical scanners. The anatomic coverage then would consist of two distinct locations/sections, each 1 cm thick, but that still could represent two separate areas of the MCA territory.
In nine of 12 patients, perfusion CT revealed focal, territorial abnormalities, and in all of these patients the presence of focal cerebral ischemia was confirmed with CT or MR images. In agreement with the literature (12), perfusion abnormalities were notable most commonly in MTT maps (eight of nine cases), followed by peak and rCBF maps (seven cases each). The rCBV and TTP maps were pathologic in only six and five cases, respectively. The low number of rCBV pathologic abnormalities is not surprising; during acute stroke, rCBV is influenced by the severity of hypoperfusion and by collateral flow and compensatory autoregulation, and thus can be either increased, normal, or decreased (13). The low number of pathologic TTP maps might be explained by the low temporal resolution. In all but one case (patient 1), where injury related to spontaneous hemorrhage 3 days after the initial event, the delineated area of perfusion abnormality was a good predictor of the ultimate infarct.
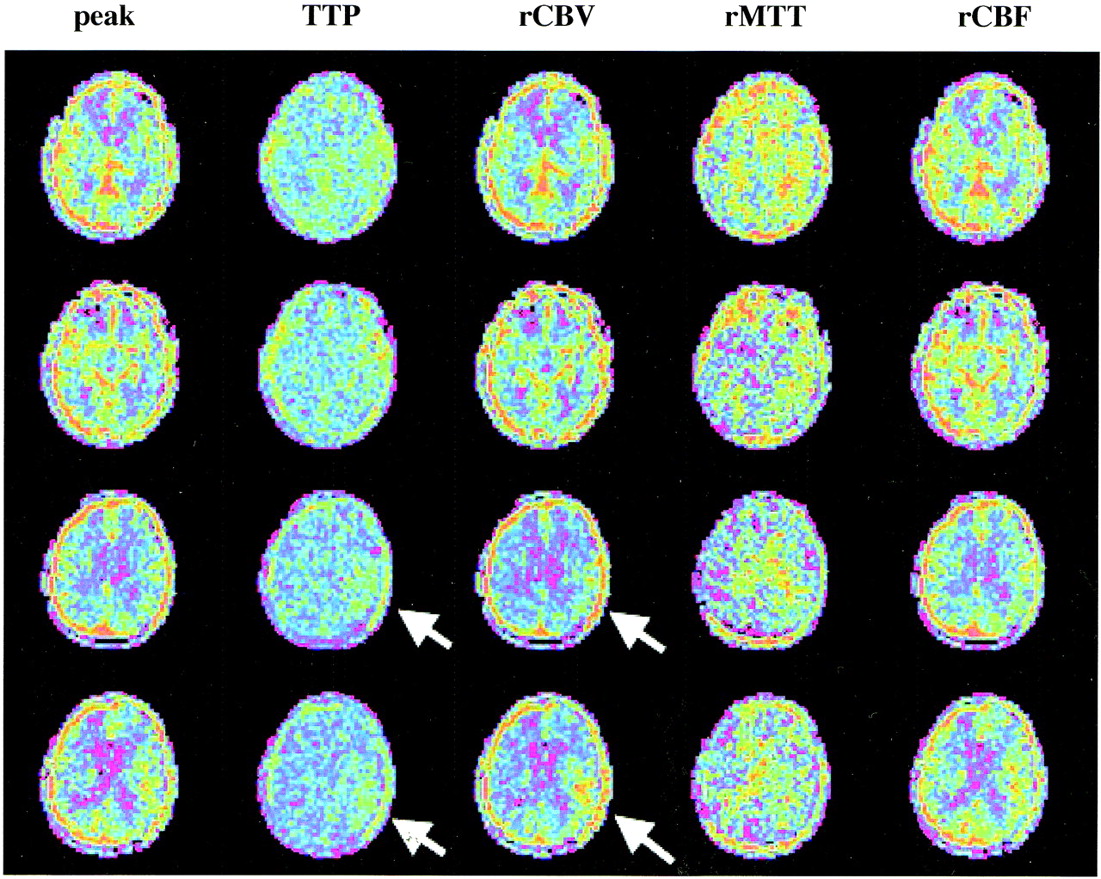
In two of nine cases with positive CT perfusion results, perfusion abnormalities were visible only in one of four sections, in two cases in two sections, in two cases in three sections, and in three cases in all four sections. In other words, using a single table position may not have detected areas of ischemia detected using two table positions (Fig 1).
