
Abstract
BACKGROUND AND PURPOSE: 4D flow MR imaging is an emerging technique that allows visualization and quantification of 3D blood flow in vivo. However, representative studies evaluating its accuracy are lacking. Therefore, we compared blood flow quantification by using 4D flow MR imaging with US within the carotid bifurcation.
MATERIALS AND METHODS: Thirty-two healthy volunteers (age 25.3 ± 3.4 years) and 20 patients with ≥50% ICA stenosis (age 67.7 ± 7.4 years) were examined preoperatively and postoperatively by use of 4D flow MR imaging, with complete coverage of the left and right carotid bifurcation. Blood flow velocities were assessed with standardized 2D analysis planes distributed along the CCA and the ICA and were compared with US at baseline and postoperatively in patients. In addition, we tested reproducibility and interobserver agreement of 4D MR imaging in 10 volunteers.
RESULTS: Overall, 101 CCAs and 79 ICAs were available for comparison. MR imaging underestimated (P < .05) systolic CCA and ICA blood flow velocity by 26% (0.79 ± 0.29 m/s vs 1.06 ± 0.31 m/s) and 19% (0.72 ± 0.21 m/s vs 0.89 ± 0.27 m/s) compared with US. Diastolic blood flow velocities were similar for MR imaging and US (differences, 9% and 3%, respectively; not significant). Reproducibility and interobserver agreement of 4D flow MR imaging was excellent.
CONCLUSIONS: 4D flow MR imaging allowed for an accurate measurement of blood flow velocities in the carotid bifurcation of both volunteers and patients with only moderate underestimation compared with US. Thus, 4D flow MR imaging seems promising for a future combination with MRA to comprehensively assess ICA stenosis and related hemodynamic changes.
ABBREVIATIONS:
- CCA
- common carotid artery
- CE-MRA
- contrast-enhanced MR angiography
- ECA
- external carotid artery
- PC
- phase contrast
- US
- 2D duplex sonography
Digital subtraction angiography is the current reference method for the assessment of ICA stenosis,1 but less invasive techniques such as CE-MRA and CT angiography have emerged as reliable alternatives.2,3 A recent meta-analysis revealed a pooled sensitivity and specificity of CE-MRA of ca. 94% and 93%, respectively, indicating that accuracy is lower compared with DSA and US.2 In contrast to angiography, US provides limited morphologic information but detailed information regarding velocities at the carotid bifurcation and intracranial collateral blood flow.3,4 A combination of such information as one 3D dataset provided by 1 technique (eg, CE-MRA plus PC MR imaging), would allow for a comprehensive assessment of the carotid bifurcation.
Accordingly, carotid artery blood flow could be determined by use of time-resolved 2D PC MR imaging. It was recently used to quantify blood flow in the carotid and basilar arteries in healthy participants5 and in extracranial and intracranial vessels in patients with ICA stenosis.6 This approach, however, is restricted to single 2D planes and requires individual angulation of analysis planes perpendicular to the vessel lumen. 3D cine PC MR imaging with 3-directional velocity encoding (also termed 4D flow MR imaging) overcomes these limitations and was recently validated in a model of cerebral aneurysms with laser Doppler velocimetry and computational fluid dynamics.7 In vivo applications allow measurement and visualization of 3D blood flow at the arterial and venous vessels, the heart, and the liver.8⇓–10 Moreover, 4D flow MR imaging was applied to visualize complex 3D blood flow at the carotid bifurcation, analyze the shape of velocity-time curves, measure flow velocities at the CCA, and investigate the in vivo distribution of wall shear stress along the carotid bifurcation in volunteers and patients.11,12
Therefore, 4D MR imaging is an exciting imaging technique that provides a wide spectrum of potentially valuable information for clinical applications. However, data comparing the measurement accuracy of 4D flow MR imaging with sonography in vivo and in a larger number of normal and diseased vessels are sparse. Previous comparisons were conducted in the CCA of 8 volunteers11; the intracranial arteries of 5 volunteers and a patient13; and, recently, in the liver vessels of 61 participants.10 Therefore, our purpose was to test the performance of carotid 4D flow MR imaging compared with US in more than 100 carotid arteries of both healthy volunteers and patients with high-grade ICA stenosis undergoing examinations preoperatively and postoperatively. Moreover, we systematically evaluated reproducibility and interobserver agreement of 4D flow MR imaging in a subgroup of 10 healthy volunteers undergoing repeated MR imaging examinations.
