
Abstract
BACKGROUND AND PURPOSE: Induced hypothermia is thought to work partly by mitigating reperfusion injury in asphyxiated term neonates. The purpose of this study was to assess brain perfusion in the first week of life in these neonates.
MATERIALS AND METHODS: In this prospective cohort study, MR imaging and ASL-PI were used to assess brain perfusion in these neonates. We measured regional CBF values on 1–2 MR images obtained during the first week of life and compared these with values obtained in control term neonates. The same or later MR imaging scans were obtained to define the extent of brain injury.
RESULTS: Eighteen asphyxiated and 4 control term neonates were enrolled; 11 asphyxiated neonates were treated with hypothermia. Those developing brain injury despite being treated with induced hypothermia usually displayed hypoperfusion on DOL 1 and then hyperperfusion on DOL 2–3 in brain areas subsequently exhibiting injury. Asphyxiated neonates not treated with hypothermia who developed brain injury also displayed hyperperfusion on DOL 1–6 in brain areas displaying injury.
CONCLUSIONS: Our data show that ASL-PI may be useful for identifying asphyxiated neonates at risk of developing brain injury, whether or not hypothermia is administered. Because hypothermia for 72 hours may not prevent brain injury when hyperperfusion is found early in the course of neonatal hypoxic-ischemic encephalopathy, such neonates may be candidates for adjustments in their hypothermia therapy or for adjunctive neuroprotective therapies.
ABBREVIATIONS
- ASL
- arterial spin labeling
- aEEG
- amplitude-integrated electroencephalogram
- ASL-PI
- perfusion imaging by arterial spin labeling
- BG
- basal ganglia
- CGM
- cortical gray matter
- DOL
- day of life
- EEG
- electroencephalogram
- FiO2
- fraction of inspired oxygen
- GM
- gray matter
- HI
- hypoxic-ischemic
- HIE
- hypoxic-ischemic encephalopathy
- PASL
- pulsed arterial spin-labeling
- pCO2
- partial pressure of carbon dioxide
Neonatal HI brain injury is an evolving process initiated by the HI insult leading to decreased blood flow to the brain (primary lesions), followed by the restoration of blood flow in an injured brain and the initiation of a cascade of pathways. This cascade includes accumulation of extracellular glutamate with excessive activation of glutamate receptors, calcium influx, and the generation of reactive oxygen and nitrogen species, leading to cell death and definitive brain injuries (secondary lesions).1 The biochemical cascade accompanying restoration of brain perfusion (so-called “reperfusion injury”) is a primary target for neuroprotective interventions, but such interventions are currently limited by insufficient knowledge of the timing and duration of the therapeutic window in neonates.2⇓–4 As the only clinically tested neuroprotective treatment to minimize brain injury in asphyxiated term neonates,5⇓⇓⇓⇓–10 induced hypothermia has been shown to lower CBF and to mitigate reperfusion injury.11 It is unclear why induced hypothermia seems effective in preventing brain injury and improving neurologic outcome in some asphyxiated neonates but not in all of them, especially not in those with severe HIE.6,10 Methods for early identification of patients who would benefit from adjustments in their hypothermia therapy or from adjunctive neuroprotective therapies12 would be useful.
This study was designed to assess the following: 1) the pattern of brain perfusion in the first week of life by MR imaging and ASL-PI in asphyxiated term neonates, and 2) whether brain perfusion abnormalities during the first week of life in asphyxiated neonates treated with induced hypothermia correlate with brain injury observed in these patients after hypothermia treatment is completed. The latter may help identify asphyxiated neonates undergoing hypothermia treatment who might benefit from tailoring of neuroprotective strategies.
Materials and Methods
We conducted a prospective cohort study of consecutive term neonates with HIE admitted during their first week of life to the neonatal intensive care unit. They were enrolled if they met criteria for treatment with induced hypothermia,6,7,9,10 or if they had evidence of perinatal depression and manifested HI brain injury on subsequent brain imaging (ie, BG pattern, watershed pattern, or total cortical injury pattern).13⇓–15 Markers of perinatal depression included seizures within 72 hours of birth or at least 2 of the following criteria: 1) an acute perinatal event; 2) umbilical artery pH < 7.1; 3) 10-minute Apgar score, ≤5; or 4) multiorgan failure.13,16,17 Eligible patients received whole-body cooling to an esophageal temperature of 33.5°C, initiated by 6 hours of life, and continued for 72 hours (unless contraindications developed), and then they were slowly rewarmed.7 Per protocol, patients who arrived after the first 6 hours of life were not eligible for induced hypothermia. Neonates with strokes, metabolic disorders, or venous patterns of injury were not included.
Four additional term neonates without any signs of encephalopathy were included as healthy controls; findings on their brain MR images were normal. Each of them was only scanned once, on days 2, 3, 4, and 10 of life, respectively.
Neonates treated with induced hypothermia were categorized according to their initial background pattern of aEEG into 2 categories: moderately or severely abnormal.6,18 The aEEG recording was started as soon as the patient was admitted to the neonatal intensive care unit. Hypothermia treatment was usually initiated at the same time to avoid delay. Seizures evident clinically or identified by aEEG or standard EEG were also recorded. Other variables influencing the CBF (temperature, pCO2, FiO2, hematocrit levels, mechanical ventilation, pressor support, sedation, antiepileptic treatment) were also recorded on the day of the MR imaging.
