
Abstract
SUMMARY: Routine intensive care unit monitoring is common after elective embolization of unruptured intracranial aneurysms. In this series of 200 consecutive endovascular procedures for unruptured intracranial aneurysms, 65% of patients were triaged to routine (non-intensive care unit) floor care based on intraoperative findings, aneurysm morphology, and absence of major co-morbidities. Only 1 patient (0.5%) required subsequent transfer to the intensive care unit for management of a perioperative complication. The authors conclude that patients without major co-morbidities, intraoperative complications, or complex aneurysm morphology can be safely observed in a regular ward rather than being admitted to the intensive care unit.
ABBREVIATION:
- ICU
- intensive care unit
The number of unruptured intracranial aneurysms treated in the past 2 decades has increased with advances in endovascular techniques and imaging.1 This has resulted in increased hospital resource utilization and increasing costs.2 There are no guidelines as to the postoperative disposition of patients after endovascular coil embolization of unruptured intracranial aneurysms, yet intensive care unit (ICU) admissions are common after these procedures. We report the results of a policy of selective ICU admission after elective aneurysm treatment.
Materials and Methods
Institutional review board approval was obtained for data collection. A prospective, consecutive series of patients treated for unruptured intracranial aneurysms by the senior author was created. Information collected included patient demographics, presentation, aneurysm size, location, treatment, admission (floor or ICU), change of care level, 24-hour complications, and 30-day follow-up. Institutional protocols regarding postsurgical care are listed in the On-line Appendix. The senior author determined the disposition of each patient on the basis of criteria outlined in Table 1. Patient records were dichotomized to floor and ICU groups and compared. Continuous independent variables, including age, aneurysm size, and length of stay, were compared with unpaired Student t tests. Independent categoric values, including anterior circulation and presentation (incidental, unrelated SAH, or symptomatic), were compared by means of χ2 analysis.
Criteria for ICU Admission
Results
Two hundred consecutive endovascular embolization procedures for unruptured aneurysms were performed in 178 patients. After 131 (65.2% of 200) procedures, patients were admitted to a neurosurgical floor (Fig 1). After 69 (34.8%) of 200 procedures, patients were admitted to the ICU for the following reasons: intraoperative complications (n = 16, 23%), investigational device (n = 14, 20%), aneurysmal morphology (n = 26, 38%), and medical co-morbidities (n = 13, 19%). Among all the patients, 79% were women, 18% had aneurysms discovered after SAH from another aneurysm more than 30 days previously, 27% had symptomatic aneurysms, and 55% had incidental aneurysms (On-line Appendix). The most common locations were internal carotid (47%) and basilar (13%) arteries. Sixty-eight percent of the aneurysms were small, 25% large, and 7% giant. Treatments included coil embolization (62%) and Pipeline Embolization Device (Covidien, Irvine, California) (25.5%). Further information regarding aneurysm location and treatments are listed in the On-line Appendix.