Materials and Methods
Study Population
A total of 32 healthy volunteers (age, 25.3 ± 3.4 years; 16 women) without a history of cardiovascular disease participated in the study. Findings of wall shear stress distribution along the carotid bifurcation of these volunteers were described recently.12 In addition, 20 patients with ≥50% ICA stenosis as measured by 2D duplex-sonography according to NASCET criteria4 were included. Of these 20 patients, 19 underwent a recanalization procedure (stent implantation: n = 4, eversion carotid endarterectomy: n = 15) and were examined by MR imaging and US before and after the procedure. MR imaging and US were repeated in 10 of the healthy volunteers to test reproducibility. Our study was approved by the local ethics committee, and written informed consent was obtained from all participants.
MR Imaging Measurements
MR imaging measurements were performed on a 3T MR imaging system (Tim-Trio; Siemens; Erlangen, Germany) by use of a combined 12-element head and 6-element neck coil. For anatomic overview, 3D time-of-flight MRA in an axial slab covering the left and right carotid bifurcation was performed (flip angle, 25°; TE, 3.7 ms; TR, 20 ms; spatial resolution, 0.5 × 0.8 × 1.0 mm3; slab thickness, 114 mm).
In patients with a glomerular filtration rate >40 mL/m, we additionally performed CE-MRA. CE-MRA was executed before recanalization (and after recanalization in individual patients) after injection of 0.1 mmol/kg body weight gadolinium-based contrast agent (gadobenate dimeglumine; Multihance, Bracco, Italy) at 3.5 mL/s (voxel size, 0.8 × 0.6 × 0.7 mm3; field of view, 225 × 300 mm2; TE, 1.31 ms; TR, 3.11 ms; flip angle, 20°; bandwidth, 650 Hz/pixel). 4D flow MR imaging consisted of a prospectively electrocardiogram-gated radio-frequency-spoiled gradient-echo sequence with interleaved 3-directional velocity encoding.11 As shown in Fig 1, the predominantly axial 3D imaging volume was angulated based on the time-of-flight MRA data to include the CCA, the bifurcation, the ICA, and the ECA. Imaging parameters were as follows: flip angle, 15°; TE, 3.1 ms; TR, 5.7 ms; velocity sensitivity, 120 cm/s; spatial resolution, 1.1 × 0.9 × 1.4 mm3; slab thickness, 50.4 mm; number of sections/slab, 36; and temporal resolution, 45.6 ms. For patients with ICA stenosis, the velocity encoding was set to 200 cm/s to account for higher blood flow velocities.

Data acquisition strategy with use of 4D flow MR imaging in an oblique axial 3D slab, including both left and right carotid bifurcation. Time-resolved 3D PC data with 3-directional velocity encoding are obtained by synchronization of data acquisition with the cardiac cycle. For each timeframe, 1 reference scan and 3 velocity-sensitive scans are acquired to calculate blood flow velocities along all 3 spatial dimensions (vx, vy, vz).
Data Processing and Flow Quantification
Data processing included noise filtering, correction for eddy currents, Maxwell terms, and velocity aliasing as described previously.14 For each 4D flow MR dataset, a 3D PC-MRA was calculated and was visualized as a 3D isosurface as shown in Fig 2 (EnSight, CEI, Apex, North Carolina).15 Next, 7 analysis planes (planes 1–6 in ICA and 1 plane in the ECA) were positioned in the carotid bifurcation according to anatomic landmarks. Analysis plane 2 was anchored at the flow diverter point (branching point between the ECA and the ICA) and was angulated perpendicular to the ICA. All other analysis planes were generated by shifting the plane center upstream (ICA) or downstream (CCA) in 4-mm intervals. The ECA plane was positioned 4 mm above the flow diverter. Each plane was manually angulated perpendicular to the arterial lumen. For comparison with sonography, the velocities of the most distal ICA analysis planes were considered. Because of the expected inability of 4D flow MR imaging to resolve high blood flow velocities exceeding the velocity encoding of 200 cm/s, intrastenotic velocities in patients were not considered for analysis.

Pulsatile velocity-time curves for all evaluated analysis planes in the CCA, ICA, and ECA. The lines, data points, and error bars represent mean velocities and SDs averaged over 64 carotid arteries of the 32 healthy volunteers.