This study was approved by the institutional review board, and parental consent was obtained. One or 2 MR images were obtained in each asphyxiated neonate during the first week of life, preferably an MR imaging on DOL 1 and on DOL 2–3 in neonates treated with induced hypothermia. Patients receiving hypothermia treatment had hypothermia maintained during the MR imaging without any adverse events.19 Any ventilatory support, pressor support, or sedation was also maintained during the MR imaging process; additional sedation was avoided. MR imaging was performed with a 3T Magnetom Trio scanner (Siemens, Erlangen, Germany), by using a 32-channel head coil in most cases (Siemens)20 or a standard 12-channel head coil. A pulsed ASL sequence21 (with TR/TE, 2400/13 ms; matrix size, 64 × 64; FOV, 192 mm; 15 axial sections with a section thickness of 4.9 mm) was acquired with high-spatial-resolution anatomic T1- and T2-weighted images and DWI. Anatomic sequences included a T1-weighted magnetization-prepared rapid acquisition of gradient echo (TR/TE, 1600/2.2 ms; matrix size, 192 × 192; FOV, 180 mm; 160 sagittal sections with a section thickness of 1.0 mm) and a T2-weighted fast spin-echo (TE, 123 ms; matrix size, 256 × 256; FOV, 220 mm; 110 axial sections with a section thickness of 1.0 mm). They were supplemented by single-shot spin-echo echo-planar diffusion-weighted (b = 750 s/mm2) isotropic images (TR/TE, 8400/84 ms; matrix size, 128 × 128; FOV, 220 mm; 50 axial sections with a section thickness of 2.2 mm). ADC maps were generated off-line. Regional CBF maps were obtained from the PASL Postprocessing Functor (Siemens). Quantitative estimates of regional CBF were made by using the formula described by Wang et al22:
 M0 was estimated by measuring the fully relaxed signal intensity and ΔM by the average difference in signal intensity between control and tag acquisitions. The conversion efficiency α was assumed to be 95% and the blood/tissue water partition coefficient λ, to be 1.2 mL/g, with TI1 / TI2 = 700/1400 ms and the longitudinal relaxation time of blood T1a = 1500 ms.23 The imaging sections were positioned axially covering the brain, and the acquisition order was ascending (inferior to superior) to reduce the required TI2. The labeling slab had a thickness of 50 mm and was positioned with a gap of 10 mm below the most proximal section. The labeling slab thus covered the lower part of the head and the neck but not the upper part of the chest, and thus not the heart. Quantification of regional CBF was performed by using the relative CBF images. Manually drawn regions of interest (Fig 1) were placed in 3 types of tissue: CGM (within the frontal, parietal, and occipital cortices), WM (within frontal and posterior white matter and the centrum semiovale), and BG (within the lentiform nucleus, the posterior limb of the internal capsule, and the thalamus).15,17,24 A total of 9 regions of interest were thus used; measurements were obtained in the right and left side of the cerebrum in these tissue regions. Their sizes depended on the location of the regions of interest. Regions of interest were always drawn by 1 observer in similar brain areas for all the MR images, without regarding the presence or absence of brain injury on DWI or other MR images. Regions of interest were manually drawn on the ASL data, by looking at the same time at the ASL data and the corresponding T2-weighted imaging; coregistration was not used. Motion during the MR imaging may cause severe artifacts in the acquired images, especially the PASL images. These were minimized by wrapping the neonates in an MR imaging−compatible vacuum cushion. In addition, a 3D prospective acquisition-correction technique was used with the PASL sequence for reducing motion-induced effects on magnetization history.
M0 was estimated by measuring the fully relaxed signal intensity and ΔM by the average difference in signal intensity between control and tag acquisitions. The conversion efficiency α was assumed to be 95% and the blood/tissue water partition coefficient λ, to be 1.2 mL/g, with TI1 / TI2 = 700/1400 ms and the longitudinal relaxation time of blood T1a = 1500 ms.23 The imaging sections were positioned axially covering the brain, and the acquisition order was ascending (inferior to superior) to reduce the required TI2. The labeling slab had a thickness of 50 mm and was positioned with a gap of 10 mm below the most proximal section. The labeling slab thus covered the lower part of the head and the neck but not the upper part of the chest, and thus not the heart. Quantification of regional CBF was performed by using the relative CBF images. Manually drawn regions of interest (Fig 1) were placed in 3 types of tissue: CGM (within the frontal, parietal, and occipital cortices), WM (within frontal and posterior white matter and the centrum semiovale), and BG (within the lentiform nucleus, the posterior limb of the internal capsule, and the thalamus).15,17,24 A total of 9 regions of interest were thus used; measurements were obtained in the right and left side of the cerebrum in these tissue regions. Their sizes depended on the location of the regions of interest. Regions of interest were always drawn by 1 observer in similar brain areas for all the MR images, without regarding the presence or absence of brain injury on DWI or other MR images. Regions of interest were manually drawn on the ASL data, by looking at the same time at the ASL data and the corresponding T2-weighted imaging; coregistration was not used. Motion during the MR imaging may cause severe artifacts in the acquired images, especially the PASL images. These were minimized by wrapping the neonates in an MR imaging−compatible vacuum cushion. In addition, a 3D prospective acquisition-correction technique was used with the PASL sequence for reducing motion-induced effects on magnetization history.

