
Abstract
BACKGROUND AND PURPOSE: CVR is a measure of cerebral hemodynamic impairment. A recently validated technique quantifies CVR by using a precise CO2 vasodilatory stimulus and BOLD MR imaging. Our aim was to determine whether preoperative CO2 BOLD CVR predicts the hemodynamic effect of ECIC bypass surgery in patients with intracranial steno-occlusive disease.
MATERIALS AND METHODS: Twenty-five patients undergoing ECIC bypass surgery for treatment of intracranial stenosis or occlusion were recruited. CVR was measured preoperatively and postoperatively and expressed as %ΔBOLD MR signal intensity per mm Hg ΔPetCO2. Using normative data from healthy subjects, we stratified patients on the basis of preoperative CVR into 3 groups: normal CVR, reduced CVR, and negative (paradoxical) CVR. Wilcoxon 2-sample tests (2-sided, α = 0.05) were used to determine whether the 3 groups differed with respect to change in CVR following bypass surgery.
RESULTS: The group with normal preoperative CVR demonstrated no significant change in CVR following bypass surgery (mean, 0.22% ± 0.05% to 0.22% ± 0.01%; P = .881). The group with reduced preoperative CVR demonstrated a significant improvement following bypass surgery (mean, 0.08% ± 0.05% to 0.21 ± 0.08%; P < .001), and the group with paradoxical preoperative CVR demonstrated the greatest improvement (mean change, −0.04% ± 0.03% to 0.27% ± 0.03%; P = .028).
CONCLUSIONS: Preoperative measurement of CVR by using CO2 BOLD MR imaging predicts the hemodynamic effect of ECIC bypass in patients with intracranial steno-occlusive disease. The technique is potentially useful for selecting patients for surgical revascularization.
Abbreviations
- ACA
- anterior cerebral artery
- AFNI
- Analysis of Functional NeuroImages
- BOLD
- blood oxygen level−dependent
- CBF
- cerebral blood flow
- CO2
- carbon dioxide
- CTA
- CT angiography
- CVR
- cerebrovascular reactivity
- DSA
- digital subtraction angiography
- ECIC bypass
- extracranial-intracranial bypass
- FiCO2
- inspiratory partial pressure of CO2
- FLAIR
- fluid-attenuated inversion recovery
- L
- left
- MCA
- middle cerebral artery
- MRA
- MR angiography
- OEF
- oxygen extraction fraction
- PaCO2
- arterial partial pressure of carbon dioxide
- PET
- positron-emission tomography
- PetCO2
- end-tidal partial pressure of carbon dioxide
- PetO2
- end-tidal partial pressure of oxygen
- R
- right
- STA
- superficial temporal artery
- TCD
- transcranial Doppler
- TIA
- transient ischemic attack
A large population-based study1 in the United States found that 9%–15% of ischemic strokes are due to intracranial stenosis or occlusion. The proportion is even higher in Asian populations.2 Management of intracranial steno-occlusive disease is a challenge because most etiologies lack effective medical therapy.3,4 Surgical treatment, traditionally by ECIC arterial bypass, was popular until the EC/IC Bypass Study (1985)5 found no difference in stroke incidence between patients randomized to medical therapy versus surgical bypass. A critique of the ECIC Bypass Study was that patients were included on the basis of degree of angiographic stenosis, without specifically assessing for cerebral hemodynamic compromise. Assessment of cerebral hemodynamic compromise is important: For a given degree of angiographic stenosis, some patients have adequate collateral supply, while others lack sufficient collateral flow. Subsequent advances in brain imaging have improved our ability to identify the latter group.
A recently validated6 technique for measuring CVR uses precise changes in PetCO2 as a vasodilatory stimulus and BOLD MR imaging to map the stimulus-induced changes in CBF. This technique uses an MR pulse sequence that is standard on clinical MR imaging systems, and it can be performed at the same session as routine MR imaging and MRA. Some groups7–9 have measured CO2 BOLD CVR by using the contralateral hemisphere as an internal standard and have reported quantitative right-left interhemispheric asymmetry indices. This kind of relative measure is necessarily problematic in patients with bilateral disease. It has previously been shown6 that expression of hemispheric CVR in absolute values (%ΔBOLD MR signal intensity per mm Hg ΔPetCO2), rather than as an interhemispheric asymmetry index, correlates well with CVR measured by using arterial spin-labeling MR imaging.
