
Abstract
SUMMARY: The HVS on FLAIR imaging is a useful marker of acute ischemic stroke. We investigated whether prior administration of gadolinium-based contrast hindered detection of this sign on images from subjects with acute nonlacunar ischemic stroke <4.5 hours after onset. Both blinded and comparative unblinded analyses showed significantly reduced HVS detection on postcontrast images. We suggest that assessment for this sign should be performed on images acquired prior to contrast administration.
ABBREVIATIONS:
- BA
- blinded analysis
- CA
- comparative analysis
- FLAIR
- fluid-attenuated inversion recovery
- HVS
- hyperintense vessel sign
- NIH
- National Institutes of Health
- NINDS
- National Institute of Neurological Disorders and Stroke
The HVS describes hyperintensity of the cerebral arteries ipsilateral to an arterial occlusion when visualized on FLAIR imaging. It is, therefore, a useful imaging marker of acute ischemic stroke.1,2 Although precise mechanisms have not yet been elucidated, angiographic findings suggest that the pathophysiology of this sign is likely to involve either arterial occlusion or retrograde flow via collateral vessels, static blood, or slow flow.1⇓–3 At proximal locations, FLAIR HVS is likely to represent arterial occlusion, and a report from our group suggested a sensitivity of 65.9%.4 At distal locations, however, the sign may be a marker for collateral flow; a further study5 suggested that subjects with the HVS in distal vessels had milder baseline neurologic deficits and a trend toward smaller subacute lesions. Given that HVS is assessed frequently in both clinical and research settings, detection should be optimized to be as sensitive as possible. However, our experience in the acquisition of postcontrast FLAIR images suggested that their sensitivity may be less than that in such images acquired before contrast administration. We aimed to clarify this issue.
Materials and Methods
A retrospective analysis was performed on an institutional review board−approved prospectively collected dataset (Natural History of Stroke Protocol). Subject inclusion criteria for this study were the following: 1) acute nonlacunar ischemic stroke, 2) <4.5 hours from stroke onset, and 3) good quality pre- and postcontrast FLAIR images from the same examination. Some of these subjects have been included in a previous publication.5 Images were acquired from 2 hospitals affiliated with our institution, and details of image acquisition have been previously reported.5 The analysis of images was performed in 2 ways: First, 1 observer (K.A.D.) reviewed all pre- and postcontrast FLAIR images while blinded to clinical and other imaging data and without knowledge of which images were performed after contrast (BA). This analysis was performed blinded to minimize observer bias. Each FLAIR image was dichotomously graded for the presence or absence of an HVS at sites proximal and distal to the Sylvian fissure. For each site, a 2 × 2 contingency table describing the presence or absence of HVS on pre- and postcontrast images was constructed. Next, StatsDirect (Version 2.7.2, http://www.statsdirect.com) was used to perform the McNemar test with Yates correction to elicit differences in the proportion of HVS detected in precontrast images compared with postcontrast images. Next, the Fisher exact test was used to compare the proportion of cases of HVS in which contrast affected detection in proximal and in distal locations.
Next, a CA was performed to simulate clinical image reads. For this analysis, pre- and postcontrast image pairings were reviewed together, while the reviewers were unblinded to other imaging data. The presence or absence of HVS on pre- and postcontrast images was noted, in addition to recording of cases in which there was a subjective reduction in HVS intensity but without complete disappearance of the sign. In a similar manner to that in the BA, images were graded for the continued presence (persistent or reduced HVS) or absence of HVS after contrast. Statistical analysis was performed as per the BA.
Results
Of the 56 subjects who fulfilled the inclusion criteria, movement artifacts precluded analysis in 11 subjects. Of the remaining 45 subjects, BA revealed 23 (51%) subjects who demonstrated the presence of HVS on precontrast FLAIR. Of these, the HVS was present in 22 subjects proximally, in 19 subjects distally, and in both locations in 18 subjects. For the BA, disappearance of HVS after contrast was seen in 11/22 (50%) subjects proximally (P = .027) and 13/19 (68%) subjects distally (P = .003). The detection of HVS by BA in the post- but not precontrast FLAIR imaging occurred in only 2 subjects. There was no difference in the proportion of cases with HVS disappearance with respect to proximal and distal locations (P = .34). In the CA, HVS was present in 24 subjects proximally, 21 distally, and both proximally and distally in 19. HVS was undetected after contrast in 3/24 (13%) subjects proximally (P = .25) and 10/21 (48%) distally (P = .004). Although the difference between proximal and distal locations was statistically significant (P = .02), there was no difference between proximal and distal locations with respect to the proportion of cases in which contrast had any effect on the HVS (ie, a reduction in intensity or complete disappearance of the HVS): 16/24 (67%) subjects proximally and 15/21 (71%) subjects distally (P = .76, Fisher exact test). An example of HVS change with contrast is given in Fig 1.