Axial PASL images showing the manually drawn regions of interest. A total of 9 regions of interest were placed in 3 types of tissue. a, CGM (within frontal, parietal, and occipital cortices). b and c, WM (within the frontal and posterior WM and the centrum semiovale) (b) and BG (within the lentiform nucleus and the posterior limb of internal capsule and the thalamus) (c).15,17,24 Measurements were obtained in the right and left sides of the cerebrum in these tissue regions. Regions of interest were always drawn on the ASL data by 1 observer in similar brain areas for all the MR images by looking at the same time at the ASL data and the corresponding T2-weighted imaging.
Conventional sequences were obtained during the same or later MR imaging studies and were used to define the extent of brain injury in these patients and to correlate it with brain perfusion measurements. Neuroradiologists, who were blinded to the clinical condition of the neonates, interpreted the brain MR images (T1- and T2-weighted images and DWI). Each MR image was evaluated for BG injury, watershed pattern injury, and/or BG/watershed pattern injury.25 This MR imaging assessment provided a description of the distribution and extent of injury. The MR imaging results were categorized as “abnormal” or “normal,” depending on whether they showed MR imaging evidence for HI brain injury in the CGM, WM, and/or BG.26
Statistical analysis was focused on comparisons between CBF values measured in the first week of life and the presence or absence of later brain injury. We calculated the mean of the CBF values for each region of interest in each subject. After obtaining these values, we then divided the asphyxiated neonates into 2 groups, based on the presence or absence of later brain injury in each region of interest, and compared the values in these 2 groups with the control group of neonates. To compare CBF values between each group, we performed statistical analyses by using a logistic regression model with the presence or absence of injury as the variable and mean brain perfusion as the outcome. We also considered, in the regression model, the possible effects of other variables influencing CBF, such as temperature, pCO2, FiO2, hematocrit level, ventilatory support, pressor support, sedation, and antiepileptic treatment. The P value was derived from the null hypothesis that the regression coefficient for the presence or absence of injury is equal to zero. The test is the Wald test for regression coefficients. A P value <.05 was considered significant.
Results
Eighteen term neonates with perinatal HIE were enrolled (On-line Table 1), 11 of whom received therapeutic hypothermia. Among the neonates treated with induced hypothermia, 4 had an initial moderately abnormal aEEG background, and 7 had an initial severely abnormal aEEG background. None of the neonates with an initial moderately abnormal aEEG background (patients 1, 2, 3, and 4) developed significant HI brain injury. Among the 7 neonates who had an initial severely abnormal aEEG background, 3 did not develop clear MR imaging evidence of HI brain injury, but 4 did. Of note, HI brain injury in these 4 patients was not evident on the first DOL by conventional MR imaging modalities, including anatomic T1- and T2-weighted imaging, and DWI but did became apparent on the later MR images.
The 7 neonates who were not cooled but who developed significant MR imaging evidence of HI brain injury were admitted beyond the 6-hour time interval in which they would have been eligible for cooling. aEEG was not available in these 7 neonates; however, EEG findings were available for those with suspected seizures and confirmed the seizures in these patients.
Four control term neonates with normal brain MR imaging findings were also enrolled.
CBF values were measured on the different scans (On-line Table 2).
In the neonates treated with induced hypothermia who did not develop hypoxic-ischemic brain injury, CBF values measured in the first DOL were decreased in the CGM and BG compared with control patients; values in the WM were similar to values measured in control patients. The hypoperfusion measured in the CGM and BG was more pronounced in the first hours after birth and in neonates with an initial severely abnormal aEEG background and tended to normalize during the first DOLs. On DOL 2, CBF values in the CGM, WM, and BG in neonates with an initial moderately abnormal aEEG background were very similar (CGM and WM) or only slightly decreased (BG) compared with controls, even if the patients were being treated with induced hypothermia during the MR imaging. In neonates with an initial severely abnormal aEEG background, perfusion in the CGM and BG became similar only on DOL 3 compared with control neonates. Of note, patient 1 had much lower CBF values in the CGM and BG. This may be due, in part, to the timing of the scan relative to the HI event. Additionally, this was the only patient with pCO2 values of 26.8 mm Hg just before MR imaging (all the other patients had pCO2 values between 30 and 40 mm Hg).
Compared with control patients and asphyxiated neonates who were treated with hypothermia but who did not develop brain injury, CBF values were more markedly decreased on DOL 1 in the brain areas subsequently exhibiting injury in the neonates treated with hypothermia, who developed MR imaging evidence of HI brain injury (Figs 2–4). On DOL 2, CBF values were increased in the injured brain areas (Figs 2–4) in these neonates. The only exception was patient 9 with BG injury, in whom CBF remained decreased in the BG. In these neonates, the brain regions that did not show any later brain injury had CBF values comparable with those of patients with an initial severely abnormal aEEG background who did not develop brain injury.

