
Abstract
SUMMARY: Idiopathic hypereosinophilic syndrome (HES) is a heterogeneous disorder characterized by prolonged eosinophilia without an identifiable cause, ultimately resulting in organ dysfunction. Three major types of neurologic involvement have been well defined in HES; however, to our knowledge, inflammatory pseudotumor (IPT) in association with HES has not been reported. We present a case of IPT of the skull base in a patient with HES that suggests that HES may result in an exaggerated immunologic or inflammatory response leading to the formation of IPT.
Idiopathic hypereosinophilic syndrome (HES) was first defined by Chusid et al in 19751 as unexplained eosinophilia of greater than 1500/μL present for longer than 6 months with evidence of organ injury related to the hypereosinophilia, such as cardiomyopathy, peripheral neuropathy, and encephalopathy. The heterogeneity of HES ranges from those patients with myeloproliferative features (splenomegaly, increased vitamin B12 levels, abnormal leukocyte alkaline phosphatase scores, and cytogenetic abnormalities) to those patients with benign courses (associated with increases in immunoglobulin E [IgE], angioedema, and corticosteroid-responsive eosinophilia).2 The serum level of interleukin-5, an eosinophilopoietic cytokine, is increased in some patients with HES,3 and a few have been found to have T cell abnormalities, including CD3-CD4+CD8- T cells,4 and CD3+CD4-CD8- T cells.5 The organs most commonly involved are the heart, skin, lungs, spleen, and liver. Neurologic complications can involve both the peripheral and central nervous systems. We describe an unusual case of inflammatory pseudotumor (IPT) involving the skull base in a patient with HES who presented with multiple cranial nerve palsies.
Case Report
A 46-year-old white woman presented with double vision, mild ptosis, and markedly decreased vision in her left eye. The patient also complained of a 1-year history of intermittent left-sided facial pain and numbness around the left eye and left forehead.
Her medical history was significant for chronic sinusitis and HES, initially presenting with urticarial-like skin lesions. There was no history of drug allergies, travel outside the country or to tropical areas within the country. A skin biopsy showed an attenuated infiltrate consisting mostly of eosinophils throughout the reticular dermis, extending into the subcutaneous fat. Numerous “flame figures” (collagen and eosinophilic debris) were present, consistent with Well syndrome (eosinophilic cellulitis). Laboratory data consistent with HES included an elevated white blood cell count of 18 400/μL with an absolute eosinophil count of 2944/μL and an absolute neutrophil count of 11 960/μL at presentation that had been sustained for 6 years. Peripheral blood smear showed numerous eosinophils. Serum plasma electrophoresis showed normal total protein and gamma globulin levels with no discrete abnormality on electrophoresis; quantitative IgE level was elevated at 247 IU/mL (reference interval, 1–180) with normal immunoglobulin G (IgG) and immunoglobulin A (IgA) levels. A bone marrow aspirate revealed moderately hyperplastic bone marrow, with 11% eosinophils and eosinophil precursors and normal maturation of all cell lines. The erythrocyte sedimentation rate was 23 mm/h (reference interval, 1–20 mm/h).
An extensive evaluation for other causes of the eosinophilia was unrevealing. Serologic testing for toxocara and Strongyloides organisms was negative, pulmonary function tests were not consistent with asthma, and cortisol levels were found to be normal. No other organ involvement was uncovered. The patient was treated for the next several years with prednisone, hydroxyurea, and α-interferon. The skin lesions waxed and waned during this time.
Physical examination at our institution revealed a visual acuity of 20/20 in the right eye and 2/200 in the left eye, with a large left afferent pupil defect. Visual fields were full in the right eye, but the left eye field showed a central scotoma that extended inferiorly. Partial left 3rd and 6th nerve palsies were present. Both optic nerve heads appeared normal. There was decreased sensation in the 1st division of the left 5th cranial nerve (V1).
