
Abstract
BACKGROUND AND PURPOSE: Interpretation of CT of the anterior skull base in children depends on knowledge of the pattern and chronology of ossification. The purpose of this study was to ascertain the age at which the anterior cranial fossa is fully ossified as assessed on CT examinations.
MATERIALS AND METHODS: This was a retrospective review of 127 CT examinations of children ranging from 1 day to 16 years 7 months of age without known or suspected anterior cranial fossa abnormality. Measurements of the length and width of the anterior skull base and the presence and size of the most anterior unossified portion were determined by 2 investigators.
RESULTS: At birth, the anterior skull base consists mainly of cartilage. There is a wide variation in ossification rates between individuals, but the anterior skull base was fully ossified at 3 years 10 months in all of our cases.
CONCLUSIONS: In healthy individuals, the anterior skull base is fully ossified by 4 years of age.
Abbreviations
- cg
- crista galli
- cp
- cribriform plate
- f
- frontal bones
- fc
- foramen cecum
- hp
- hard palate
- p
- perpendicular plate of the ethmoid bone
- s
- sphenoid bone
An important indication for imaging the anterior skull base is the evaluation of developmental midline masses such as nasal dermal sinuses, anterior cephaloceles, and nasal gliomas.1–3 All of those lesions may retain a connection with the intracranial compartment via the anterior cranial fossa, and an important role of imaging is to determine whether such a connection exists because this will affect surgical treatment substantially.1–4
Interpretation of anterior skull base imaging in young children can be difficult because most of the bone forms as cartilage, with only a small component of membranous bone,5 and ossification occurs from multiple centers.4,6 A good knowledge of the above features is, therefore, essential for the radiologist interpreting these studies. In a study of 61 children ranging in age from neonate to 24 months, Belden et al6 described the timing and pattern of ossification of the anterior skull base. By 24 months, it was shown that 84% of the anterior skull base was ossified, with a cartilaginous gap in the region of the foramen cecum. To our knowledge, no study has addressed the question of the age at which anterior skull base ossification is complete on radiologic analysis.
The purpose of this study was to ascertain the age at which the anterior cranial fossa is fully ossified as assessed on CT examinations.
Materials and Methods
CT scans that covered the anterior skull base obtained at our institution between August 2001 and February 2008 were identified by a computerized search. One hundred thirty-five patients were identified initially, but after review of the clinical details from the imaging requests and imaging reports, 8 patients with known metabolic or developmental anomalies of bone or conditions known to affect development of the anterior skull base were excluded from the study, leaving 127 examinations for analysis. All the CT examinations were performed on the same machine, and the images were reviewed on an Advantage workstation (GE Healthcare, Milwaukee, Wisconsin). Images were acquired in the axial plane with collimation ranging from 1.2 to 2.5 mm and were reformatted on the workstation into sagittal and coronal planes. One hundred twenty-three examinations had a high-resolution bone algorithm, while 4 patients had examinations on a soft-tissue algorithm that were deemed to have acceptable quality for interpretation. The images were reviewed retrospectively by 2 of the authors (D.C.H. and M.J.K.).
Measurements were made of the length of the anterior skull base (the nasion to the posterior clinoid process, Fig 1A) on a midline sagittal image and of any anterior bony defect present (Fig 1B). Measurements were made of the width of the anterior skull base (minimum interorbital distance at the level of the posterior globe, Fig 2A) on a coronal image. The maximum width of any anterior bony defect present was measured on an anterior coronal image just posterior to the frontal bone (Fig 2B). The mean value for each of the 4 measurements was calculated. In the absence of a published standard for measuring the length and width of the skull base on CT, we chose the above measurements because they used easily identified anatomic landmarks and were, therefore, likely to be reproducible. The most anterior unossified portion of the skull base was measured because it is apparent from previous studies that this is the last area to ossify and has the most important clinical implications in terms of assessment of developmental midline masses such as nasal glioma.