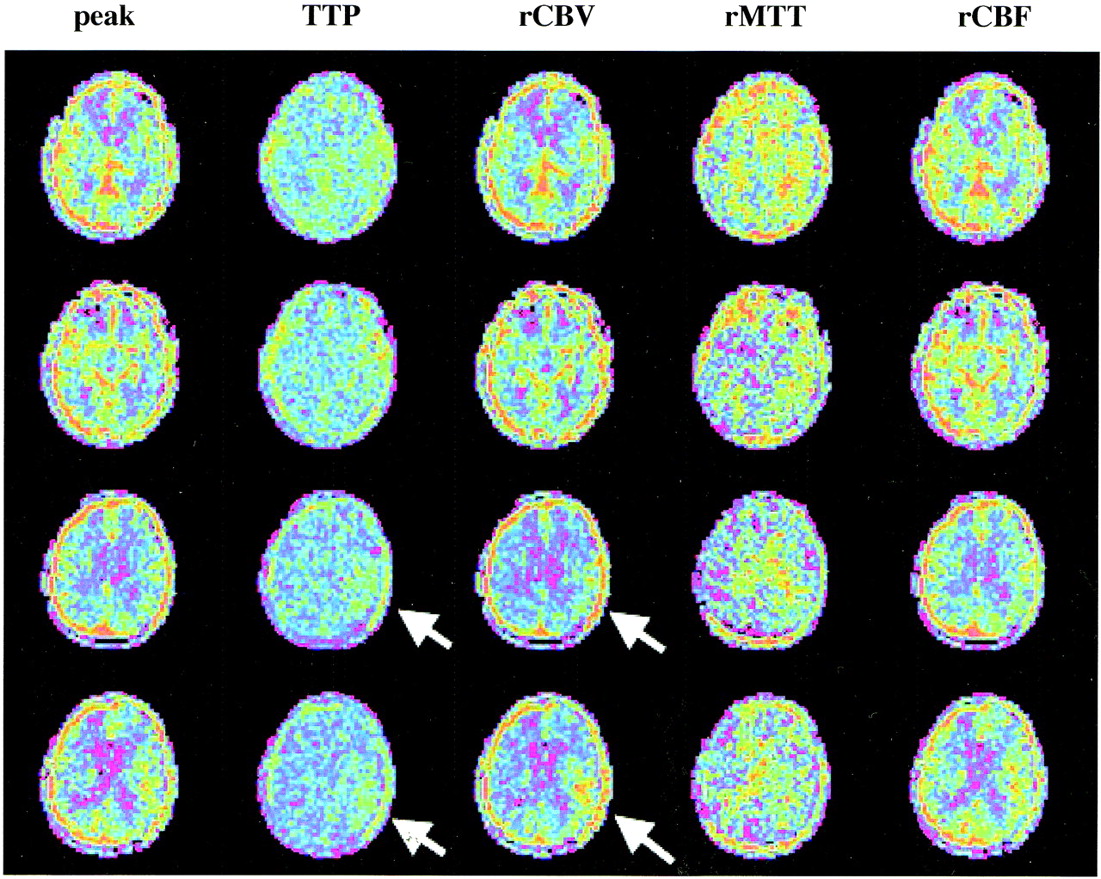
The CT perfusion maps of a patient with an acute onset of a right-sided weakness (patient 2 in the Table). Noncontrast CT scan was negative for acute infarct signs. The infarcted area is covered only on the most superior location (sections 3 and 4) of the four sections from the toggling-table technique (arrows) and would have been missed if a single section location (eg, at the level of the third ventricle) would have been chosen
In eight of nine patients with positive CT perfusion findings, ischemic changes were territorial and caused by a major branch occlusion. In one patient, the perfusion abnormality was caused by an angular branch occlusion, which was confirmed by diffusion-weighted MR imaging.