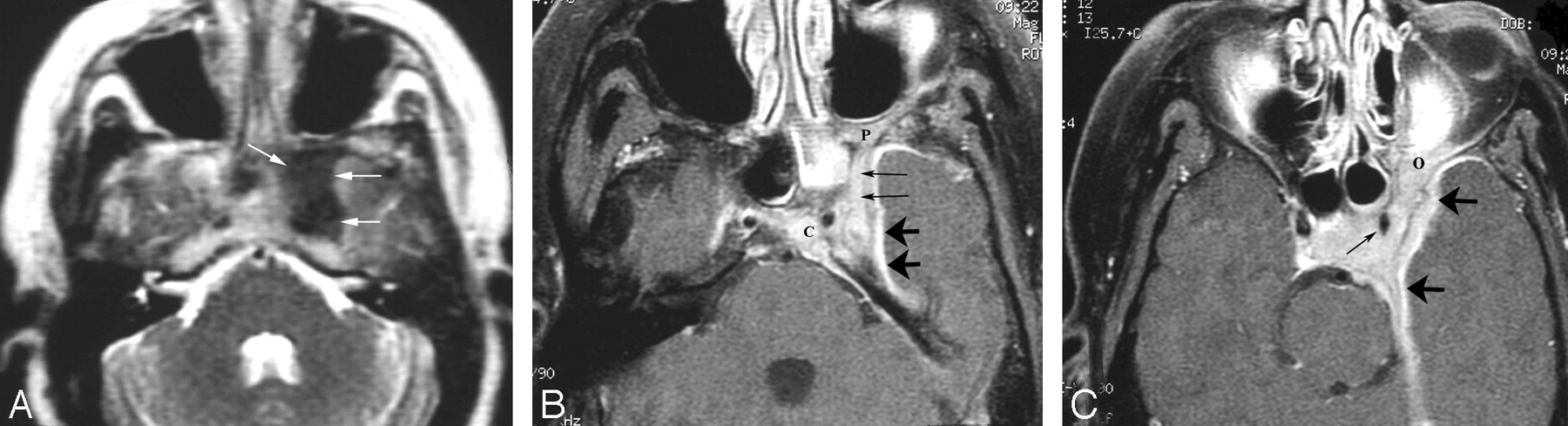
MR imaging revealed a mass in the left cavernous sinus with dural involvement, and extensive infiltration into the sella and suprasellar cistern, the left posterior orbit, and the left masticator space and pterygopalatine fossa (Fig 1A–C). The mass involved the left sphenoid sinus with deficiency of the lateral sinus wall. Diagnostic considerations included meningioma, an inflammatory lesion such as sarcoid, and malignant neoplasms including lymphoma. The patient had both CT-guided and endoscopic biopsies of the skull base mass. Histologic sections showed normal structures such as nerves and blood vessels entrapped in a fibroinflammatory process (Fig 2A, -B). Dense collagen fibrosis surrounded the nerves and fat cells. Within the fat, there was low-grade fat necrosis and infiltration by plasma cells, scattered eosinophils, lymphocytes, and histiocytes. No tumor was identified, nor were there any amyloid deposits. A diagnosis of IPT was rendered.

A 46-year-old woman with a history of idiopathic hypereosinophilic syndrome presented with multiple cranial nerve palsies.
A, Axial T2-weighted MR image shows a hypointense left skull base mass (arrows) at the region of the left basisphenoid.
B, Enhanced fat-suppressed axial T1-weighted MR image demonstrates the enhancing left skull base mass with involvement of the clivus (C), foramen rotundum (thin arrows), dura (thick arrows), and pterygopalatine fossa (P).
C, Enhanced fat-suppressed axial T1-weighted MR image shows a solidly enhancing mass (similar in appearance to a meningioma) involving the left cavernous sinus with some narrowing of the adjacent internal carotid artery (thin arrow), with associated thick dural enhancement (thick arrows). Also note involvement of the left orbital apex (O).

