
Abstract
Summary: Anthrax meningoencephalitis is a rare complication of infection with Bacillus anthracis and generally produces a hemorrhagic meningoencephalitis. We present the CT and MR imaging findings in two patients demonstrating subarachnoid, intracerebral, and intraventricular hemorrhage with leptomeningeal enhancement.
Infection with the Bacillus anthracis, a large gram-positive, spore-forming bacillus transmitted to humans by contact with infected animals or contaminated animal products, is rare (1). The incidence of meningoencephalitis as a complication of this disease is even rarer and is usually caused by lack of immunization and poor industrial hygiene (2). Brain CT findings are described in a single prior report (2), however; MR imaging findings have not been previously reported. We present the CT and MR imaging findings of two cases of anthrax meningoencephalitis. The two patients, along with 30 or more people, cooked or ingested beef several days prior to the onset of clinical symptoms.
Case Histories
Case 1
A 53-year-old man was admitted to our hospital with fever and bullous lesions on the left forearm. Ten days prior to admission, he was among thirty or more farmers who cooked and ate beef together. Four days later, several papular lesions appeared on his left forearm. On the fifth day post ingestion, the papular lesions increased in size, became vesicular, and ruptured. His left forearm was swollen and fever ensued. At admission, his temperature was 39.2°C, respiration rate was 24, hemoglobin was 9.79 g/dL, white blood cell count was 8,800/mm3, erythrocyte sedimentation rate was 4 mm/h, and fibrinogen was 2.16. He had no history of hypertension, diabetes mellitus, tuberculosis, or hepatitis. Skin biopsy, culture, and smear and blood culture were performed. Several hours later, he became stuporous. A precontrast head CT scan (Fig 1A) revealed multiple hyperdensities at the interhemispheric and sylvian fissures and obliteration of the basal cisterns. A contrast-enhanced CT scan (Fig 1B) revealed prominent supratentorial leptomeningeal enhancement. The patient became comatose, developed respiratory arrest, and required ventilatory support. On the second day following admission, MR imaging of the brain was performed with spin-echo T1-weighted, T2-weighted, fluid-attenuated inversion recovery (FLAIR), and gradient-echo images and contrast-enhanced T1-weighted images on a 1.5-T system. Multiple areas of obliteration of the supra- and infratentorial subarachnoid spaces were revealed on T1-weighted images. Multiple hypointense areas were present in the subarachnoid spaces, especially