For blood flow velocity quantification, all planes were imported into a home-built analysis tool programmed in Matlab (Mathworks, Natick, Massachusetts).16 The location of the vessel walls were defined by manual outlining of lumen contours on all measured timeframes. For each analysis plane, the mean (averaged over the segmented lumen) and maximal absolute blood flow velocity-time curves were calculated. The time needed to complete the data processing workflow, including preprocessing, placement of analysis planes, and manual segmentation of the carotid lumen, was approximately 60–90 minutes.
Reproducibility, Interobserver, and Intraobserver Variability
We examined 10 healthy volunteers at 2 different times by MR imaging and US to test reproducibility (6-month time difference between scans 1 and 2). Interobserver agreement was evaluated by 2 independent observers for MR imaging measurements (observer 2 segmented luminal contours and was blinded to the results of observer 1).
In addition, reproducibility of maximal blood flow velocity (ie, peak systolic and end-diastolic velocities) at the CCA and ICA were measured by the same examiner at baseline, along with repeated sonography measurement in the same 10 volunteers.
Sonography Measurements
All participants were examined with a 7–12-MHz linear array scanner (Logiq 7; GE Healthcare, Milwaukee, Wisconsin) by 1 experienced sonographer who was blinded to MR imaging data. With the participant in the supine position, the carotid bifurcations of both sides were examined: CCAs at least 2 cm proximal to the bifurcation and in the distal ICA were examined. Maximal blood flow velocities in cm/s in peak systole and end-diastole were determined manually by means of electronic calipers for 5 heart cycles. The average value was taken for further analysis.
Hemodynamic Monitoring
After establishing stable values during rest and with the participants in the supine position for 10 minutes, we began measurements with the patients breathing normally. Parameters were recorded in 5-minute intervals and were averaged for comparison MR imaging of US. Heart rate, systolic and diastolic arterial blood pressures, and arterial oxygen saturation (%) were measured during MR imaging (Millennia 315MVS; In vivo Research, Orlando, Florida) and US (Dinamap GE Pro 300, Criticon; GE Healthcare).
Statistical Analysis
Data are presented as the mean ± SD for continuous variables. To detect statistically significant differences between continuous variables, paired t tests (hemodynamic data) or the Wilcoxon test was applied. Correlations between selected variables were estimated with the Pearson correlation coefficient. All tests were 2-sided and used a significance level of 5%. The comparison between maximal and mean blood flow velocities measured by Doppler US and MR imaging and of maximal velocities (peak systolic and end-diastolic at the CCA and ICA) between baseline and repeated sonography measurements was evaluated via the approach of Bland and Altman17 by calculation of the mean (d) and SD of the difference. From these data, the limits of agreement (±2 SDs) were calculated. All analyses were performed with Matlab and the SPSS statistical package (version 15.0; SPSS, Chicago, Illinois).
Results
Baseline Data and Hemodynamic Monitoring
Patient demographics are summarized in Table 1. Total scan time for 4D flow MR imaging was 15–20 minutes, depending on heart rate of the participants. In the 32 healthy volunteers, heart rate (67.5 ± 12.3 minutes vs 63.7 ± 9.1/minutes; P = .006) and arterial oxygen saturation (97.6% ± 0.7% vs 98.3% ± 1.1%; P = .01) were significantly different at the time of MR imaging vs US examination. No significant difference was detected between systolic and diastolic blood pressures. In the 20 patients, we observed no significant differences between heart rate, arterial oxygen saturation, or systolic or diastolic blood pressure.
Incidence of cardiovascular risk factors and degree of ICA stenosis
Carotid Blood Flow Velocities by Use of MR Imaging in Healthy Volunteers
Figure 2 shows blood flow velocities averaged over 64 carotid bifurcations in healthy volunteers for all analysis planes along the carotid bifurcation. Typical flow velocity-time curves and dampening of the flow curves during passage through the bulbic ICA region can clearly be appreciated. Also, the typically higher pulsatility of the CCA and the ECA compared with the ICA is demonstrated by the velocity-time curves.