Our aim was to determine whether preoperative CO2 BOLD CVR, expressed in absolute values, predicts the hemodynamic effect of surgical bypass in patients with intracranial steno-occlusive disease. We hypothesized that patients with normal preoperative CVR would not improve in CVR following bypass, those with reduced preoperative CVR would improve, and those with markedly reduced CVR (ie, negative or paradoxical CVR) would have the greatest improvement.
Materials and Methods
Patients
The institutional ethics committee approved the study protocol, and all patients provided written informed consent. There were no study-related adverse events. Patients scheduled for ECIC bypass surgery for treatment of intracranial steno-occlusive disease at the Toronto Western Hospital (Toronto, Ontario, Canada) were recruited. Twenty-five consecutive patients (16 women, 9 men; mean age, 39.6 years ± 14.5) were recruited between August 2006 and January 2010. Seven patients had bilateral bypass procedures during the study period, resulting in a total of 32 ECIC bypasses. Patient demographics, clinical presentations, and diagnoses are listed in the Table.
Patient characteristics
Surgical Procedure
The most common surgical procedure (31/32) was direct ECIC bypass by end-side anastomosis of the STA to an MCA branch. In patients with small recipient MCA branches, this direct bypass was supplemented (7 procedures) with pial synangiosis, which is an indirect bypass performed by opening the arachnoid and attaching a branch of the STA to the pia mater. Two procedures consisted of indirect bypass only: 1 was a pial synangiosis and 1 was an encephalodural arterial synangiosis.
Vasodilatory Stimulus
PetCO2 and PetO2 were controlled by using model-based prospective end-tidal gas targeting.10 These algorithms are incorporated into a device (RespirAct; Thornhill Research, Toronto, Ontario, Canada) that consists of a computer-controlled gas blender, sensors for PCO2 and PO2, and a sequential rebreathing circuit applied to the patient. The user enters the target end-tidal gas values and their durations. The RespirAct system then uses the algorithm10 to calculate the various gas concentrations and flows it will administer to the breathing circuit to attain the target end-tidal gas partial pressures. The RespirAct system is capable of inducing precise square-wave changes in PetCO2 and PetO2, independently of each other over a wide range of minute ventilation and breathing patterns. The gas sequence for CVR was 8 minutes 20 seconds. Iso-oxia (target PetO2 of 100 mm Hg) was maintained throughout. The target PetCO2 was the following: 1) 40 mm Hg for 60 seconds (normocapnia), 2) 50 mm Hg for 60 seconds (hypercapnia), 3) normocapnia for 100 seconds, 4) hypercapnia for 160 seconds, and 5) normocapnia for 120 seconds.11 Tidal PCO2 and PO2 were monitored continuously, digitized, and recorded (RespirAct).
Imaging
MR imaging was performed on a 3T whole-body scanner (Signa HDx; GE Healthcare, Milwaukee, Wisconsin) with an 8-channel phased-array head coil for signal reception. Each patient was imaged with an identical CO2 BOLD CVR protocol preoperatively and postoperatively. Each CVR session included routine clinical acquisitions (sagittal T1-weighted, axial T2-weighted, axial T2-weighted FLAIR, and diffusion-weighted), an axial T1-weighted 3D spoiled gradient-echo acquisition (matrix size, 256 × 256; section thickness, 2.2 mm; intersection gap, 0) for anatomic coregistration, and an axial T2*-weighted single-shot gradient-echo echo-planar BOLD acquisition (flip angle, 85°; TR, 2000 ms; TE, 30 ms; FOV, 24 × 24 cm; matrix size, 64 × 64; section thickness, 5 mm; intersection gap, 2 mm; number of frames, 255) during controlled changes in PetCO2.