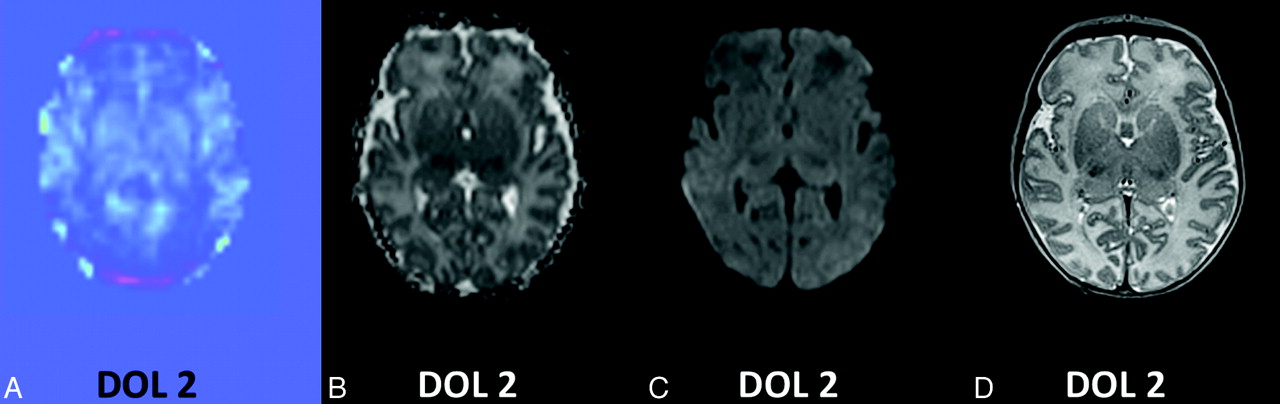
Brain MR imaging in a control neonate; comparison between the perfusion map and images obtained from conventional sequences. A, CBF map obtained by perfusion imaging by ASL shows higher brain perfusion in GM and in BG compared with WM. B, ADC map. C, DWI. D, T2-weighted imaging.
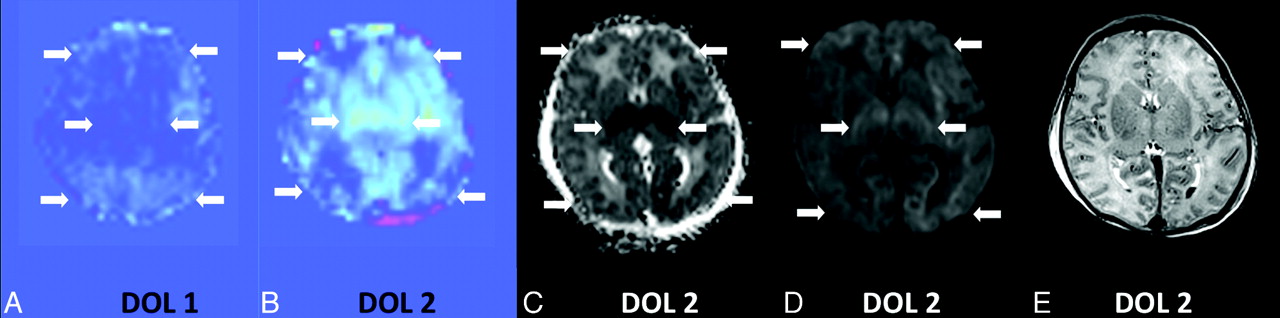
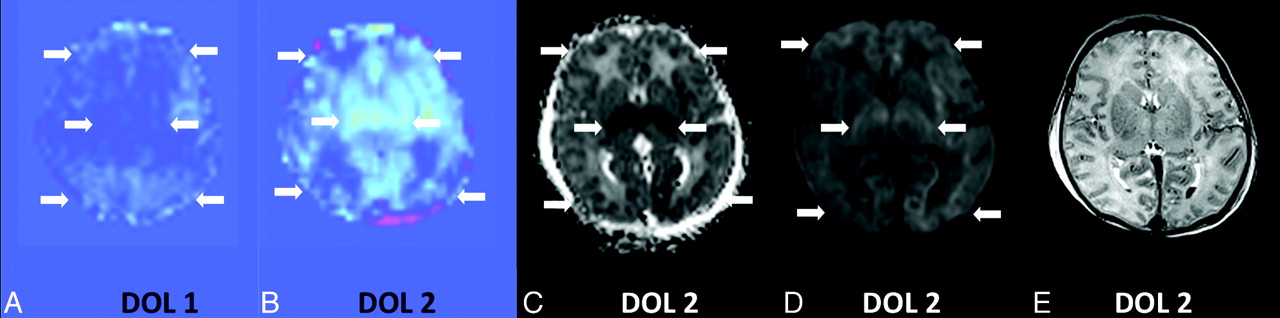
Brain MR imaging on DOL 2 in patient 5 while he was treated with induced hypothermia; comparison between the perfusion map and images obtained from conventional sequences. A and B, CBF maps obtained by perfusion imaging by ASL show decreased brain perfusion on DOL 1 (A) followed by increased brain perfusion on DOL 2 (B) in the GM, WM, and BGs bilaterally, compared with the control patient. C and D, ADC map (C) and DWI (D) on DOL 2 display multifocal areas of restricted diffusion within bilateral BGs and both cerebral hemispheres involving GM and WM. E, Changes on T2-weighted imaging on DOL 2 are subtle.
