
Abstract
Summary: Intraosseous hemangiomas are uncommon, constituting less than 1% of all osseous tumors. The most frequent sites are the calvaria and the vertebral column. Involvement of the facial bones is rare, and occurs most commonly in the maxilla, mandible, and nasal bones. Only 20 cases of zygomatic involvement have been reported in the English-language literature. We report a case of an intraosseous hemangioma of the zygoma documented by CT and MR studies.
Intraosseous hemangiomas of the zygoma are rare. The diagnosis in our case was suggested by the CT and MR imaging characteristics. Preoperative awareness of the vascular nature of this lesion is crucial, as routine bone biopsy and curettage may lead to significant hemorrhage. For this reason, we also obtained an angiogram.
Case Report
A 31-year-old woman presented with a 3-month history of progressive dystopia and a 1-year history of painless swelling of the left cheek. She denied any prior trauma. Physical examination was significant for a hard, immobile mass of the malar eminence. A contrast-enhanced CT study of the paranasal sinuses showed a 2.5-cm expansile, rounded, well-defined bony lesion in the left zygoma (Fig 1A–C). Posteriorly, the lesion tapered into the anterior zygomatic arch. There was no associated soft tissue mass, either in the overlying soft tissues of the cheek or in the infratemporal fossa. The lesion had an overall spokewheel appearance formed by radiating fine trabeculae, and the inner and outer cortices were intact but thinned. A residual “ghost” of the cortex was seen, which argued for a benign lesion, as a destructive process would not respect the original cortex. There was no periosteal reaction. The mass impressed on the inferolateral aspect of the orbit, resulting in slight upward and medial displacement of the globe. The preliminary diagnosis, based on the CT appearance, was intraosseous hemangioma of the zygoma.
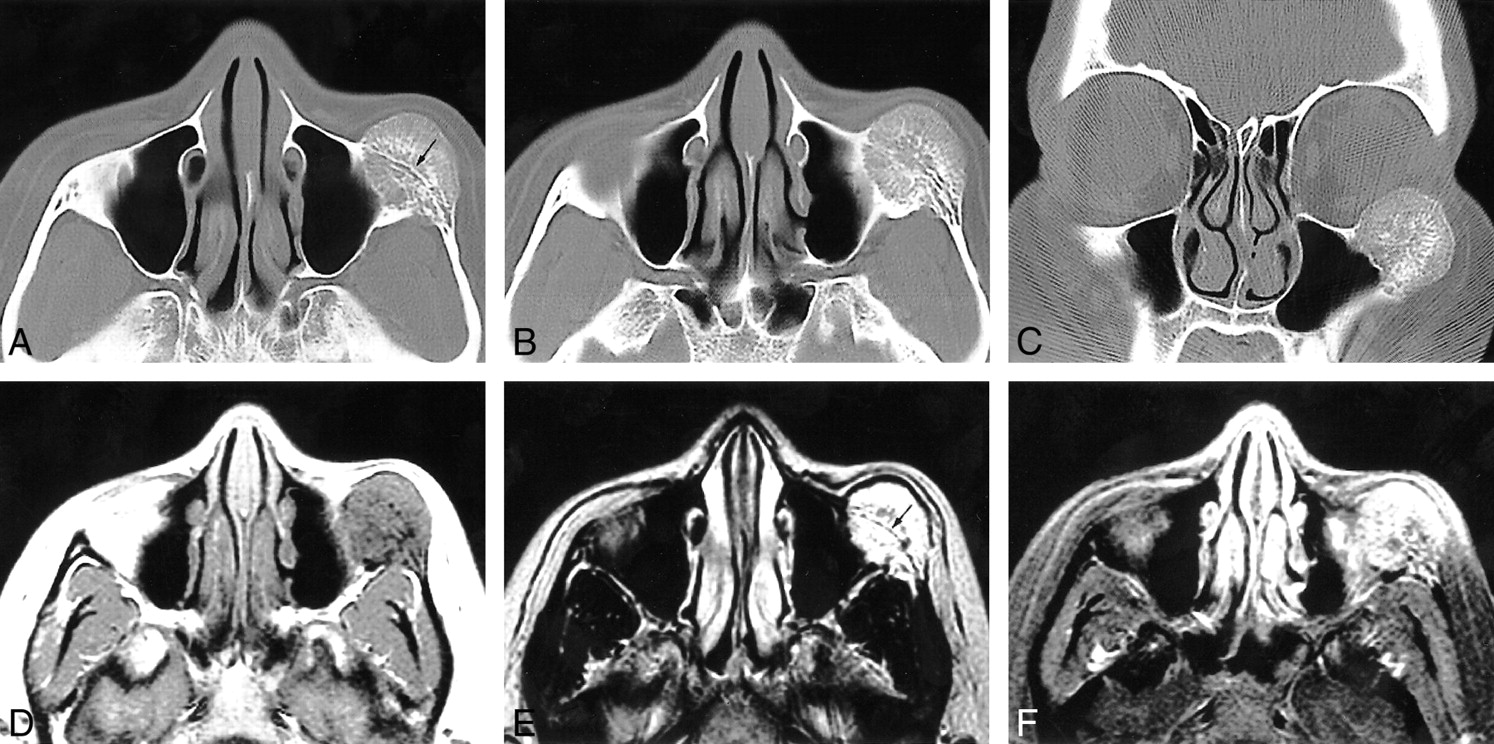
31-year-old woman with a 3-month history of progressive dystopia and a 1-year history of painless swelling of the left cheek.
A–C, Axial caudal (A), cranial (B), and coronal (C) CT scans, viewed at wide window settings.