infratentorially, on gradient-echo images (Fig 1C–D). Compared with the signal intensity of CSF, subarachnoid lesions were isointense on T1- and slightly hypointense on T2-weighted spin-echo images. On FLAIR images, these lesions were slightly hyperintense to CSF. On contrast-enhanced T1-weighted images (Fig 1E), diffuse leptomeningeal enhancement was revealed. Gram-positive bacillus was found on the skin biopsy specimen and smear. In spite of intravenous penicillin injection and supportive therapy, the patient died on the sixth day following admission. One week later, Bacillus antracis was confirmed on blood and tissue cultures.

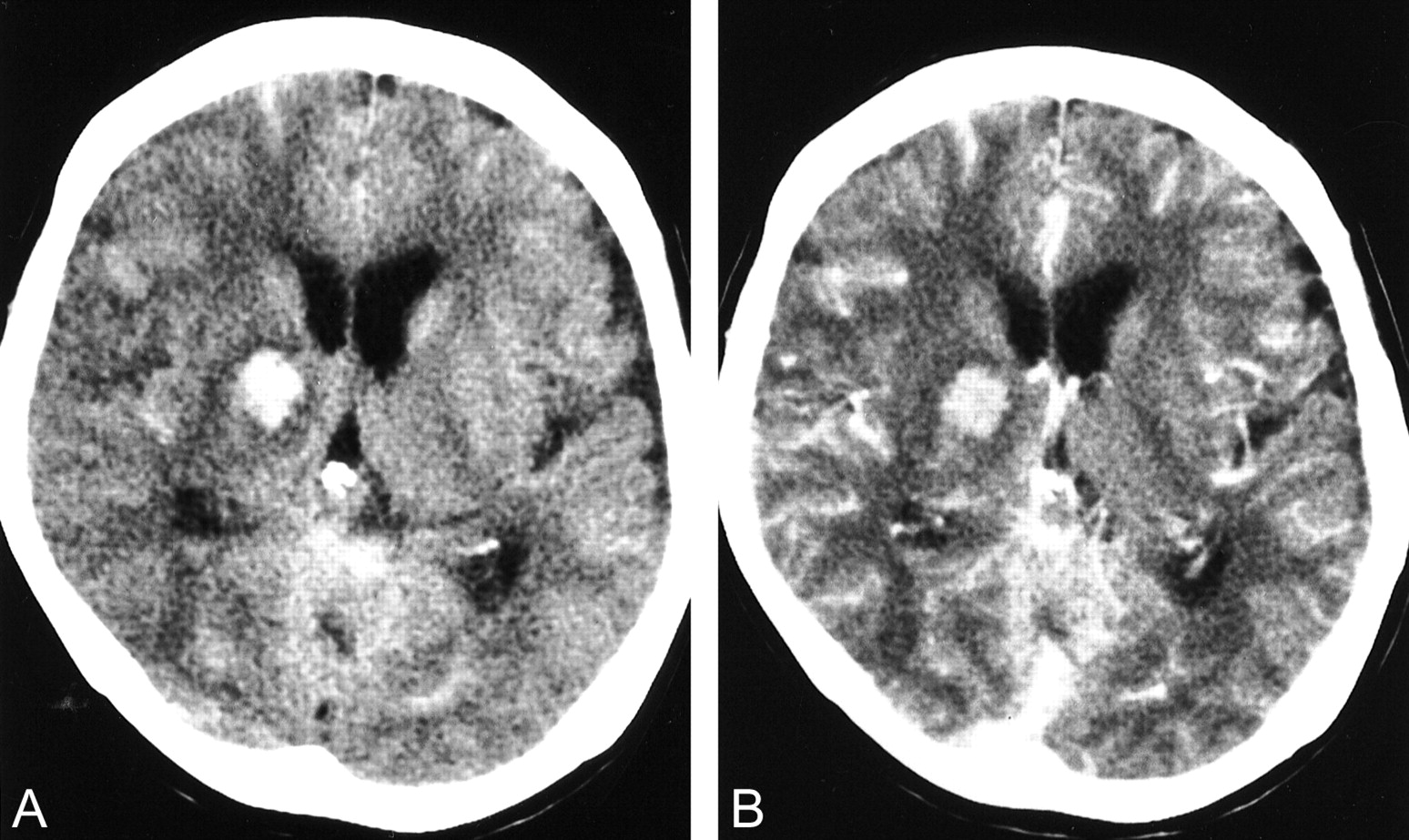
Case 1, a 53-year-old man with anthrax meningoencephalitis.
A and B, Precontrast (A) and contrast-enhanced (B) axial CT scans show diffuse subarachnoid hemorrhage and leptomeningeal enhancement. Mild ventriculomegaly is also seen.
C and D, Axial T2-weighted gradient-echo MR images (703/15 [TR/TE]) show diffuse dark signal intensities suggesting hemorrhage within the supra- and infratentorial subarachnoid spaces.
E, Contrast-enhanced axial T1-weighted MR image (513/12) shows diffuse leptomeningeal enhancement.
Case 2
A 72-year-old woman was admitted to the emergency room (of the hospital of N.M.H.) 2 days earlier than the above-described patient. She was semicomatose at admission, and it became known that she was a friend of the previously described patient and that they had cooked and ingested the beef together. On the third day post ingestion, she developed dark vesicles on her left hand. At admission, her temperature was 36°C, respiration rate was 26, blood pressure was 80/50 mm Hg, and pulse was 154. She had hyperactive knee and ankle jerks, a positive Babinski sign, and decreased power in the left leg. Hemoglobin was 11.3 g/dL, white blood cells were 27,700/mm3, platelet was 88,000/μL, prothrombin time/partial thromboplastin time were 16.2/85.5 s, serum aspartate aminotransferase/alanine aminotransferase were 67/12, blood urea nitrogen/creatinine were 33.8/1.9. She had no history of hypertension, diabetes mellitus, tuberculosis, or hepatitis. Blood culture was performed. A precontrast head CT scan (Fig 2A) revealed multiple hyperdensities at several areas along the subarachnoid spaces, right basal ganglia, thalamus, internal capsule, and right lateral ventricle, suggesting subarachnoid, intracerebral, and intraventricular hemorrhage. Contrast-enhanced CT scan (Fig 2B) revealed diffuse leptomeningeal enhancement. She died of respiratory failure on the second day following admission. One week later, blood culture confirmed Bacillus anthracis.