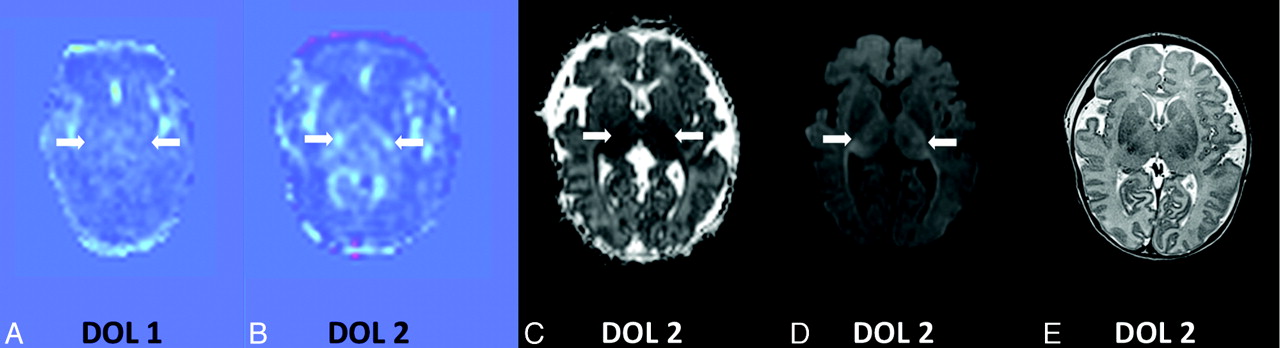
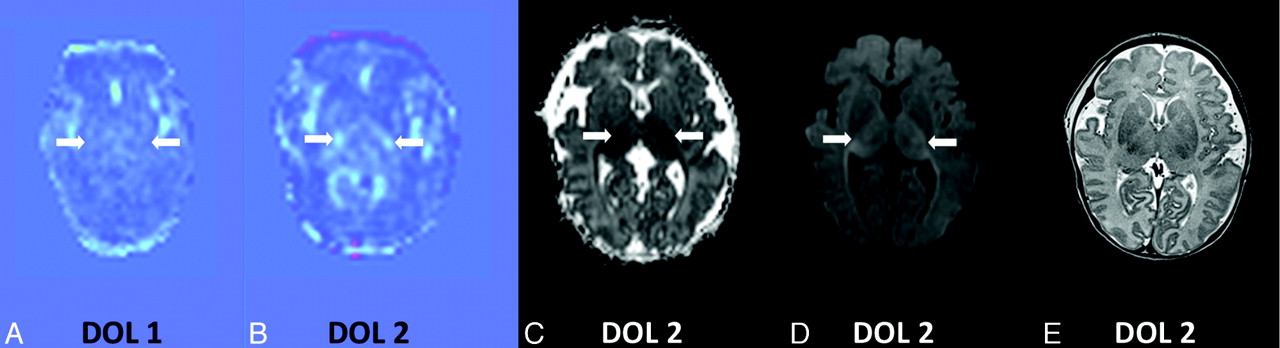
Brain MR imaging on DOL 2 in patient 8, while he was treated with induced hypothermia; comparison between the perfusion map and images obtained from conventional sequences. A and B, CBF maps obtained by perfusion imaging by ASL show decreased brain perfusion on DOL 1 (A) followed by increased brain perfusion on DOL 2 (B) in bilateral thalami, and relatively lower perfusion in GM and the remaining BG, compared with the control patient. C and D, ADC map (C) and DWI (D) on DOL 2 display restricted diffusion within bilateral thalami. E, Changes on T2-weighted imaging on DOL 2 are subtle.
In the neonates who were not treated with induced hypothermia but who developed HI brain injury, CBF values were increased in the injured brain areas during the first week of life. Increased CBF was already present on DOL 1 (as demonstrated in patient 12), seemed to peak around DOL 2–3, and, though less marked, persisted to the end of the first week of life. In these neonates, the brain regions that did not show any later brain injury displayed CBF values comparable with those in control patients. As with the infants who received hypothermia, these early findings of abnormal CBF predicted future injury on the later MR imaging.