As summarized in Fig 3, scan-rescan and interobserver analysis is confirmed by good reproducibility and low interobserver variability for MR imaging. In sonography, reproducibility was comparable to MR imaging, showing a 5.8% deviation between measurement 1 and measurement 2 for maximal systolic and diastolic blood flow velocities as obtained in the CCA and ICA, whereas MR imaging exhibited a deviation of 7.4%. The 95% limits of agreement for peak systolic and end-diastolic blood flow velocity in the CCA on sonography were mean 0.09 m/s (−0.22–0.40 m/s) and 0.04 m/s (−0.10–0.18 m/s), respectively. For the ICA, they were mean −0.00 m/s (−0.25–0.25 m/s) and 0.02 m/s (−0.06–0.09 m/s), respectively.

Reproducibility and interobserver variability of carotid blood flow velocity measurements by 4D flow MR imaging. A, Subsequent scan and data analysis for 10 healthy participants. B, Subsequent lumen segmentation and velocity calculation for the 10 volunteers. The data points reflect the measured mean and maximal blood flow velocities in all 7 analysis planes and for all measured timeframes.
Correlation of MR Imaging and Sonography
Overall, 101 carotid bifurcations were available for comparison of MR imaging with US: 64 normal carotid bifurcations of the 32 volunteers, 20 carotid bifurcations of patients with ICA stenosis, 15 carotid artery bifurcations after recanalization by endarterectomy and 4 carotid artery bifurcations after recanalization by endovascular treatment. In some of the patients, either MR imaging or US data were of insufficient image quality. In particular, this problem was apparent in the ICA of patients receiving stent insertion. Therefore, these carotid arteries were not considered. As a result, the number of carotid segments (ie, the ICA or CCA) that were compared in MR imaging vs US in systolic and diastolic blood flow velocities was variable (Figs 4 and 5, Table 2).
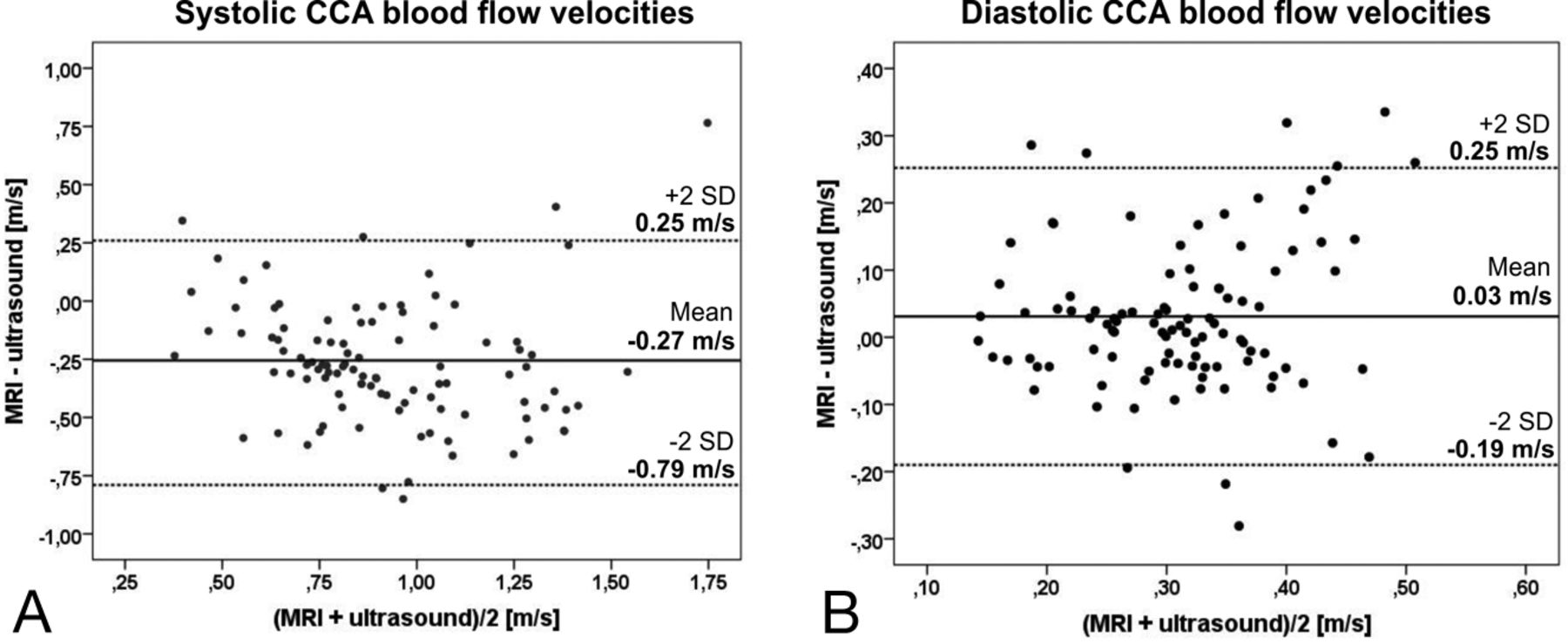
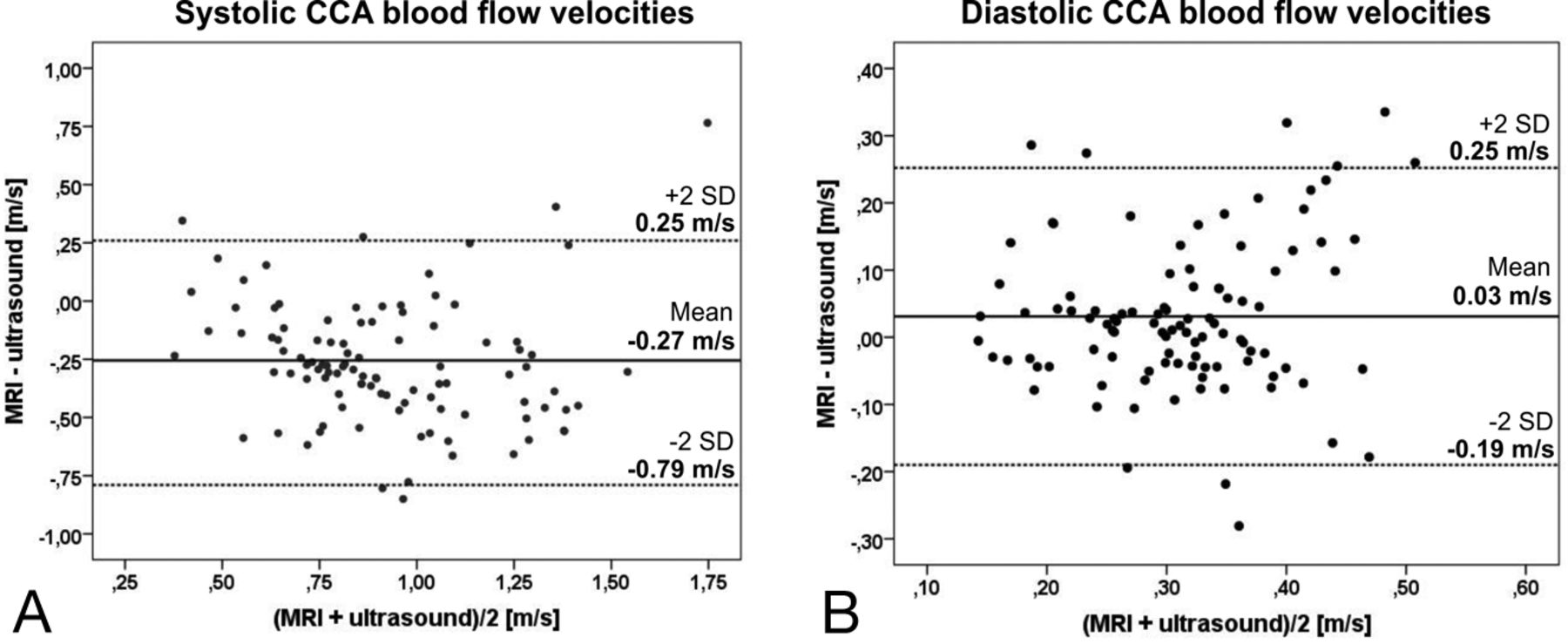
Bland-Altman plot of systolic (A) and diastolic (B) blood flow velocities within the CCA of volunteers and patients as measured by MR imaging vs sonography (n = 101 carotid arteries).

Bland-Altman plot of systolic (A) and diastolic (B) blood flow velocities within the ICA of volunteers and patients as measured by MR imaging vs sonography (n = 101 carotid arteries).