Sagittal skull base measurements (2 years of age). A, Midline sagittal CT scan demonstrates measurement of the anterior skull base from the nasion to the posterior clinoid process. B, Midline sagittal CT scan demonstrates sagittal measurement of the most anterior unossified portion of the anterior skull base.
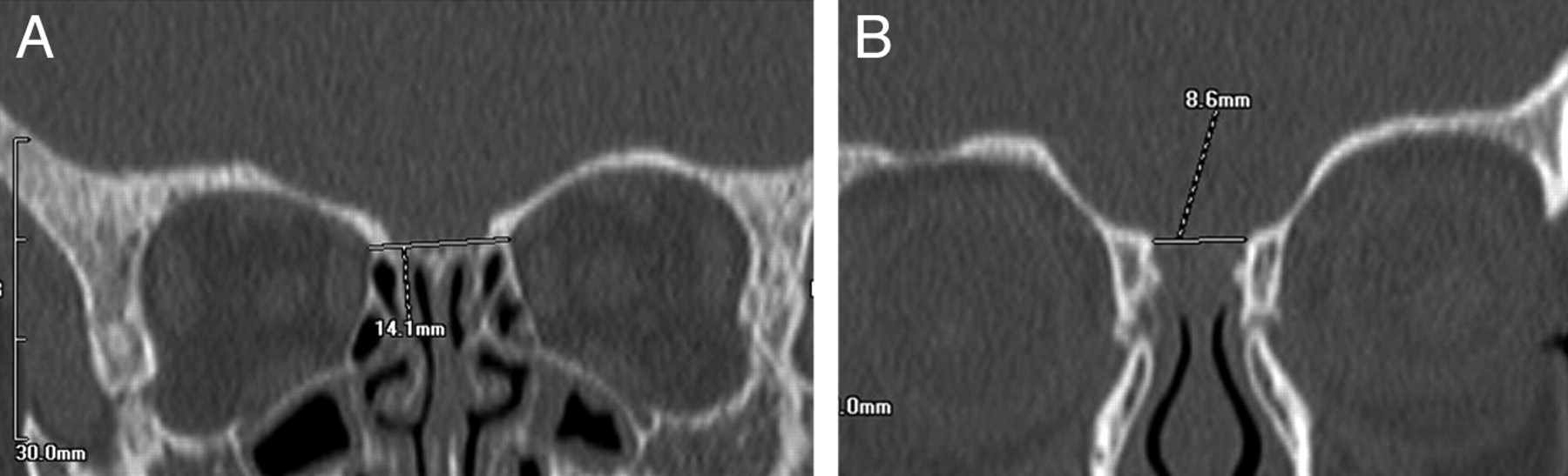
Coronal skull base measurements (2 years of age). A, Coronal CT scan shows measurement of the minimum interorbital distance at the level of the posterior globe. B, Coronal CT scan shows coronal measurement of the unossified portion of the anterior skull base just posterior to the frontal bones.
The presence of a normal foramen cecum was noted and distinguished from an unossified anterior cranial floor. The mean length and width of the unossified anterior skull base were plotted against patient age to determine whether a clear cutoff age could be found, beyond which the anterior skull base is always fully ossified in healthy individuals.
Results
Of the 127 examinations included, 60 (47.2%) were of females (range, 0–16 years 5 months; median, 7 years 6 months) and 67 (52.8%) were of males (range, 0–16 years 4 months; median, 9 years 4 months). The ages were rounded down to the nearest month for the purposes of the study.
Figure 3A, -B shows the mean skull base length and width, respectively, plotted against age. It demonstrates the good correlation between age and skull base dimension with continued growth after ossification is completed, which plateaus in adolescence.

A, Scatterplot shows the positive relationship between skull base length and age. B, Scatterplot shows the positive relationship between skull base width and age.
Figure 4A, -B shows the mean size of the unossified anterior skull base in the sagittal and coronal planes, respectively. This shows that there is a wide variation in the amount of unossified anterior skull base in the first few years but that by 3 years 10 months of age, 100% of children had a fully ossified anterior skull base. The 2 neonate children in our study are shown on the graphs in Fig 4A, -B as having particularly large amounts of unossified skull base. This reflects the fact that the amount of ossification is limited at birth and proceeds rapidly in the first 6 months of life.

A, Scatterplot shows the size of the most anterior unossified portion of anterior skull base measured in the sagittal plane versus age. B, Scatterplot shows the size of the most anterior unossified portion of the anterior skull base measured in the coronal plane versus age.
Discussion
The anterior cranial fossa (Fig 5) comprises anteriorly and laterally the frontal bone, while its floor comprises the orbital plate of the frontal bone, the cribriform plate of the ethmoid bone, and the lesser wings and anterior part of the body of the sphenoid bone. The cribriform plate of the ethmoid bone occupies the midline between the 2 orbital plates but is depressed below them, separating the anterior cranial fossa from the nasal cavity. Anteriorly the median crista galli projects upward between the frontal lobes. A depression between the crista galli and the crest of the frontal bone is crossed by the frontoethmoidal suture and contains the foramen cecum. The foramen cecum is usually plugged by the fibrous tissue of the falx but occasionally transmits a vein from the nasal mucosa to the superior sagittal sinus. Posteriorly each cribriform plate articulates with the body of the sphenoid bone.