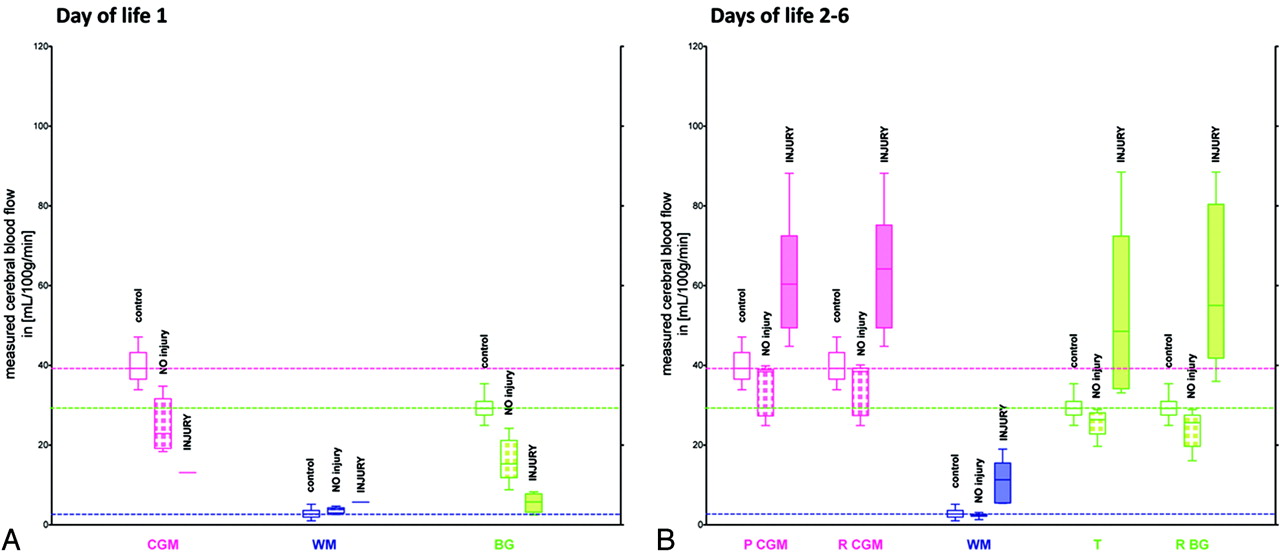
After adjustment for temperature and pCO2 (On-line Table 3), results from the regression model showed that brain perfusion values in the first week of life were significantly different in those neonates developing brain injury compared with those who did not. There was a significant difference between the injury and noninjury group in the different regions of interest on DOL 2–6 (P ≤ .0005 for each region of interest). Only comparison between means of CBF values is represented (Fig 5B), but comparisons between medians and quartiles of CBF values were also performed and yielded similar results. Similar analyses were difficult to perform on DOL 1, considering the small number of patients with brain injury, especially in the CGM and WM (Fig 5A); however, the same statistical significance was found for the BG area (P ≤ .0005) on DOL 1. The effect of FiO2 and hematocrit levels were nonsignificant after the inclusion of the presence or absence of injury, temperature, and pCO2 values. We were unable to control for ventilatory support, pressors, sedation, or antiepileptic treatment in the multiple regression model, due to the small sample size and the uniformity of treatment.
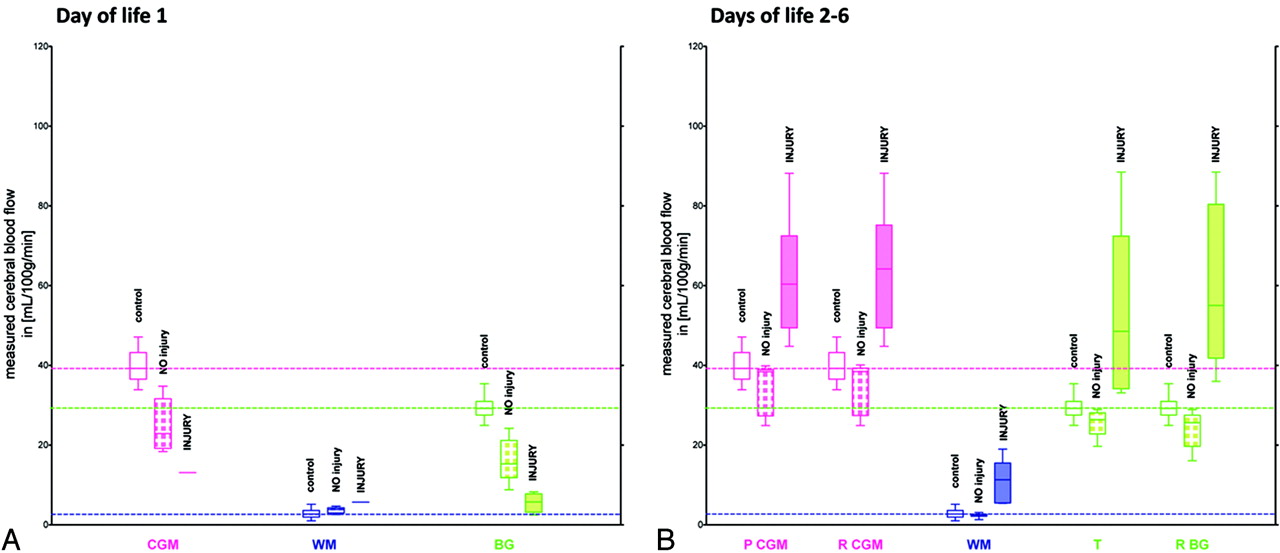
Comparison of means of CBF values in each region of interest between neonates developing brain injury in these regions of interest compared with those who did not, on DOL 1 (A) and on DOL 2–6 (B). Box-and-whisker plots (median, minimum, and maximum, in milliliters/100 g/minute) representation. The group of neonates developing brain injury is noted as the “INJURY” group, and the group of neonates who did not as “NO injury” group. The different regions of interest consist of the following: 1) CGM, including parietal CGM and remaining CGM with frontal and occipital cortical regions; 2) WM, including frontal and posterior WM and the centrum semiovale; 3) BG, including the thalamus and remaining BG with the lentiform nucleus and posterior limb of internal capsule. Dashed lines are drawn horizontally through the mean values of CBF in the CGM, WM, and BG of control neonates, to facilitate comparisons. Of note, CBF values of patient 12 are not included in the graph A, because this subject was the only asphyxiated neonate not treated with induced hypothermia; he presented with hyperperfusion on DOL 1. Patient 9 with BG injury in whom CBF was still decreased in the BG on DOL 2 is not included in the graph B because he was the only patient with persistent relative hypoperfusion on DOL 2.