Case 2, a 72-year-old woman with anthrax meningoencephalitis.
A, Precontrast axial CT scan shows hemorrhage at the right deep gray matter, both lateral ventricles, and cortical sulci.
B, Contrast-enhanced axial CT scan shows diffuse leptomeningeal enhancement.
Discussion
Pathogenic Bacillus anthracis endospores that reach a primary site in the skin, gastrointestinal mucosa, or alveolar spaces are phagocytosed by macrophages and migrate to the regional lymph nodes. Endospores germinate within the macrophages and become vegetative bacteria, which are released from the macrophages. Endospores multiply in the lymphatic system, enter the bloodstream, and increase to high numbers, causing severe septicemia. High levels of exotoxins are produced that lead to the death of the host (3, 4). Anthrax meningoencephalitis is a rare form of anthrax infection, caused by dissemination of the organism to the CNS, which may occur via hematogenous or lymphatic routes (3, 5). In addition to meningeal signs, clinical features include nausea and vomiting, myalgia, chills, dizziness, and occasionally a petechial rash. Progressive neurologic deterioration, convulsions, and coma usually occur within 2 to 4 days. Fatality rates are high for all forms of systemic anthrax infection (5).
Anthrax meningoencephalitis is described as a hemorrhagic alteration in the brain and meninges, as characterized by the two cases reported herein. Autopsy was not performed in the present two cases. Postmortem examination of the anthrax meningoencephalitis revealed hemorrhage over the surface of the cerebral hemisphere and in the subarachnoid space, and congestion of the white and gray matter (6).
The first description of the CT findings of anthrax meningoencephalitis showed multiple hemorrhagic lesions at the gray-white matter junction of the cerebrum and diffuse meningeal enhancement (2). On CT and MR images, hemorrhage at the deep gray matter, ventricle, supra-, and infratentorial subarachnoid spaces and diffuse meningeal enhancement were revealed. However, no parenchymal enhancement was found in our patients nor reported in the prior literature. Low signal intensity on spin- and gradient-echo T2-weighted images of case 1 represented acute hematoma or the state of deoxy-hemoglobin of the hematoma. This is correlated with the time of clinical onset of CNS symptoms.
The differential diagnosis of anthrax meningoencephalitis includes subarachnoid or intracerebral hemorrhage, bacterial or aseptic meningitis, and encephalitis. MR imaging with contrast medium can easily distinguish hemorrhagic meningoencephalitis from subarachnoid or intracerebral hemorrhage. The hemorrhagic encephalitis can be seen in herpes simplex virus type I encephalitis (7) and varicella zoster, rubellar, and amoeba infection in immunocompromised patients (8–10). To differentiate other hemorrhagic or nonhemorrhagic meningoencephalitis, Gram's staining and culture of CSF should be performed (1, 6).
Another three patients who cooked or ate the same beef at the same location as the two patients reported here had cutaneous infection, but they were all cured. Cutaneous infection, the most common form of the disease, begins with a small, somewhat pruritic papule at the site of an abrasion, which over the next several days develops into a vesicle containing serosanguineous fluid teeming with organisms. As the lesion progresses, ulceration occurs, with formation of a necrotic ulcer base frequently surrounded by smaller vesicles. The characteristic black eschar evolves over several weeks. This black eschar accounts for the name anthrax, which comes from the Greek word for coal (1).
In summary, this case report describes hemorrhagic meningoencephalitis clearly demonstrable on CT and MR images in antracis infection. The site of hemorrhage was the subarachnoid space, deep gray matter, and ventricle. Diffuse leptomeningeal enhancement was prominent.
Footnotes
1 Address reprint requests to Hak Jin Kim, Department of Radiology, Pusan National University Hospital, 10, 1-Ga, Ami-Dong, Seo-Ku, Pusan, 602-739, South Korea.
References
- Received January 25, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Neuroinfectiology of an atypical anthrax-causing pathogen in wild chimpanzees
- Leptomeningeal Enhancement in Multiple Sclerosis and Other Neurological Diseases: A Systematic Review and Meta-Analysis
- Armies of Pestilence: CNS Infections as Potential Weapons of Mass Destruction
- Anthrax meningoencephalitis