A, At medium power, most tissue fragments showed attenuated fibrosis (thick arrows) around nerves (thin arrows) and vessels (arrowhead), along with crushed inflammatory cells. Focal areas of fat necrosis are present at the periphery of the fibroinflammatory mass. (hematoxylin-eosin [H&E], original magnification ×100)
B. At high power, lymphocytes, histiocytes, plasma cells (arrow), and scattered eosinophils (arrowhead) are seen within the fatty tissue. (H&E, original magnification ×400)
The patient was treated with corticosteroids and imatinib mesylate (a protein kinase inhibitor) with dramatic improvement in her left eye vision (from 2/200 to 20/20 acuity), ocular motility, and left facial numbness. Follow-up MR imaging 3 months later revealed significant reduction in the size of the skull base mass and decreased meningeal enhancement. In addition, her cutaneous and hematologic manifestations of HES resolved on therapy.
Discussion
Idiopathic HES is characterized by sustained eosinophilia, without an identifiable underlying cause, and tissue injury resulting in organ damage by hypereosinophilia. It has a strong male preponderance, with a male-to-female ratio of 9:1, and most frequently involves the heart, lungs, nervous system, and skin.2 In 1 series, 65% of patients with HES had neurologic involvement, and some reports have described recurrent optic neuritis as the presenting symptom of HES.6,7 Three major types of neurologic involvement have been defined as follows: peripheral polyneuropathy, encephalopathy, and central nervous system (CNS) thromboemboli. Peripheral polyneuropathy is most common, occurring in approximately 50% of patients with HES, and may manifest as a sensory neuropathy, mononeuritis multiplex, radiculopathy, or muscle atrophy caused by denervation.2,6
Patients with encephalopathy have memory loss, confusion, ataxia, incoordination, weakness, and upper motor neuron signs including increased muscle tone, deep tendon reflexes, and a positive Babinski reflex.8 Seizures, intracranial hemorrhages, dementia, and organic psychoses occur less frequently.2 Eosinophilic meningitis occurs uncommonly.8 The pathogenesis of both the encephalopathy and peripheral neuropathy of HES remains unknown. Possible mechanisms include direct damage from the infiltration of eosinophils and other inflammatory cells and injury from a toxin originating within eosinophils.6
Embolic disease to the CNS may be caused by intracardiac thrombus formation secondary to eosinophilic infiltration resulting in endomyocardial fibrosis and thrombus formation.6 However, thromboemboli may also occur without demonstrable cardiac disease and can be the presenting manifestation of HES. In these cases, it has been postulated that thrombosis within the vessels of the CNS may be the underlying mechanism.2
To our knowledge, IPT in association with HES has not been described. “IPT” is a clinicopathologic term used to describe a reactive inflammatory and nonneoplastic process. In the literature, “pseudotumor” has been given many different names, some of which are plasma cell granuloma, plasmacytoma, inflammatory myofibroblastic tumor proliferation, and histiocytoma.9 IPT has been described most often in the lung and orbit, with other systemic sites somewhat less frequently. Involvement of the CNS parenchyma by IPT is rare.10-15 The lesions occur throughout the brain parenchyma and meninges, without restriction to a particular area.10 IPT can both clinically and radiologically mimic a malignant process.9
The pathologic mechanism for IPT remains obscure.10 The histology is similar in all cases with variable amounts of plasma cells, lymphocytes, histiocytes, and fibroblasts. In several reported cases, patients had elevated levels of serum immunoglobulins and erythrocyte sedimentation rates, leading to the hypothesis that the lesion may have resulted from an exaggerated immunologic or inflammatory process occurring at sites of injury or infection.10 The case presented here suggests that a similar process may occur in HES and result in IPT.
The differential diagnostic considerations of a mass in the cavernous sinus with dural enhancement include meningioma, lymphoma, neurosarcoidosis, infection, and amyloidosis. Although the radiographic features in this case had a tumorlike presentation, the histologic findings were nonneoplastic. Given the histologic characteristics, we classified the lesion as IPT. Treatment with steroids and a protein kinase inhibitor resulted in significant improvement of the patient's symptoms and radiologic findings. IPT with a prominent eosinophilic component may complicate HES and should be added to the list of conditions associated with this rare disorder.
References
- Received November 8, 2004.
- Accepted after revision September 17, 2006.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.