Discussion
Lowering body temperature, as in therapeutic hypothermia, is thought to decrease CBF in patients with HIE.27 However, hypothermia alone does not account for all of the decrease in CBF values observed in our patients studied during hypothermia treatment. Our data suggest that the encephalopathy itself also decreases CBF. On DOL 1, CBF values were lower in neonates with HIE treated with hypothermia with an initial severely abnormal aEEG background who did not develop brain injury, compared with the ones with initial moderately abnormal aEEG background. On DOL 2, while they were still treated with induced hypothermia, those with an initial moderately abnormal aEEG background had similar CBF values compared with control patients. This finding suggests that the therapeutic value of induced hypothermia may not depend on any effect on regional CBF. Moreover, neonates with an initial severely abnormal aEEG background who did not develop brain injury had still lower CBF values on DOL 2 and became similar to control patients only on DOL 3. This finding suggests that the severity of encephalopathy has an important effect on brain perfusion in the first DOLs, as demonstrated in animal data.28 A better understanding of the degree to which the severity of the HIE influences brain perfusion and of the relation between brain perfusion and brain activity measured by aEEG would be useful. ASL-PI performed in these neonates just before initiation of hypothermia and repeated shortly after the beginning and again later during treatment might improve understanding of the effect of hypothermia on brain perfusion in asphyxiated neonates.
In our study, CBF values on DOL 1 were decreased in the brain areas that were later found to be injured. These CBF findings were evident earlier than changes observed with conventional MR imaging modalities because the brain injury in these 5 patients was not evident on the first DOL by conventional sequences. In addition, patient 9, who developed brain injury in bilateral BGs despite hypothermia treatment, had persistently low CBF values on DOL 2. Of interest, conventional sequences and DWI also performed in this patient on the same day were initially read as having negative findings; subtle abnormalities in BG were only retrospectively identified after reviewing later imaging.
The significance of the hypoperfusion observed in the first DOLs in our study remains unclear. This initial hypoperfusion phase has been previously observed in some asphyxiated neonate humans29 not treated with hypothermia. In animals, this transient hypoperfusion phase has also been described after HI. Its onset time and duration become earlier and longer respectively as the severity of the insult is increased.30 It is debated whether this hypoperfusion phase exacerbates future brain injury31,32 or protects the brain due to the reduced metabolic demand.33,34 The protective theory is one of the physiologic bases behind induced hypothermia treatment, which is intended to prolong the state of reduced metabolic demand.11 It is also possible that these hypoperfused regions represent areas of immediate neuronal death not amenable to neuroprotective therapies, because induced hypothermia can only prevent secondary or delayed neuronal death.35 It is also known that brain perfusion changes during the first 24 hours of life and might be very different at 6 compared with 24 hours of life or later.29 Given the small number of neonates with injured areas on DOL 1, the lack of normal measurements with this technique in healthy neonates during the first DOL, and the wide range in hours of the MR imaging in our patient population, there is insufficient evidence to conclude that this hypoperfusion might be used for early determination of neonates at risk for developing brain injury despite hypothermia treatment, as suggested by some animal studies.36
On DOL 2–3, the asphyxiated neonates developing brain injury despite hypothermia treatment displayed hyperperfusion in the brain areas subsequently exhibiting injury, in a very similar way to that in the asphyxiated neonates not treated with hypothermia who developed brain injury.15 The cause of this hyperperfusion is unknown, though experimental data suggest roles for nitric oxide, free radicals, adenosine, and prostaglandins.1 This state of vasodilation and vasoparalysis is most likely a marker of tissue injury.37 Our results suggest that early hyperperfusion correlates with later brain injury even in infants treated with induced hypothermia. Therefore this finding might be used to help identify or predict future brain injury in asphyxiated neonates undergoing hypothermia treatment. In our study, when hyperperfusion was found early in the course of neonatal HIE, systemic cooling for 72 hours appears not to have prevented future brain injury. It is currently unclear whether induced hypothermia can mitigate further brain injury11 when this hyperperfusion is present. In our study, hypothermia was associated with a smaller increase of CBF in patients 10 and 11, who developed bilateral thalami injury, compared with patient 15, who was not treated with induced hypothermia and who also developed injury in the bilateral BGs.
The natural history of this hyperperfusion phase is described here by brain perfusion measured in 7 asphyxiated neonates who did not receive induced hypothermia. Increased CBF was already present on DOL 1 in 1 patient, peaked around days 2–3 of life, and, though less marked, persisted through 1 week after delivery. These findings suggest that autoregulation of the CBF takes time to recuperate in the most severely infarcted areas.17 If the hyperperfusion stage persists for at least a week after the event and if induced hypothermia mitigates some of this hyperperfusion and extension of brain injury, perhaps induced hypothermia should be continued for longer than 72 hours or at lower temperatures than 33.5°C in patients with severe HIE demonstrating early hyperperfusion in areas of injured brain. Additional studies are needed to determine whether prolongation of hypothermia or deeper cooling could mitigate this hyperperfusion phase and prevent more secondary or delayed neuronal death.