Age 4 years 7 months. Anterior (A) and posterior (B) coronal, midline (C), and parasagittal (D) images show complete ossification of the anterior skull base with typical well-corticated margins of the foramen cecum.
The perpendicular plate of the ethmoid bone, thin, flat, and median, descends from the cribriform plate to form the upper nasal septum. Laterally on either side are 2 vertical plates, between which are the cells of the ethmoidal labyrinths. The lateral orbital plate of the ethmoid bone is part of the medial orbital wall and the lateral nasal wall. The superior and middle conchae are formed from this medial vertical plate, separated by the narrow oblique superior meatus.
The sphenoid bone completes the floor of the fossa posteriorly. Centrally, the anterior part of its upper surface, the jugum sphenoidale, articulates anteriorly with the cribriform plate; posteriorly, it is the anterior bank of the sulcus chiasmatis, crossing the sphenoid body centrally in the middle cranial fossa and connecting the optic canals. The medial ends of the posterior borders of the lesser wings of the sphenoid bone form the anterior clinoid processes.
As described by Belden et al,6 ossification of the anterior skull base proceeds in a reasonably constant manner. Most of the skull base begins as cartilage. At birth, the frontal bones are well ossified and extend to the medial edge of the orbit (Fig 6). Ossification of the cribriform plate begins in the region of the vertical attachments of the superior and middle turbinates and spreads along the surface of the cribriform plate to reach the crista galli at approximately 2 months of age. Ossification tends to proceed from the central portion of the cribriform plate in both anterior and posterior directions. Anterior ossification takes place more slowly, resulting in an anterior gap between the ethmoid and nasal bones in most children (Figs 6–8). The earliest age at which complete ossification was seen in this area was 14 months, and Belden et al showed that by 2 years of age, most children still had a gap in this region, with only 8% having complete ossification anterior to the margin of the cribriform plate. Our observations agree with the patterns described above, with only 4% of children in our study having complete ossification of the anterior skull base by 2 years of age.

Age, 22 days. Anterior (A) and posterior (B) coronal, midline (C), and parasagittal (D) images show ossification of the frontal bones and superior turbinates (asterisks) but no ossification of the cribriform plate or crista galli (arrows).

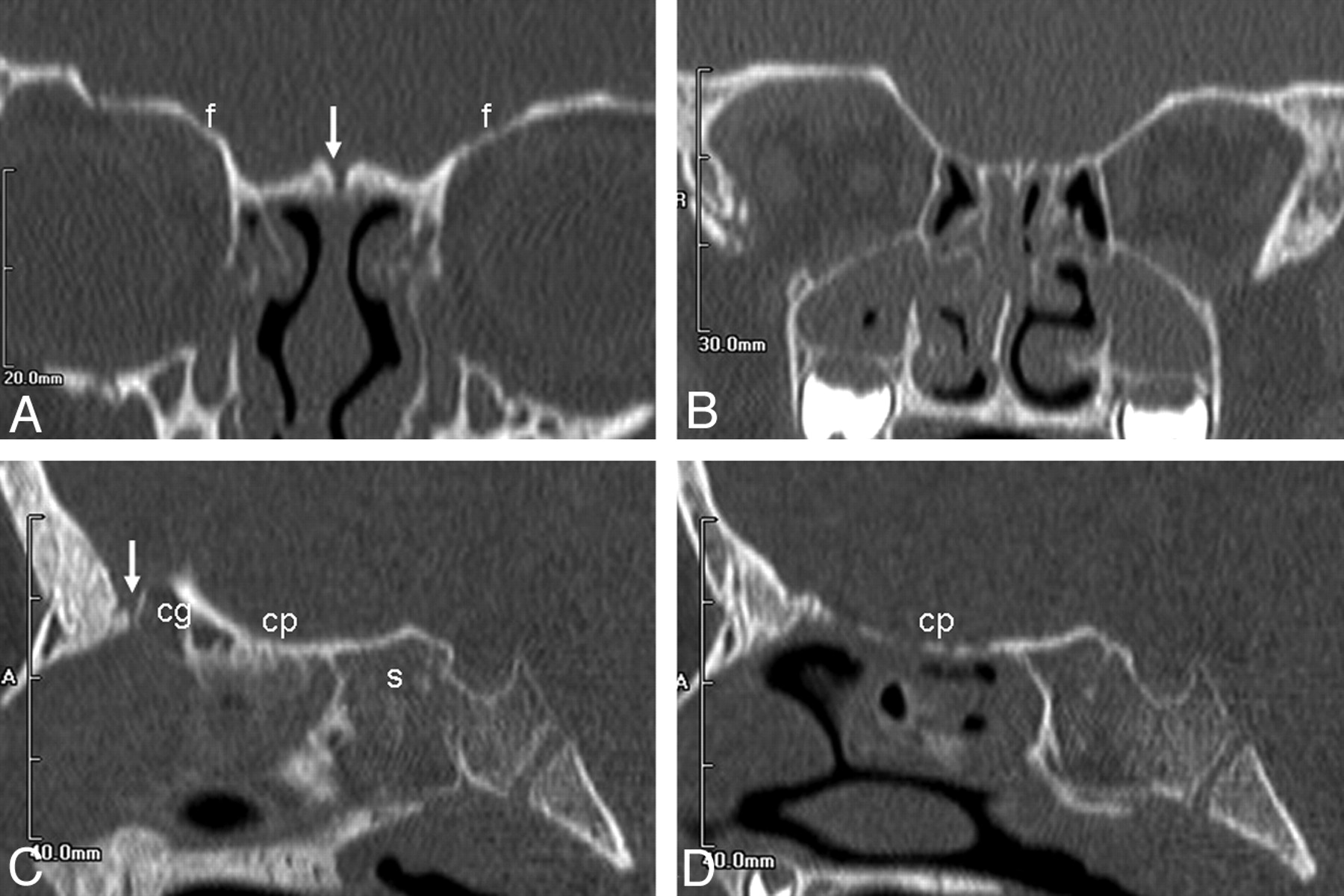
Age, 9 months. Anterior (A) and posterior (B) coronal, midline (C), and parasagittal (D) images show that ossification is more complete posteriorly than anteriorly, with ossification of the cribriform plate extending laterally to the frontal bones. There is a persistent unossified portion anteriorly (asterisk).