A, A 2.5-cm round lesion arises from the zygoma. The inner and outer cortices, although thinned, are preserved. The trabeculae radiate in a spokewheel-type pattern, and a residual trace of the original cortex is seen (arrow).
B, The trabeculae of the lesion taper into the zygomatic arch. There is no associated soft tissue mass.
C, The rounded lesion encroaches on the inferolateral orbit.
D–F, Axial T1-weighted (500/9/2) (D), T2-weighted (3600/95/2) (E), and contrast-enhanced, fat-suppressed T1-weighted (450/9/2) (F) MR images.
D, The lesion is isointense with muscle and shows fine radiating lines of high signal intensity that are interspersed with the trabecular signal voids.
E, Encroachment on the inferolateral aspect of the orbit is seen. No extraosseous mass is evident. A line of signal representing the original cortex is visible (arrow).
F, The mass enhances; no large regional vessels are evident.
MR imaging of the paranasal sinuses confirmed the CT localization of the lesion (Fig 1D–F). The mass had an overall intermediate T1 signal intensity and a high T2 signal intensity. Within the mass were areas of signal void that corresponded to the trabeculae seen on the CT study. There was marked enhancement after intravenous administration of 15 mL of gadopentetate dimeglumine. No extraosseous soft tissue component was apparent.
Based on the imaging diagnosis, a decortication incisional biopsy of the lesion was performed, which precipitated moderate bleeding that was controlled with bone wax. The diagnosis of this tissue was consistent with hemangioma.
A carotid arteriogram showed a hypervascular lesion in the left zygoma, and a delayed persistent blush with a “cluster of grapes” appearance. The lesion was supplied predominantly by the left external carotid artery via the infraorbital and posterosuperior alveolar arteries, the anterior deep temporal artery, and the left facial artery. Supraselective embolization of these vessels was performed with polyvinyl alcohol particles, resulting in nearly complete devascularization.
The surgical approach was via a subciliary incision, with exposure of the zygoma and orbital floor. An en bloc resection of the lesion was performed with reconstruction of the malar bone using Medpor, and of the orbital floor using titanium mesh. The open maxillary sinus was repaired with an Alloderm patch. Intraoperative bleeding was minimal; the surgeons felt that the preoperative embolization limited the bleeding and optimized a clean field for resection.
Discussion
Intraosseous hemangiomas of the facial bones are rare and most commonly arise in the maxilla, mandible, and nasal bones. Only 20 cases of zygomatic involvement have been reported in the English-language literature (1–10). Patients usually present in about the fourth decade of life with a tender or painless swelling of the malar eminence. There is a 3:1 female predominance. The lesion is more common on the left side, and there may be associated prior trauma. Clinical diagnosis may be difficult; in our case, the initial clinical impression favored fibrous dysplasia. Establishing the vascular nature of the lesion is critical in presurgical planning, as routine bone biopsy and curettage may result in severe hemorrhage.
Hemangiomas, which were originally classified as vascular neoplasms, are now thought to be hamartomas with an anomalous proliferation of endothelial-lined vascular channels. Malignant transformation has only been reported after radiation treatment. Osseous hemangiomas are slow growing, and treatment is not always necessary. Indications for surgery include correction of a mass effect (in our case, elevation of the eye), control of hemorrhage, and cosmesis. Because curettage may have a high morbidity due to uncontrolled hemorrhage, en bloc surgical excision, including a rim of normal bone, is usually the definitive treatment. Recurrence is rare. Radiotherapy is not recommended because of scar formation, impairment of regional bone growth in children, and, rarely, development of a malignant transformation.
CT is considered the most useful imaging technique because of its excellent characterization of trabecular and cortical detail. The CT appearance is variable, and in the calvaria most commonly shows a characteristic sharply marginated expansile lesion with intact inner and outer tables and a sunburst pattern of radiating trabeculae. “Soap bubble” and “honeycomb” configurations may also occur. MR imaging provides information about any associated soft tissue elements. The MR signal characteristics of a hemangioma are dependent on the quantity of slow-moving venous blood and on the ratio of red marrow to converted fatty marrow present within the lesion. Low or high signal may be seen on T1-weighted images, and high signal on water-sensitive sequences (11). Small lesions may appear bright on T1-weighted images; however, in larger lesions, the trabeculae typically show low signal on T1-weighted images. In cases in which a round, potentially benign bone lesion is initially detected on MR images, the lesion may be confused with other disease processes, including malignancy. The addition of a CT scan is recommended to evaluate the cortex and periosteum.
In our case, the diagnosis of an intraosseous hemangioma of the zygoma was suggested on the basis of the morphologic similarity of the lesion to a calvarial hemangioma. An intraosseous meningioma was thought unlikely, as the trabeculae were not perpendicular and the zygoma is an unlikely site for that lesion. Osteogenic sarcoma was also thought unlikely, as the cortex, although thinned, was preserved and there was no periostitis or associated soft tissue mass.
The usefulness of preoperative angiography and selective embolization has been debated in the literature. Although many authors recommend either embolization or external carotid ligation (1, 2, 4, 8), others state that proximal vascular control is unnecessary if an adequate margin of normal bone is resected (9, 10).
Conclusion
Intraosseous hemangiomas of the zygoma often show a characteristic cross-sectional configuration, with radiating trabeculae and intact, smooth cortices, as reported in six cases studied with CT and in two studied with MR imaging (1–3, 5, 6, 8). This appearance is pathognomonic, and allows for confident preoperative diagnosis.
Footnotes
1 Address reprint requests to Sandra Moore, MD, Department of Radiology, Mount Sinai Hospital, One Gustave Levy Place, Box 1234, New York, NY 10029.
References
- Received September 29, 2000.
- Accepted after revision January 3, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}