These findings also raise the question of the timing of the transition between the hypoperfusion phase and the hyperperfusion phase. In some cases, induced hypothermia might prolong the duration of this initial hypoperfusion phase and prevent delayed hyperperfusion.11,33,34,38 Patient 8 with generalized brain injury already had hyperperfusion on his second scan, even though he was scanned sooner, on DOL 2, than patient 9. Thus if a transition time does exist, it may differ according to the different patterns of HI injury13,15 and the specific timing, duration, or severity of the HI at birth.
Ours is one of only a few studies measuring brain perfusion with ASL-PI in neonates.24 It is the only such study of brain perfusion in neonates with HIE, to our knowledge. Compared with other methods of measuring brain perfusion, including Doppler sonography, near-infrared spectroscopy, positron-emission tomography, or xenon-enhanced CT, only ASL-PI permits the direct assessment of CBF values in different areas of the brain without injecting contrast. Absolute measurements, despite their known limitations,20,39 permit the noninvasive assessment of perfusion in different regions of interest of neonate brains, as well as comparison among the neonates. The distribution of CBF in the CGM, WM, and BG obtained in the control term neonates showed higher brain perfusion in CGM and BG compared with WM. This is in general accordance with previous measurements in neonates by using other approaches.15,24,37,40⇓–42 However, the current limitation of the quantitation by this method might be that some of the labeling persisted in the major arteries in neonates (as demonstrated in our figures), and the entire label may thus not have reached the imaging plane, limiting the accuracy of the results. The current results in asphyxiated neonates treated with induced hypothermia show the feasibility of the ASL method and support the addition of ASL-PI to current imaging sequences in these patients.
Conclusions
ASL-PI performed during the first week of life in term asphyxiated neonates shows that an initial hypoperfusion phase followed by a hyperperfusion phase in specific brain regions is correlated with the development of brain injury in those regions, despite treatment with induced hypothermia. Furthermore, 72 hours of induced hypothermia at 33.5°C may not prevent injury when hyperperfusion is found early in the course of neonatal HIE. The value of ASL-PI for identifying asphyxiated neonates already undergoing hypothermia treatment who are at risk of developing brain injury and who might be ideal candidates for adjustments in their hypothermia therapy or for adjunctive neuroprotective therapies should be further assessed, as well as its potential role for tailoring the neuroprotective strategies to the specific clinical and imaging findings of individual patients to improve the future neurodevelopmental outcome.
Acknowledgments
We thank Joseph J. Volpe, MD, for his scientific advice and support, and the families and their neonates participating in the study. A special thank you is also expressed to the nurses in the neonatal intensive care unit and the MR imaging technicians, who have made this study possible.
Footnotes
-
Pia Wintermark receives research grant funding from the William Randolph Hearst Fund Award and the Thrasher Research Fund Early Career Award Program. The work of Simon K. Warfield is supported by National Institutes of Health grants R01 RR021885, R01 GM074068, R03 EB008680,and P30 HD018655.
-
Paper previously presented in part as posters at: 4th International Conference on Brain Monitoring and Neuroprotection in the Newborn, February 20–22, 2009; Orlando, Florida (a description of the first studied case) and 17th Scientific Meeting and Exhibition of the International Society for Magnetic Resonance in Medicine, April 18–24, 2009; Honolulu, Hawaii (a feasibility of ASL in newborns, use of a 32-channel coil); Annual Meeting of the Pediatric Academic Societies, May 2–5, 2009; Baltimore, Maryland (hyperperfusion on DOL 2, first results); and 50th Annual Meeting of the European Society for Paediatric Research, October 9–12, 2009; Hamburg, Germany (hypoperfusion on DOL 1, first results), but this work has not been published previously.
-
Disclosures: The authors have no conflict of interest to disclose affecting the content of this article.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received January 11, 2011.
- Accepted after revision April 17, 2011.
- © 2011 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Long-term consequences of neonatal encephalopathy in the hypothermia era: protocol for a follow-up cohort study at 9 years of age
- Anoxic Brain Injury Detection with the Normalized Diffusion to ASL Perfusion Ratio: Implications for Blood-Brain Barrier Injury and Permeability
- Cerebral Perfusion Is Perturbed by Preterm Birth and Brain Injury
- Brain Temperature Is Increased During the First Days of Life in Asphyxiated Newborns: Developing Brain Injury Despite Hypothermia Treatment
- Brain Perfusion Imaging in Neonates: An Overview
- Medial Occipital Lobe Hyperperfusion Identified by Arterial Spin-Labeling: A Poor Prognostic Sign in Patients with Hypoxic-Ischemic Encephalopathy
- Acquisition Guidelines and Quality Assessment Tools for Analyzing Neonatal Diffusion Tensor MRI Data
- Brain Perfusion in Encephalopathic Newborns after Therapeutic Hypothermia