Age, 3 years 3 months. Anterior (A) and posterior (B) coronal, midline (C), and parasagittal (D) images show progressive ossification of the cribriform plate posteriorly, with only a small persistent unossified portion of the skull base anteriorly (arrow).
Imaging of the anterior skull base is infrequently requested in children. However, it is important to understand how the maturation of this area results in changing appearances on CT according to the age of the patient. As reported above, Belden et al6 have described changes relating to the ossification of the anterior skull base on CT up to 2 years of age. In a small pathologic study, van Loosen et al7 found that the skull base was fully ossified by 6 years of age. Our study expands on this information by assessing more precisely the age at which complete ossification of the anterior skull base can be expected (Figs 3 and 4). This is important when evaluating lesions that have the potential to extend intracranially, in particular developmental midline masses such as nasal glioma or anterior cephalocele. We have shown that after 4 years of age, the anterior skull base can be expected to be fully ossified in individuals who have no clinical suspicion of skull base abnormality. Absence of complete ossification in children older than 4 years of age should, therefore, raise the suspicion of intracranial extension or of a bony metabolic disorder or dysplasia. This information is of use in helping to decide which patients may require further investigation with MR imaging.
Some children have a persistent foramen cecum (the remnant of the dural diverticulum, which extends from a midline opening anterior to the crista galli and temporarily reaches the subcutaneous region of the midnasal bridge), which might potentially be confused with a bony defect in a child whose anterior skull base should be fully ossified, though the well-defined, corticated margins (Fig 5) usually allow the correct interpretation. Previous studies have looked at widening of the foramen cecum as an indirect marker of intracranial extension.2,4 Pensler et al8 reported 10 patients in whom an enlarged foramen cecum was taken as evidence of intracranial extension, with 7 of them having a bifid crista galli. At craniotomy, however, none of the patients were found to have intracranial lesions. Bloom et al9 found that a normal size and appearance of the foramen cecum and crista galli seemed to rule out intracranial extension but that isolated widening of the foramen cecum and a bifid crista galli were only suggestive of intracranial extension, requiring further evaluation by MR imaging. These studies suggest that widening of the foramen cecum alone is not a strong marker for intracranial extension, though a normal foramen cecum is useful in excluding this complication.
CT, in comparison with MR imaging, has many advantages in pediatrics. Scanning times are short, often negating sedation or anesthetics, and isotropic voxels allow reformats in any plane. Claustrophobia is also less of a problem. However, because imaging of the anterior skull base is infrequently performed in this age group, image interpretation of the evolving ossification can be difficult. The information from our study will help radiologists interpreting such imaging.
Conclusions
The anatomy and embryology of the anterior skull base are complex. A sound knowledge of the normal appearances on imaging at different ages is essential for the radiologist. We have shown that beyond 4 years of age, the anterior skull base can be expected to be fully ossified on CT.
Acknowledgments
We thank Yvonne Vickers, radiographer at Sheffield Children's Hospital, for her help in obtaining archived scans for review and also for sharing her expertise regarding image manipulation on the workstation, and Dan Pickering, MD, for his technical help in preparing this manuscript.
Footnotes
-
Paper previously presented as an electronic poster at: Annual Meeting of the British Society of Neuroradiology, October 10–12, 2008; Manchester, United Kingdom.
References
- Received October 14, 2009.
- Accepted after revision December 21, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.