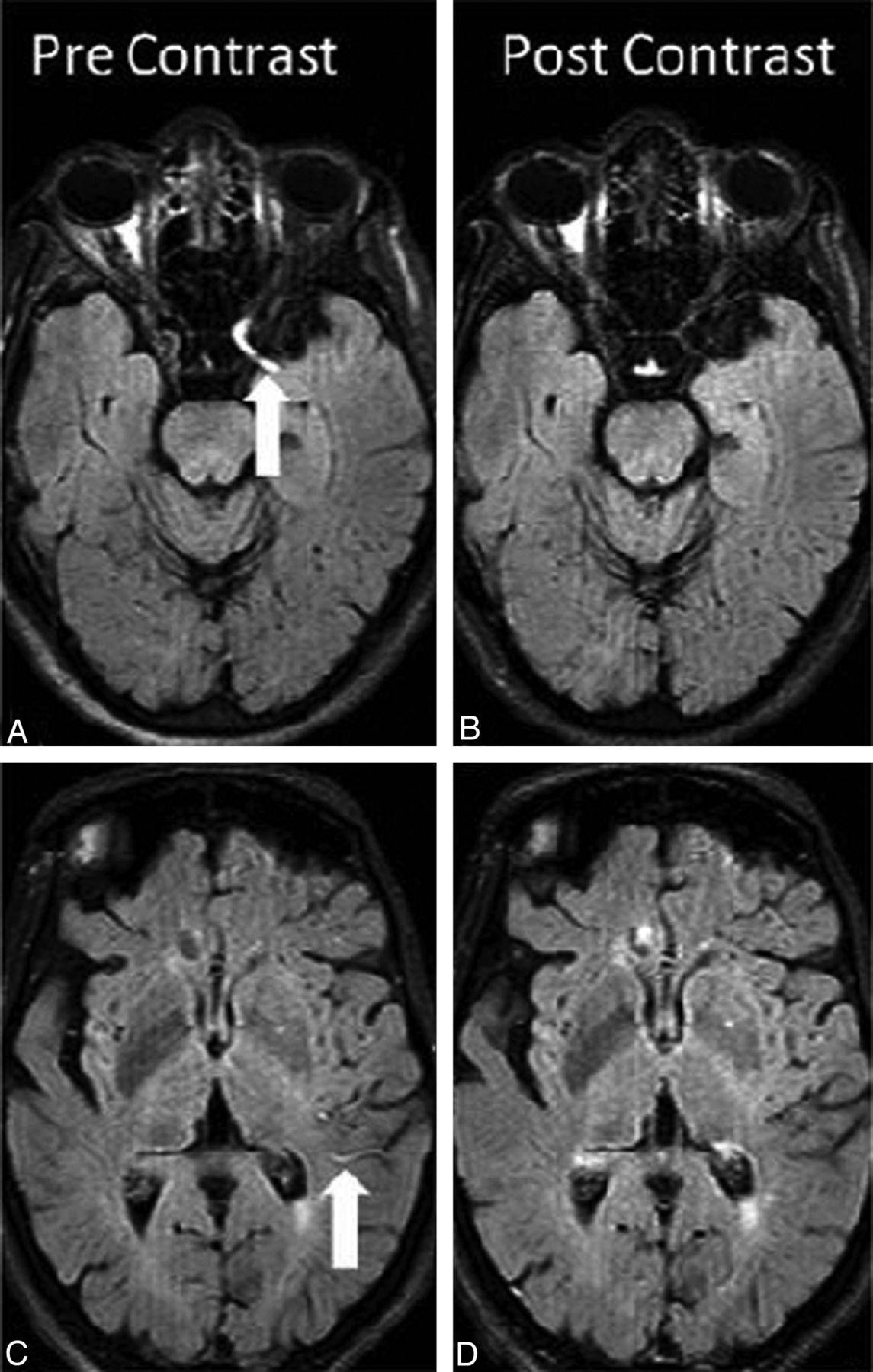
The HVS before and after gadolinium-based contrast. All images are from the same subject. A and C, Precontrast FLAIR images. The white arrow in A marks the proximal HVS, and the white arrow in C marks the distal HVS. B and D, The HVS is not detected in the postcontrast FLAIR images.