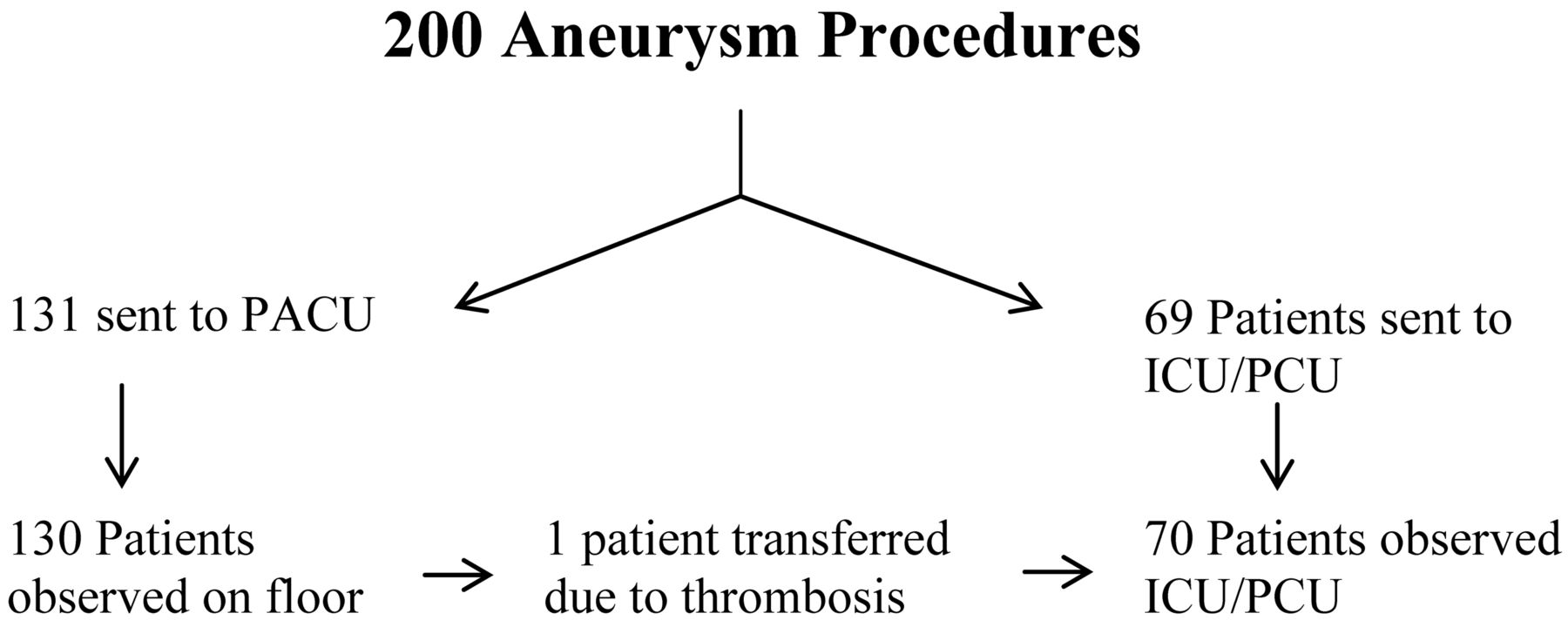
Disposition after endovascular treatment of unruptured aneurysms. PCU indicates Progressive Care Unit; PACU, Postoperative Recovery Unit.
Patients admitted to the ICU had larger aneurysms than those who went to the floor (12.6 ± 9.2 mm versus 7.7 ± 4.7 mm, P < .001). Patients admitted to the ICU were also more likely to have had symptomatic aneurysms than patients admitted to the floor (37.7% versus 21.3%, χ2 = 4.43, P = .0353) (Table 2). Admission to the ICU also led to significantly longer lengths of stay (1.1 versus 1.5 days, P = .026).
Floor versus Intensive Care Comparison
A change of admission status occurred after 1 (0.8%) of 131 procedures. This patient had undergone coiling of an anterior choroidal aneurysm, recovered to her baseline postoperatively, and developed an acute hemiparesis in the recovery unit. The angiogram revealed thrombosis of the anterior choroidal artery, which was reversed with abiciximab. Another complication within 24 hours was seen in a patient originally admitted to the ICU and discharged the following day who had noncardiac chest pain that was evaluated in the emergency department. Neither of these patients had permanent morbidity at 30-day follow-up.
Two patients of 200 (1%) had morbidity persistent at 30 days. One was admitted to the ICU after intraoperative aneurysm rupture. Another patient was admitted to the floor and discharged the next day but had a thromboembolic stroke on postoperative day 4. There were no significant differences in early (24-hour) complications resulting in permanent morbidity between the floor and ICU groups (0.8% versus 1.9%, P = .56).
Overall, 88% of complications were apparent in the angiography suite, either during the procedure or on awakening from anesthesia, and 12% of complications developed during the first 24 hours. Further information regarding intraoperative and 24-hour complications is listed in the On-line Appendix.