As part of their routine clinical care, all patients with direct ECIC bypasses also underwent postoperative imaging to assess bypass patency. This imaging was a combination of CT angiography (23/30 bypasses), MR angiography (12/30), and conventional angiography (10/30). Imaging to assess bypass patency was performed on the same day as postoperative CVR for 9/30 bypasses and both before and after the postoperative CVR for 13/30 bypasses. For the latter cases, one may infer bypass patency at the time of CVR if the bypass was patent on both the pre-CVR and post-CVR vascular studies. In the remaining 8/30 cases, patency was only assessed prior (mean, 4.0 ± 1.7 months) to the postoperative CVR. Mean time from assessment of vessel patency to postoperative CVR was 4.0 ± 1.7 months for these 8 patients. There was no suspicion of bypass nonpatency on clinical follow-up in any of these 8 patients.
Data Analysis
MR imaging and PetCO2 data were imported into the software AFNI (National Institutes of Health, Bethesda, Maryland; http://afni.nimh.nih.gov/afni).12 An AFNI algorithm was used to calculate head motion for each BOLD MR imaging acquisition. Bypass procedures (4/32) with >1 voxel-width head motion on either the preoperative or postoperative CVR study were excluded from further analysis. Each patient's whole-brain BOLD MR signal-intensity dataset was temporally shifted to the point of maximum correlation with the patient's PetCO2 waveform. The BOLD MR signal-intensity-time waveform then underwent least-squares fitting to the PetCO2-time waveform on a voxel-by-voxel basis, and CVR was calculated as %ΔBOLD MR signal intensity per mm Hg ΔPetCO2. Anatomic images were automatically segmented into gray matter and white matter and transformed into Montreal Neurologic Institute space by using the software SPM8 (Wellcome Department of Imaging Neuroscience, Institute of Neurology, University College, London, United Kingdom; http://www.fil.ion.ucl.ac.uk/spm/software/spm8). Anatomic images were further segmented into ACA, MCA, and posterior circulation (including the cerebellum) by using masks created from the atlas of Kretschmann and Weinrich.13 Mean gray matter CVR was calculated for each of these segments, for each CVR study.
The preoperative and postoperative routine T1- and T2-weighted images were reviewed to identify regions of parenchymal infarction or hemorrhage. Using AFNI, we created a mask of each region of parenchymal abnormality and generated a second set of CVR maps with these regions segmented. Clinical reports from postoperative CTA, MRA, and DSA were also reviewed, and each bypass was categorized as patent or nonpatent.
Statistical Analysis
To determine whether ECIC bypass had a significant effect on CVR, we performed a Wilcoxon 2-sample test (2-sided, α = 0.05) comparing preoperative and postoperative CVR values for each of the 6 vascular territories. Then, to determine whether preoperative stratification of patients by absolute CO2 BOLD CVR values predicts the hemodynamic effect of bypass surgery, we categorized patients on the basis of preoperative CVR in the territory of planned surgical bypass. Patients were categorized into 3 groups: 1) normal CVR, 2) reduced CVR, and 3) paradoxical CVR (that is, negative CVR). In a previous study,14 an identical CO2 BOLD CVR technique was used to study a group of 10 healthy subjects (mean age, 30.0 ± 8.2 years). In that study, mean CVR in the MCA territory was 0.30 ± 0.07 (%ΔBOLD MR signal intensity per mm Hg PetCO2). Because these data were approximately age-matched with the current study population, we used 2 SDs below the mean CVR from the healthy subjects as a threshold for reduced CVR. The lower threshold CVR value was 0.16% ΔBOLD MR signal intensity per mm Hg ΔPetCO2. We performed Wilcoxon 2-sample tests (2-sided, α = 0.05) to determine whether the change in CVR following ECIC bypass was significant for each of the 3 groups, and we also tested whether the change in CVR following ECIC bypass differed significantly between the healthy versus reduced CVR groups and reduced versus paradoxical CVR groups. All statistical analyses were then repeated for the CVR maps with regions of infarction or intraparenchymal hemorrhage removed. We also performed a Wilcoxon 2-sample test to look for a difference in preoperative CVR between those subjects who had direct bypass only versus those who received direct and indirect bypass.