Comparison of systolic and diastolic blood flow velocities in MRI vs US in healthy volunteers (n = 34) and in the CCA and ICA of patients before (n = 20) and after (n = 19) recanalization
As summarized in Figs 4 and 5 and in Table 2, MR imaging significantly (P < .05) underestimated systolic blood flow velocity compared with US by 26% and 19% for the CCA and ICA, respectively (Figs 4 and 5, Table 2). Diastolic blood flow velocities of the CCA and ICA were slightly overestimated by MR imaging by 9% and 3%, respectively (not significant). The underestimation of MR imaging was observed for all velocities without evidence of a systematic bias in the Bland-Altman plots.
Discussion
4D flow MR imaging is an emerging method that provides the opportunity to visualize 3D blood flow in vivo in any larger artery or vein in the body. Previous studies have shown the potential of the technique to retrospectively quantify blood flow velocities or derived parameters, such as pulse wave velocities or wall shear stress.10⇓⇓–13,18 However, to date, no study with a large number of normal and diseased carotid arteries has evaluated the accuracy of 4D flow MR imaging compared with a reference method such as US in vivo.
In our study, more than 101 carotid arteries provided a wide spectrum of velocities for the evaluation of 4D flow MR imaging. Such imaging underestimated velocities in both the CCA and the ICA by 20%–25% and thus performed slightly better than described in previous studies performed on the carotid and intracranial arteries11,13,19 or on the hepatic veins,10 underestimating US by 30%–40% and 10%–50%, respectively. Peak systolic and end-diastolic blood flow velocities of the CCA in the 32 volunteers were similar to those in 8 healthy volunteers studied previously13 (systole: 0.72 m/s on MR imaging vs 0.87 m/s on US; diastole: 0.27 m/s on MR imaging vs 0.37 m/s on US). In addition, reproducibility and interobserver agreement for the manual lumen segmentation of 4D flow MR imaging data as tested in 10 healthy volunteers were excellent and confirmed accuracy in a recent study applying 4D flow MR imaging at the aorta.20 Thus, this technique shows high reproducibility and interobserver agreement, but absolute values are still lower compared with sonography as the reference method. Note that the interscan variability for peak velocities was characterized by a mean difference of 0.02 m/s and limits of agreement of ±0.18 m/s. Both are lower compared with the intermodality mean differences and limits of agreement shown in Fig 4 and 5, indicating the potential of 4D flow MR imaging to assess peak velocities.
MR imaging especially underestimated peak systolic blood flow velocities in the CCA and ICA. The difference of peak end-diastolic velocities between MR imaging and US, however, was low and on the order of ±10%. The underestimation of maximal systolic blood flow velocities by MR imaging is most probably caused by the limited spatial and temporal resolution of MR imaging of (1.1 mm)3/45 ms compared with approximately (0.3 mm)2/1.5 ms on sonography. Thus, it would be beneficial to further increase spatial and temporal resolution to increase the accuracy of future MR imaging applications and to be able to measure very high velocities. Another potential improvement would be the application of a dedicated neck coil positioned closer to the neck surface to improve signal-to-noise ratio of the acquired MR imaging data. It should be noted that the absence of significant differences between MR imaging and US for diastolic velocities may be related to the high velocity encoding (120–200 cm/s) that was used for data acquisition. In the case of low diastolic velocities, this may have resulted in higher velocity noise and, thus, a reduction in accuracy for diastolic velocities.
4D flow MR imaging based on retrospective flow quantification at the CCA, ECA, and multiple locations in the ICA revealed typical velocity-time curves that are very comparable to those known from sonography, described in a previous 4D MR imaging study11 and in a more recent 2D PC MR imaging approach by Gwilliam et al.5 In contrast to Gwilliam et al, we are able to cover the entire carotid bifurcation at a similar spatial resolution of (1.1 mm).3 An additional benefit compared with standard 2D-PC methods relates to the possibility of measuring flow velocities at any point of interest after MR measurement. Even coverage of the distal ICA or of the basilar artery could be achieved by tilting or enlarging the predefined 3D field of view as desired. In addition, blood volume flow can be measured by mean velocity and diameter change of the analysis plane with time (ie, approximately every 45 ms). Comparable with Gwilliam et al,5 we found differences in the velocity-time curves between the CCA and ICA in volunteers and between volunteers and patients.