In three of 12 patients, CT perfusion maps failed to delineate any abnormality. In two cases, the absence of a perfusion abnormality was confirmed by MR perfusion imaging, and the absence of tissue injury was confirmed on diffusion-weighted MR image. In one case, however, diffusion MR imaging delineated an injury that was confined to a small angular branch and not visible on CT perfusion maps.
The presented preliminary data on 12 patients show only one false-negative result in a patient who demonstrated an angular branch occlusion on diffusion-weighted MR imaging (Table). Confirmed territorial infarcts, caused by major branch occlusions of the MCA, were detected in all cases. Within this limited series of patients, there was no false-positive result.
Summary of the CT perfusion findings of the 12 patients
There have been other approaches in the literature to circumvent the limited anatomic coverage of a single-section CT perfusion technique. One approach is to use subtraction images of nonenhanced and contrast-enhanced spiral or helical images of the whole brain, which then indicate the perfused area of the cerebral tissue (4). Normalization to Hounsfield unit changes in a reference blood vessel allows interpretation of such subtraction images as maps of fractional, or perfused, blood volume, and possible delineation of the acute infarct as reduction in rCBV. Information is then limited to this perfusion parameter only, which is less sensitive for the delineation of acute ischemia than, for example, MTT maps (see above). Another approach is to scan several (maximum, three) distinct sections consecutively with high temporal resolution (11), with the number of scanned sections depending on the result of the perfusion parameter maps of the previously scanned location. This, however, not only requires time-consuming data postprocessing and analysis to make the decision whether to scan the next section, but also increases the amount of injected contrast agent, and thus possibly precludes a successive CT angiography acquisition.
In summary, the proposed toggling-table technique is a useful method to expand the anatomic coverage of CT dynamic perfusion. This may help confirm or exclude the diagnosis of an acute ischemic event in a significant volume of the cerebral hemisphere. It is easily performed and is sufficient for the calculation of relative perfusion maps. These first results demonstrate a reliable diagnosis of cerebral ischemia most prominently in the MTT maps. Ongoing studies in a larger patient population are underway to provide numbers for specificity and sensitivity.
Footnotes
1 Address reprint requests to Heidi C. Roberts, M.D., Department of Radiology, University of California, San Francisco, San Francisco, CA 94143.
References
- Received July 17, 2000.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- 4D-CTA in Neurovascular Disease: A Review
- Contribution and Additional Impact of Imaging to the SPAN-100 Score
- The evaluation of haemodynamics in cirrhotic patients with spectral CT
- Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association
- Dose Exposure of Patients Undergoing Comprehensive Stroke Imaging by Multidetector-Row CT: Comparison of 320-Detector Row and 64-Detector Row CT Scanners
- Emerging impact of CTA/perfusion CT on acute stroke thrombolysis in a community hospital
- Recommendations for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association
- 320-slice CT neuroimaging: initial clinical experience and image quality evaluation
- Theoretic Basis and Technical Implementations of CT Perfusion in Acute Ischemic Stroke, Part 2: Technical Implementations
- Identification of Penumbra and Infarct in Acute Ischemic Stroke Using Computed Tomography Perfusion-Derived Blood Flow and Blood Volume Measurements
- Evaluation of carotid stenosis using CT angiography in the initial evaluation of stroke and TIA
- Perfusion CT for the assessment of tumour vascularity: which protocol?
- Trial Design and Reporting Standards for Intra-Arterial Cerebral Thrombolysis for Acute Ischemic Stroke
- Guidelines and Recommendations for Perfusion Imaging in Cerebral Ischemia: A Scientific Statement for Healthcare Professionals by the Writing Group on Perfusion Imaging, From the Council on Cardiovascular Radiology of the American Heart Association
- Perfusion CT: a worthwhile enhancement?
- Safety and Feasibility of a CT Protocol for Acute Stroke: Combined CT, CT Angiography, and CT Perfusion Imaging in 53 Consecutive Patients