Results
Median time from baseline CVR measurement to bypass procedure was 14.6 weeks (interquartile range, 13.5 weeks). Median time from bypass procedure to follow-up CVR measurement was 21.9 weeks (interquartile range, 9.5 weeks).
Bypass procedures excluded from the analysis were those associated with excessive head motion on a CVR study (4/32), nonpatent bypass (6/32), and a moderate-sized postoperative subdural hematoma (1 patient). The details of the 6 nonpatent bypasses are as follows: 1 bypass (patient 15) had already been excluded from the analysis due to head motion. One bypass (patient 1) was indeterminate for patency because the bypass was patent on an immediate postoperative CTA, postoperative CVR study was performed 2 months later, and the bypass was nonpatent on a CTA 2 months following the CVR. One bypass (patient 17) showed extremely delayed passage of contrast through the STA on DSA, with severe disease of the MCA M2 and M3 branches resulting in lack of retrograde flow into the MCA. Bilateral bypasses in a single patient (patient 13) showed significant stenosis at the arterial anastomoses. One bypass (patient 11) was occluded at the time of follow-up CVR.
There was no significant difference in preoperative CVR between subjects who received direct ECIC bypass only versus those who received direct and indirect bypass (mean, 0.09% ± 0.10% versus 0.09% ± 0.08%, respectively; P = .857).
Effect of ECIC Bypass on CO2 BOLD MR imaging CVR
CVR in the vascular territory of the surgical bypasses improved significantly following treatment (mean, 0.09% ± 0.10% prebypass to 0.22% ± 0.08% postbypass; 2-sided P < .001). CVR in the other vascular territories did not change significantly. Figure 1 shows these summary results, and Fig 2 is a representative case (patient 24). Repeating the analysis with regions of infarction or hemorrhage removed from the CVR maps did not significantly alter these results.

Graph shows the effect of ECIC bypass on CO2 BOLD CVR in gray matter vascular territories ipsilateral and contralateral to the bypass. Whiskers mark the 10th and 90th percentiles, and boxes are bounded by the 25th and 75th percentiles.

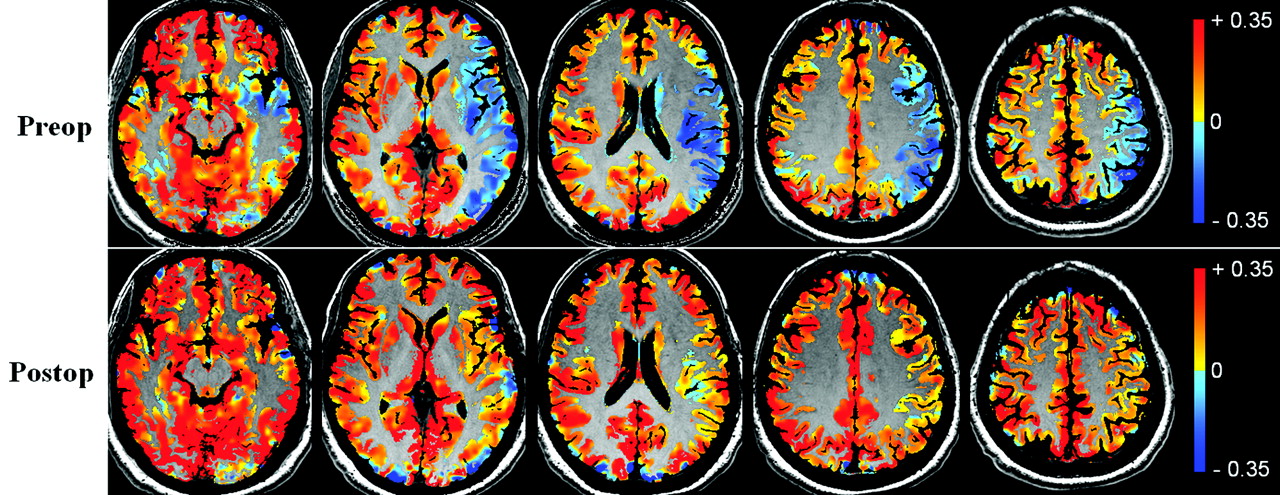
Gray matter CVR map overlaid on anatomic T1-weighted images for a representative patient (patient 24). Top row is before bypass, and bottom row is after bypass surgery. CVR units are %ΔBOLD MR signal intensity per mm Hg ΔPetCO2. Images demonstrate decreased, and in fact paradoxical (negative), CVR in the left MCA territory cortex and deep gray matter before bypass and marked improvement postbypass surgery.