Discussion
The blinded analysis presented here demonstrates a significantly reduced rate of detection of the HVS after the administration of gadolinium-based contrast. These findings are consistent with the CA, which showed either a reduction in intensity or complete disappearance of HVS after gadolinium in most subjects. These findings are clinically important for 2 reasons: First, in concert with angiographic studies, the presence of HVS can potentially distinguish areas of slow flow from sites of arterial occlusion and, therefore, potentially highlight regions with collateral circulation, thus informing the clinician of the underlying tissue pathophysiology.5 Second, the value of postcontrast FLAIR examinations after stroke is increasingly being recognized; hyperintensity of CSF spaces (hyperintense acute reperfusion marker) seen on the postcontrast FLAIR imaging can suggest early breakdown of the blood-brain barrier. This sign is associated with hemorrhagic transformation and worse clinical outcome.6 Therefore, given the potential utility of postcontrast FLAIR images after acute ischemic stroke in clinical and research settings, neuroradiologists and neurologists should be aware of the optimal imaging conditions for detection of the HVS, which include assessment of FLAIR imaging performed before gadolinium-based contrast administration.
The cause of the postcontrast disappearance of the HVS is unclear. FLAIR images have both T1 weighting from the inversion recovery for CSF suppression and T2 weighting from a long TE. We can only speculate that the gadolinium in the vessels results in a shortening of T1 and T2 in such a way that the HVS effect is significantly decreased.
A number of limitations to this study should be acknowledged. First, we could not account for the volume or type of contrast agent used, which is likely to have varied between hospitals and across time. In addition, the FLAIR images analyzed in this study were acquired in a number of years, during which time acquisition parameters varied. In this study, we did not account for variations in TI, TE, and TR, which can all affect tissue contrast on FLAIR imaging. Section thickness and section gap thickness, which also vary between MR imaging stroke protocols, are likely to influence the detection of the HVS. Nonetheless, this heterogeneity reflects the range of routine clinical practice and, therefore, makes our observations all the more relevant. Furthermore, a particular strength of this study is that the pre- and postgadolinium FLAIR images were acquired contemporaneously (within a matter of minutes), by using exactly the same acquisition parameters, thus negating many of the potentially confounding effects of variations in acquisition parameters between examinations. Indeed, the aim of this study was to determine an effect of gadolinium in the detection of HVS, which we have successfully achieved. However, further analyses with larger numbers of subjects that examine concomitant MR angiographic findings are required to determine whether there is a difference in the effect of gadolinium on the HVS found due to arterial occlusion compared with that due to slow flow/collateral circulation, because this may explain the observed differences between proximal and distal locations.
Conclusions
Gadolinium reduces the detection of the HVS after ischemic stroke. We therefore suggest that if both pre- and postcontrast FLAIR examinations are acquired, the assessment of HVS is ideally performed on precontrast FLAIR, especially if comparisons between institutions are to be performed. Additional studies are required to determine the biologic significance of the “disappearing” HVS.
Acknowledgments
We thank Pat Lyall and Lizbeth Keller from the Section on Stroke Diagnostics and Therapeutics (NINDS) for assistance with data base searching.
Footnotes
Disclosures: Krishna Dani, Research Support (including provision of equipment and materials): Patrick Berthoud, Research Fellowship. The study was funded by the NIH. Details: The above fellowship provided salary and funds to travel to the NIH. This is a 3-year research training fellowship. Two years were spent at the University of Glasgow (UK) and 1 year at the NIH.
This work was supported by the Division of Intramural Research of the NIH and NINDS. Krishna Dani is supported by the Patrick Berthoud Charitable Trust.
Paper previously presented at: International Stroke Conference, February 23–24, 2010; San Antonio, Texas.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received June 21, 2010.
- Accepted after revision November 17, 2010.
- © 2012 by American Journal of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.