
Abstract
SUMMARY: A 52-year-old man presented with subacute thyroiditis and showed an intensely hypermetabolic thyroid lesion on 18F-FDG PET/CT. The patient also had coexisting chronic lymphocytic thyroiditis. The lesion of subacute thyroiditis revealed an SUVmax of 9.1 g/mL and was ill-defined, heterogeneous, markedly hypoechoic, and hypovascular on US. Biopsy demonstrated histologic findings of subacute thyroiditis, which should be included in the differential diagnosis of an intensely hypermetabolic thyroid lesion on 18F-FDG PET/CT.
Abbreviations
- 18F-FDG PET/CT
- [18F] fluorodeoxyglucose whole-body positron-emission tomography and CT
- FDG
- fluorodeoxyglucose
- US
- sonography
- PD
- power Doppler
- PTC
- papillary thyroid carcinoma
- SUVmax
- maximum standardized uptake value
- US-FNAB
- sonography-guided fine-needle aspiration biopsy
Subacute thyroiditis is an uncommon inflammatory disease of the thyroid gland that occurs most often in middle-aged women. It is usually preceded by an upper respiratory tract infection and is presumed to be caused by a viral infection. A postviral inflammatory response leads to giant cell infiltration into the thyroid follicles, ultimately resulting in follicular swelling, which in turn results in stretching of the thyroid capsule with subsequent pain and tenderness on palpation, symptoms that are characteristic clinical features of this illness.1 It is a self-limited illness, which often resolves spontaneously. Thyroid US is useful for the initial diagnosis and follow-up of patients with subacute thyroiditis.2,3
Thyroid lesions identified by combined 18F-FDG PET/CT can create a dilemma for both patients and physicians; the probability of malignancy in thyroid focal uptake on 18F-FDG PET/CT ranges from 14% to 63%.4,5 Diffuse FDG uptake can be an indicator of chronic lymphocytic thyroiditis,6 which can also present as focal FDG uptake, mimicking thyroid malignancy.7 Cases of subacute thyroiditis presenting as diffuse FDG uptake have also been reported8,9; however, focal FDG uptake in the case of subacute thyroiditis has not appeared in the English literature, to our knowledge.
We report a case of subacute thyroiditis presenting as an intensely hypermetabolic thyroid lesion on 18F-FDG PET/CT, along with findings at US and US-FNAB that mimicked a malignancy of the thyroid gland, in a patient with coexisting chronic lymphocytic thyroiditis.
Case Report
A 52-year-old man was referred to our department for further evaluation of an incidentally identified hypermetabolic mass in the right thyroid lobe on 18F-FDG PET/CT. Physical examination was unremarkable except for a tender palpable mass at the right anterior neck. Approximately 17 days prior, he was admitted to our medical center for 2 days for general aches and mild febrile sensation. Findings of his thyroid function test and serum radioimmunoassay were normal except for elevated antithyroglobulin antibodies (153.7 IU/mL [normal, <70 IU/mL]). An 18F-FDG PET/CT was performed for cancer screening, which showed an intensely hypermetabolic mass with an SUVmax of 9.1 g/mL in the right thyroid lobe (Fig 1), which had not been present on the previous 18F-FDG PET/CT performed 20 months earlier. Background thyroid parenchyma showed mild diffuse FDG uptake in both thyroid lobes, which suggested chronic lymphocytic thyroiditis (Fig 1).
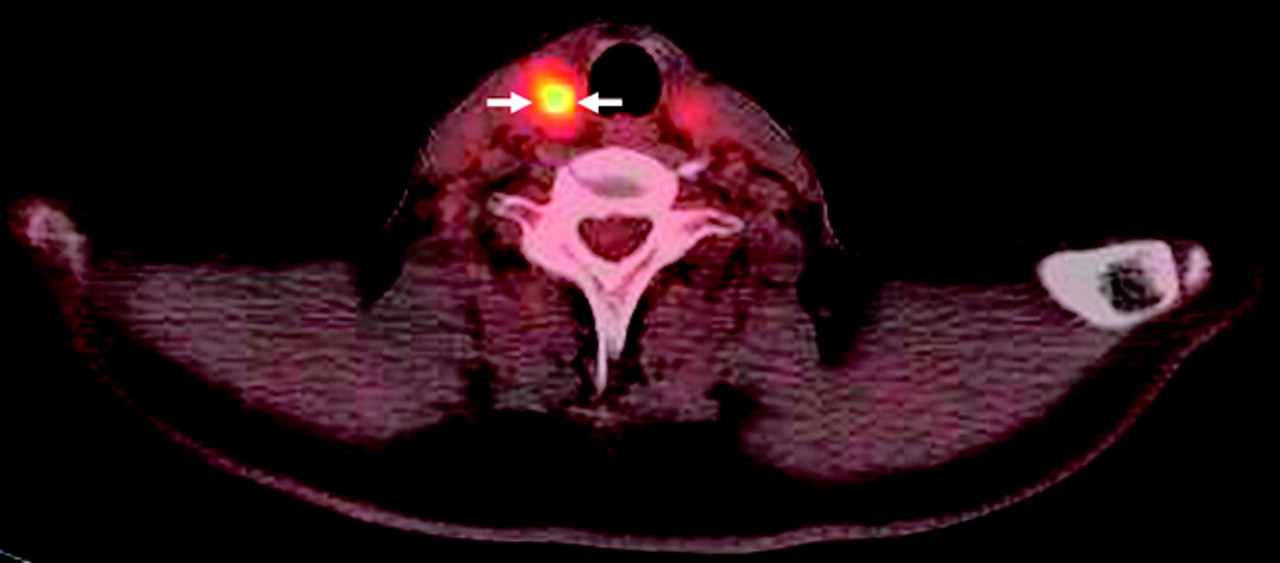
18F-FDG PET/CT image demonstrates an intensely hypermetabolic mass (SUVmax = 9.1 g/mL) in the right thyroid lobe (arrows). Background thyroid parenchyma shows mild diffuse FDG uptake.