Preoperative CVR as a Predictor of the Hemodynamic Effect of ECIC Bypass
Defining “reduced CVR” as 2 SDs below the mean CVR of approximately age-matched healthy subjects resulted in 5 patients with normal CVR, 12 patients with reduced (but positive) CVR, and 4 patients with paradoxical (negative) CVR. The group with normal preoperative CVR demonstrated no significant change in CVR following bypass surgery (mean, 0.22% ± 0.05% to 0.22% ± 0.01%; P = .881). The group with reduced preoperative CVR demonstrated a significant improvement following bypass surgery (mean, 0.08% ± 0.05% to 0.21 ± 0.08%; P < .001), as did those with paradoxical preoperative CVR (mean change, −0.04% ± 0.03% to 0.27% ± 0.03%; P = .028) (Fig 3 ). The differences in CVR improvement between the normal-versus-reduced preoperative CVR groups and between the reduced and paradoxical preoperative CVR groups were both significant (P = .012 and P < .001, respectively). Repeating the analysis with regions of infarction removed from the CVR maps yielded no significant change in the results.

Boxplots show the change in ipsilateral MCA territory CVR following ECIC bypass surgery for 3 groups: normal preoperative CVR, reduced preoperative CVR, and paradoxical preoperative CVR. Units of CVR are %ΔBOLD MR signal intensity per mm Hg ΔPetCO2.
Discussion
In this study, we found that CO2 BOLD CVR, expressed in absolute values, predicted the hemodynamic effect of ECIC bypass. Patients with normal preoperative CVR did not improve in CVR following bypass, those with reduced preoperative CVR did improve, and those with paradoxical preoperative CVR had the greatest improvement. These results have 2 main implications: First, they further validate the use of absolute CO2 BOLD CVR values for the measurement of cerebral hemodynamic compromise. Second, they suggest that absolute values from CO2 BOLD CVR are potentially of use in determining which patients with intracranial steno-occlusive disease should undergo surgical revascularization.
Quantitative Assessment of Hemodynamic Impairment Using CO2 BOLD CVR
We have expressed CVR in absolute values of %ΔBOLD MR signal intensity per mm Hg ΔPetCO2. This approach was validated in a study6 that compared BOLD MR imaging and arterial spin-labeling MR imaging measurements of CVR in 25 patients with steno-occlusive disease. This differs from much of the published CO2 BOLD CVR work7–9 that used the contralateral hemisphere as an internal standard and reported CVR as a right-left interhemispheric asymmetry index. Use of an interhemispheric asymmetry index is problematic because patients commonly have bilateral disease—that is, no normal hemisphere for normalization. We will briefly discuss a few methodologic details that may be important for obtaining absolute values of CO2 BOLD CVR.
First, is it necessary to normalize %ΔBOLD MR signal intensity to the magnitude of the vasodilatory stimulus? Goode et al8 suggested that use of a strong CO2 challenge yields near-maximal vasodilation and removes the need for normalization. Hypothetically, a CO2 stimulus sufficiently strong to cause near-maximal vasodilatory capacity in all patients could enable measurement of cerebrovascular reserve. However, the 40- to 50-mm Hg PetCO2 range typical of a CVR study is unlikely to consistently result in complete exhaustion of vasodilatory reserve. CBF continues to increase in response to incremental increases in PetCO2 well above 60 mm Hg in many subjects.15 In those patients in whom the CO2 stimulus does not result in complete exhaustion of vasodilatory capacity, %ΔBOLD MR signal intensity depends on the magnitude of the CO2 stimulus; thus, CVR must be expressed as a slope: ΔBOLD MR signal intensity / ΔPetCO2.