Discussion
We have prospectively evaluated a policy of selective ICU admission in a consecutive, unselected population of patients undergoing endovascular treatment of unruptured intracranial aneurysms. Since adoption of this policy, >60% of patients were admitted to the floor, which has resulted in reduced utilization of specialized hospital resources. Only 1 patient required a change of admission status because of a deficit noted on admission to the neurosurgical ward. This event was promptly recognized, and the patient was treated without any untoward neurologic sequelae. Our study suggests that a large number of patients who undergo elective endovascular treatment of unruptured intracranial aneurysms do not need the specialized and intensive monitoring provided in an ICU environment. There were no complications seen among patients in the ICU admitted for aneurysmal morphology or investigational device reasons, perhaps indicating a more aggressive policy of admission to the floor is possible.
As shown by other authors, both thromboembolic and hemorrhagic complications are not infrequent during endovascular procedures for intracranial aneurysms but can be promptly recognized and treated in the angiographic suite, thus resulting in a low rate of permanent co-morbidity and mortality.3,4 In our series, most complications were evident during the procedure or on awakening from anesthesia.
There is limited information about the need and indications for ICU admission in patients undergoing elective endovascular procedures. Studies on neurosurgical patients after craniotomy have suggested that ICU care after craniotomy may not be necessary.5,6 Zimmerman et al7 conducted a multicenter analysis of 3000 patients admitted to ICU care for neurosurgical diseases and found that among patients who were only observed in the ICU, <10% were likely to need any ICU treatments. Their analysis highlighted the need for comprehensive admission guidelines to the ICU. Beauregard and Friedmann6 reported that 2 of 132 patients required ICU admission from the floor after craniotomy. Similarly, Bui et al5 reported 10 response calls among 343 elective craniotomy patients, none of which resulted in ICU transfer. Clearly, patients with some neurologic interventions can be safely observed in a general ward, and the safety of this practice among patients undergoing elective aneurysm treatment is shown for the first time in this study.
Our study has limitations. It is a single-center study, we did not include a cost-saving analysis, and the triaging criteria that we used have not been validated and were only carried out by the senior author. Admission of the selected patients to the ICU may have avoided a complication, and this is not accounted for in our analysis. However, none of the complications that could have been prevented by ICU admission (such as prompt recognition of new ischemic symptoms, hemodynamic instability in a patient with large access hematoma, or cardio-respiratory issues) occurred in our cohort of patients admitted to the ICU who were stable in the angiography suite and did not have intraprocedural events. It can also be argued that the rate of transfer to the ICU after floor admission would have been higher had all of the patients been admitted directly to a regular ward. However, as previously mentioned, there were no complications observed in the patients admitted to the ICU who were stable after awakening from anesthesia and who had had a “straightforward” procedure. Moreover, the paradigm presented may not be applicable in every center because patients are admitted to a regular floor or to the ICU, depending on the level of comfort with floor care, which is variable from center to center.
Conclusions
Serious complications after endovascular elective aneurysm treatment are most often evident during the procedure or immediately on awakening. The presence of intraoperative complications, complex aneurysm morphology, or severe medical comorbidities may predispose to ICU admission. In the absence of these complications or predisposing factors, patients may safely be observed on the floor.
Footnotes
Disclosures: Giuseppe Lanzino—UNRELATED: Consultancy: ev3/Covidien.* Alejandro Rabinstein—UNRELATED: Consultancy: Boehringer Ingelheim, Comments: Participation in a single advisory meeting; Royalties: Elsevier, Comments: Authored books. Harry Cloft—UNRELATED: Grants/Grants Pending: Cordis Endovascular.* David Kallmes—UNRELATED: Consultancy: ev3,* Medtronic,* Cordis*; Grants/Grants Pending: ev3,* MicroVention,* Codman,* Benvenue*; Payment for Lectures (including service on speakers bureaus): MicroVention*; Royalties: UVA Patent Foundation; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: MicroVention,* ev3.* (*money paid to institution).
REFERENCES
- Received November 27, 2012.
- Accepted after revision February 15, 2013.
- © 2013 by American Journal of Neuroradiology





{kind=link}
Jump to section
Related Articles
Cited By...
- Timing of complications during and after elective endovascular intracranial aneurysm coiling
- Is intensive care monitoring necessary after coil embolization of unruptured intracranial aneurysms?
- Current Trends and Results of Endovascular Treatment of Unruptured Intracranial Aneurysms at a Single Institution in the Flow-Diverter Era