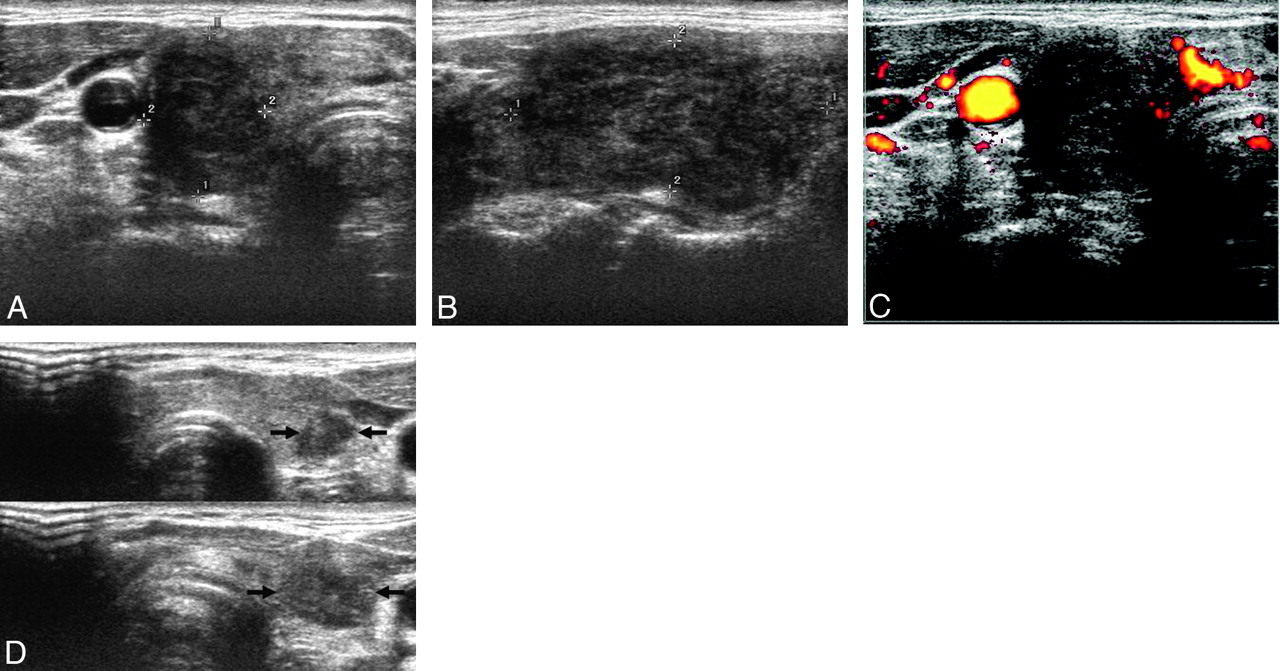
Thyroid US, performed 1 day after the 18F-FDG PET/CT examination, demonstrated an approximately 21 × 19 × 37 mm mass in the right thyroid lobe (Fig 2A−C), the location of which coincided with the hypermetabolic focus on 18F-FDG PET/CT. The mass was ill-defined, markedly hypoechoic, and heterogeneous, with scattered hyperechoic areas on gray-scale US (Fig 2A, -B), and was hypovascular compared with the background parenchyma on PD US (Fig 2C). Tenderness was noted just on compression of the mass. These sonographic findings suggested subacute thyroiditis. In addition, 2 small focal ill-defined markedly hypoechoic nodular lesions were present in the left thyroid lobe (Fig 2D). They could not be distinguished from background thyroid parenchyma that showed mild diffuse FDG uptake on 18F-FDG PET/CT. We performed US-FNAB of the right thyroid mass because the patient and referring physician were anxious about the newly developed intensely hypermetabolic focus on 18F-FDG PET/CT and because we could not definitively exclude infiltrative malignancies such as PTC or primary thyroid lymphoma.