Second, how does one measure the magnitude of the CO2 stimulus? The independent variable affecting CBF is the PaCO2, but measurement of PaCO2 requires arterial puncture, which is uncomfortable for the patient. Instead, we have noninvasively measured its surrogate,16 PetCO2. With the end-tidal gas-targeting system that we used, PetCO2 correlates well with PaCO2.17 Some have used the FiCO2 as the independent variable, but the ventilatory response to hypercapnia varies between subjects, so FiCO2 does not have a consistent relationship with PaCO2.18
Third, if one normalizes %ΔBOLD MR signal intensity to the magnitude of the vasodilatory stimulus, is it necessary to maintain a consistent magnitude of vasodilatory stimulus for all subjects? The relationship between CBF and PaCO2 is sigmoidal. If only 2 points on the curve are taken (PaCO2 at 2 levels), then the slope (ie, the CVR) will depend on both the initial PaCO2, and the magnitude of the change in PaCO2.14,19 Therefore, to have comparable CVR measurements in 1 subject with time or between subjects, one must establish a consistent baseline PaCO2 and a consistent magnitude of change.
Finally, consider the “BOLD MR signal intensity” term. BOLD MR imaging is an indirect measure of changes in CBF. Increased CBF results in dilution of intravascular deoxyhemoglobin, generating increased signal intensity on T2*-weighted (BOLD) images. BOLD MR signal intensity also depends on cerebral blood volume, cerebral metabolic rate of oxygen consumption, PaO2, and hematocrit20 on pulse-sequence parameters such as TE and voxel size and on hardware factors such as magnetic field strength. Despite the many influences on absolute BOLD MR signal intensity, it has been shown empirically that with a tightly controlled CO2 stimulus and a single MR imaging scanner with consistent sequence parameters, hemispheric CVR measured in absolute values of %ΔBOLD MR signal intensity per mm Hg ΔPetCO2 is both precise21 and accurate.6 The technique does not provide a measure of CVR in the criterion-standard CBF units of mL/100 g/min, but it does enable quantitative intra- and intersubject comparisons.
Quantification within subjects may enable accurate follow-up of patients who are not surgically revascularized and measurement of treatment response in those who are revascularized. Quantification may allow the establishment of CVR thresholds to guide treatment decisions.
Absolute Values of BOLD CVR to Select Patients for Surgical Revascularization
To determine which patients with intracranial arterial steno-occlusive disease should undergo surgical revascularization, one aims to identify the subset of patients with cerebral hemodynamic impairment. The most widely studied imaging markers of cerebral hemodynamic compromise are increased OEF measured by PET and impaired cerebrovascular reactivity, most commonly measured by single-photon emission tomography, xenon-enhanced CT, or transcranial Doppler sonography.22 A major trial currently under way, the North American Carotid Occlusion Surgery Study,23 uses increased OEF on PET to select patients for ECIC bypass. PET measurement of OEF is accurate, and the results of this trial are highly anticipated, yet clinical translation of PET OEF may remain a challenge due to limited availability, high cost, and the requirement for an on-site cyclotron to produce the very short-lived radiopharmaceutical oxygen 15 (half-life 2 minutes). Our results suggest that absolute values of CO2 BOLD CVR are potentially useful in identifying a subset of patients with intracranial steno-occlusive disease who are most likely to have a hemodynamic improvement following surgical revascularization. The CO2 BOLD MR imaging technique is quick and nonionizing, and it can be performed at the same session as routine MR imaging and MRA.