Limitations
Limitations of carotid 4D flow MR imaging include the long measurement time of approximately 15–20 minutes and of approximately 60–90 minutes for preprocessing and postprocessing that is required to visualize or quantify 4D MR imaging raw data. As a result, this technique is not yet suited for clinical routine. However, current developments in parallel imaging allow data acquisition at the same resolution to be performed in less than 10 minutes, and new software prototypes that are currently under evaluation in our institutions are promising in improving the workflow of MR imaging data analysis.
Regarding methodologic improvements (higher resolution, reduced scan total time) of 4D flow data acquisition, future studies should investigate the potential of new multidimensional imaging acceleration techniques such as k-t undersampling or compressed sensing, which appear ideally suited for 4D flow MR imaging and would permit acceleration along multiple dimensions (3D space, time).21 Alternatively, different readout strategies such as spiral or radial k-space trajectories and their potential for more efficient data acquisition should be explored.22
It is currently challenging to accurately assess higher blood flow velocities at the site of ICA stenosis by using 4D flow MR imaging, leading to an underestimation of velocities in sonography in our current study. Compatible with this explanation, the difference of 4D flow MR imaging and US was less than the half for quantification of much lower diastolic blood flow velocities in the CCA and ICA (approximately 10%). Therefore, we did not compare maximal flow velocities within the stenosis between both techniques. However, maximal systolic velocities are 1 major criterion for hemodynamic evaluation of the impact of ICA stenosis in US. Thus, further significant improvement of temporal and spatial resolution of 4D MR imaging or, as an alternative, a combination with high-resolution single 2D PC-MR imaging measurements at the site of the ICA stenosis is needed to reliably measure high velocities by 4D MR imaging in the future.
The reproducibility of 4D flow MR imaging was high in healthy volunteers. However, it should be additionally tested in patients with high-grade ICA stenosis to determine whether it is also reliable and, thus, useful for future applications in patients with carotid artery disease.
The current comparison of 4D flow MR imaging with US as the reference method is, moreover, limited by the fact that velocities could not be exactly obtained at the identical region of the vessel. This is certainly less problematic for the straight CCA showing a relatively constant flow throughout the vessel course. Comparison at the ICA, especially at the ICA bulb or in patients with upstream stenosis and, thus, complex physiologic patterns at the bulb or poststenotic flow, is much more challenging because of the rapid change of flow patterns within a few millimeters. We tried to minimize such effects by measuring maximal flow velocities very distal to the dilated bulb or stenosis both on MR imaging and US. A future comparison, however, should also compare maximal intrastenostic velocities at the clearly defined stenotic region.
Clinical Perspective
The future improvement of measurement accuracy of CE-MRA and the combination with optimized 4D flow MR imaging would allow for a more comprehensive assessment of ICA stenosis. Such an MR imaging protocol could provide 3D information on flow, velocities, and wall shear stress at any desired location. Moreover, 4D flow MR imaging of extracranial and intracranial areas could be helpful to quantify blood flow in locations that are not accessible by sonography, such as the ICA siphon or intracranial arteries in case of an insufficient bone window.
Conclusions
4D flow MR imaging was tested in comparison with US in a larger cohort of healthy volunteers and patients with ICA stenosis. MR imaging underestimated US by 20%–25% but showed high reproducibility and interobserver agreement for data analysis in volunteers. 4D flow MR imaging is currently a time-consuming but promising technique that can be ideally combined with CE 3D MRA to study ICA stenosis more comprehensively and in vivo.
Acknowledgments
We thank Hansjörg Mast for performing MR imaging examinations.
Footnotes
Disclosures: Andreas Harloff—UNRELATED; Payment for Lectures: Boehringer Ingelheim. Cornelius Weiller—UNRELATED: Consultancy: GSK, Pierre Fabre; Payment for Lectures (including service on speakers bureaus): Pierre Fabre.
Grant support: Deutsche Forschungsgemeinschaft (DFG) Grant # HA 5399/3-1; NMH Excellence in Academic Medicine (EAM) Program “Advanced Cardiovascular MRI Research Center.”
Indicates open access to non-subscribers at www.ajnr.org
REFERENCES
- Received July 12, 2012.
- Accepted after revision October 2, 2012.
- © 2013 by American Journal of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Carotid webs produce greater hemodynamic disturbances than atherosclerotic disease: a DSA time-density curve study
- In-room assessment of intravascular velocity from time-resolved rotational angiography in patients with arteriovenous malformation: a pilot study
- Cerebral Veins-Why Functional MR Imaging is Worth the Trouble