A, Transverse gray-scale US reveals a markedly hypoechoic mass with a taller-than-wide shape in the right thyroid lobe (delineated by electronic calipers). B, A longitudinal gray-scale US shows an ill-demarcated heterogeneous mass with scattered hyperechoic areas (delineated by electronic calipers). C, A transverse PD US demonstrates hypovascularity of the mass compared with the background thyroid parenchyma. D, Split transverse gray-scale USs show 2 small focal ill-defined markedly hypoechoic nodular lesions in the left thyroid lobe (arrows).
US-FNAB was also performed on the 2 small nodular lesions of the left thyroid lobe to exclude PTC. The results of US-FNAB of the right and left thyroid lesions were consistent with subacute thyroiditis (Fig 3A) and chronic lymphocytic thyroiditis (Fig 3B), respectively.

A, Photographs of the cytologic examination of the specimen obtained by US-FNAB of the right thyroid mass show several multinucleated giant cells (arrows) with the background of smaller inflammatory cells, consistent with subacute thyroiditis (Papanicolaou, original magnification ×200). B, Photomicrograph of the cytologic examination of the specimen obtained by US-FNAB of 1 of the 2 left thyroid nodules reveals a lymphoid tangle (arrow) in the background of small lymphoid cells, suggestive of chronic lymphocytic thyroiditis (Papanicolaou, original magnification ×200).
Discussion
In subacute thyroiditis, the clinical and laboratory data are usually sufficient for making the diagnosis, and biopsy is rarely indicated. Our case presented a clinical dilemma because of unexpected focal, newly developed, intense FDG uptake of the lesion of subacute thyroiditis on 18F-FDG PET/CT, which raised clinical concern about thyroid malignancy.
Focal FDG uptake in the thyroid gland is likely caused by malignancy.10 However, focal FDG uptake may also be attributed to several benign conditions, including nodular hyperplasia, Hürthle cell and follicular neoplasms, and even chronic lymphocytic thyroiditis.7,10
Subacute thyroiditis can involve 1 or both lobes of the thyroid gland diffusely or focally.11 Several reports concerning US features of subacute thyroiditis have been published in the English literature.2,3 In a study of 27 patients with subacute thyroiditis,2 unilateral thyroid involvement was demonstrated in 23 and bilateral involvement, in 4 patients. All the lesions were ill-defined and hypoechoic. Nine patients had a hypoechoic nodular lesion with an irregular or microlobulated margin, which mimicked thyroid carcinoma. No hypervascularity was noted in any of the lesions on color or PD US. Zacharia et al3 reported the utility of color Doppler US in a case of subacute thyroiditis that mimicked thyroid carcinoma clinically. They reported that color Doppler US showed no hypervascularity at the acute stage and slightly increased vascularity at the recovery stage.
Two cases of subacute thyroiditis with diffuse hypermetabolism on 18F-FDG PET, involving a single lobe and both lobes of the thyroid gland, respectively, have been reported.8,9 However, cases of subacute thyroiditis with focal hypermetabolism have not appeared in the English literature. Our case represents the first of subacute thyroiditis that showed focal hypermetabolism on 18F-FDG PET/CT, mimicking a thyroid malignancy. In view of clinical and US features, subacute thyroiditis was suggested as a probable diagnosis. However, because the patient and referring physician were anxious about the newly developed intensely hypermetabolic focus on 18F-FDG PET/CT and because we could not definitively exclude infiltrative malignancies such as PTC and primary thyroid lymphoma, we proceeded to US-FNAB. The results of cytologic examination were consistent with subacute thyroiditis. In addition, 2 small nodular lesions of the left thyroid lobe proved to be chronic lymphocytic thyroiditis by US-FNAB.
Thus, this case represents coexistence of subacute thyroiditis and chronic lymphocytic thyroiditis. Interestingly, the lesion of subacute thyroiditis showed intense hypermetabolism, while the lesions of focal chronic lymphocytic thyroiditis were not significantly hypermetabolic compared with the background parenchyma. We hypothesized that the intense hypermetabolism of the lesion of subacute thyroiditis might be caused by active inflammation, while the lesions of focal chronic lymphocytic thyroiditis might be relatively quiescent; thus they did not show hypermetabolism on 18F-FDG PET/CT.
In conclusion, subacute thyroiditis should be included in the differential diagnosis of focal FDG uptake on 18F-FDG PET/CT. Gray-scale and PD US are useful for the characterization of this lesion, and US-FNAB can provide a definitive diagnosis of subacute thyroiditis that presents as an intensely hypermetabolic thyroid incidentaloma on 18F-FDG PET/CT.
References
- Received September 24, 2009.
- Accepted after revision December 2, 2009.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.