Limitations
Several bypass procedures were excluded from the quantitative analysis: those with excessive head motion (4/32), nonpatent bypass (6/32), and a moderate-to-large postoperative subdural hematoma (1 patient). We have found that patient head motion during BOLD MR imaging acquisition is the most common reason for a failed CO2 BOLD CVR examination. In this study, we used an automated tool to exclude BOLD acquisitions with excessive head motion. Our analysis for head motion was performed after the MR imaging was complete, but it is possible to analyze BOLD MR imaging data in real-time. Analysis of head motion while the patient is in the MR imaging scanner would allow one to repeat those CVR acquisitions with head motion, potentially reducing the number of failed examinations. Nonpatent bypasses were excluded because we wanted to study the relationship between CO2 BOLD CVR and ECIC bypass, and nonpatent bypasses would confound the results. Future randomized controlled trials by using CO2 BOLD CVR as a means of selecting patients for randomization will likely require an intention-to-treat analysis, with patients in the surgical arm included regardless of whether the bypass procedure is technically successful.
An inclusion criterion for the study was the presence of intracranial stenosis or occlusion. We did not have a sufficient number of subjects to perform subgroup analyses on the various specific causes of stenosis or occlusion. There was also some variability in surgical treatments, with direct surgical bypass in 31/32 procedures and indirect bypass in 8/32. This could confound the study results if the subjects with lower preoperative CVR had a greater likelihood of receiving more extensive revascularization. However, there was no significant difference in preoperative CVR between those who received direct bypass only versus direct and indirect bypass.
A limitation was the assessment of ECIC bypass patency by using a clinically dictated schedule of CTA, MRA, and DSA. In most cases (22/30 direct bypass procedures), patency was assessed on the same day as the postoperative CVR or both before and after the postoperative CVR, enabling one to infer vessel patency if the bypass was patent on both studies. In a minority of patients (8/30 direct bypasses), patency was only assessed before the CVR study. All 8 of these latter patients had patent bypasses on imaging, and none had clinical suspicion of bypass nonpatency, but we cannot completely exclude the possibility of bypass occlusion between the time of patency assessment and the postoperative CVR study.
We have used an atlas-based segmentation of vascular territories into ACA, MCA, and posterior distributions. A limitation of this approach is that vascular territories may have altered size and geometry in patients with severe cerebrovascular disease. The atlas-based approach does still allow assessment of CVR near the region of the MCA bypass, versus farther from the bypass on the ipsilateral side, versus contralateral to the bypass.
Conclusions
CVR measured by using CO2 BOLD MR imaging identifies those patients with intracranial steno-occlusive disease who are more likely to have a hemodynamic improvement following ECIC bypass surgery. The CO2 BOLD MR imaging technique is quick and nonionizing, and it can be performed at the same session as routine MR imaging and MRA.
Acknowledgments
We thank Marat Slessarev and Alex Vesely for their contributions to the development of the breathing apparatus. We thank the Toronto Western Hospital MR imaging technologists, particularly Eugen Hlasny, David Johnstone, and Keith Ta, for their contributions to the data acquisition. We are grateful for the support of the Radiologist Scientist Training Program, Department of Medical Imaging, University of Toronto.
Footnotes
-
D.M.M. was supported by the American Society of Neuroradiology Foundation Scholar Award in Neuroradiology Research 2010–2011.
-
Paper previously presented at: Annual Meeting of the American Society of Neuroradiology, May 15–20, 2010; Boston, Massachusetts.
References
- Received July 29, 2010.
- Accepted after revision September 2, 2010.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Estimating Flow Direction of Circle of Willis Using Dynamic Arterial Spin-Labeling MR Angiography
- Improved White Matter Cerebrovascular Reactivity after Revascularization in Patients with Steno-Occlusive Disease
- Identifying Significant Changes in Cerebrovascular Reactivity to Carbon Dioxide
- Impaired Cerebrovascular Reactivity Predicts Recurrent Symptoms in Patients with Carotid Artery Occlusion: A Hypercapnia BOLD fMRI Study
- Assessing the effect of unilateral cerebral revascularisation on the vascular reactivity of the non-intervened hemisphere: a retrospective observational study
- Multimodal Markers of Inflammation in the Subcortical Ischemic Vascular Disease Type of Vascular Cognitive Impairment
- Acute Stroke Imaging Research Roadmap II
- Imaging Brain Oxygenation with MRI Using Blood Oxygenation Approaches: Methods, Validation, and Clinical Applications
- Novel MRI Approaches for Assessing Cerebral Hemodynamics in Ischemic Cerebrovascular Disease