
Abstract
BACKGROUND AND PURPOSE: Spontaneous intracranial hypotension can be a therapeutic challenge to the treating physician. In this study, we present our experience with the administration of a large-volume blood patch to multiple sites in the epidural space through a single-catheter access site.
MATERIALS AND METHODS: A retrospective review was conducted of patients with spontaneous intracranial hypotension who underwent a large-volume blood patch to multiple sites in the epidural space through a single-catheter access site from 2010 to 2012. Patient demographic data, clinical charts, indications for treatment, radiographic images, procedure notes, and postprocedure hospital course were reviewed.
RESULTS: Overall, 9 patients were identified who underwent 20 blood patch procedures. Patients were selected to undergo the large-volume procedure either because they had a failed site-directed epidural blood patch or if imaging demonstrated multiple possible leak sites. There were 6 women and 3 men, with an average age of 33.5 years. The mean volume of blood injected per procedure was 54.1 mL (median = 55 mL; range = 38–70 mL). All patients had an orthostatic headache as one of their presenting symptoms; 22% also presented with neurocognitive decline and behavioral changes; 89% of patients had improvement or resolution of their symptoms; and 80% of patients who had a previously failed site-directed epidural blood or fibrin glue patch improved with a large volume catheter-directed blood patch.
CONCLUSIONS: Our experience supports the use of a large-volume blood patch to multiple sites in the epidural space through a single-catheter access site for the treatment of spontaneous intracranial hypotension. Additionally, our results indicate a role for this procedure in refractory cases of spontaneous intracranial hypotension.
ABBREVIATION:
- SIH
- spontaneous intracranial hypotension
Spontaneous intracranial hypotension (SIH) is a well-recognized entity associated with a CSF leak. The characteristic clinical presentation is a positional headache, which is often severe. CSF leak can occur spontaneously or can be the result of trauma or an iatrogenic cause. Epidural blood patch has long been considered the procedure of choice for treatment of a CSF leak. In cases of SIH or idiopathic intracranial hypotension, the CSF leak site may not be identified or multiple areas of leak may be present. Additionally in iatrogenic cases, the leakage may be refractory to small-volume single-site injection of epidural blood. Treatment in these cases presents a unique challenge. Administration of a large-volume blood patch at multiple sites in the epidural space is a recently reported novel technique for the treatment of SIH.1 Direct injection of blood to multiple sites allows directed therapy at suspected leak sites and treatment of occult sites. Additionally, this treatment avoids puncture of the epidural space in the thoracic and cervical spine, making it theoretically less challenging for the operator. We present our experience with the use of a large-volume blood patch to multiple sites in the epidural space through a single-catheter access site for the treatment of SIH.
Materials and Methods
This study was approved by the institutional review board at the University of Michigan. We retrospectively reviewed cases of spontaneous or refractory intracranial hypotension that were treated with a large-volume epidural blood patch to multiple sites in the epidural space through a single-catheter access site at our institution from 2010 to 2012 for the treatment of SIH. Pertinent medical records including operative notes, laboratory values, and clinical notes were reviewed and correlated with imaging (Table 1). Radiologic imaging, including CT, MR imaging, myelography, CT myelography, and MRI myelography, was reviewed. Preprocedural imaging was reviewed by attending neuroradiologists and by the procedural operators to assess possible sites of leakage before the procedure. Patient outcomes were graded on the basis of symptom response to therapy and symptom recurrence. Our grading system is further defined in Table 2.
Case characteristics
Multisite epidural blood patch procedures and outcomesa
Procedure
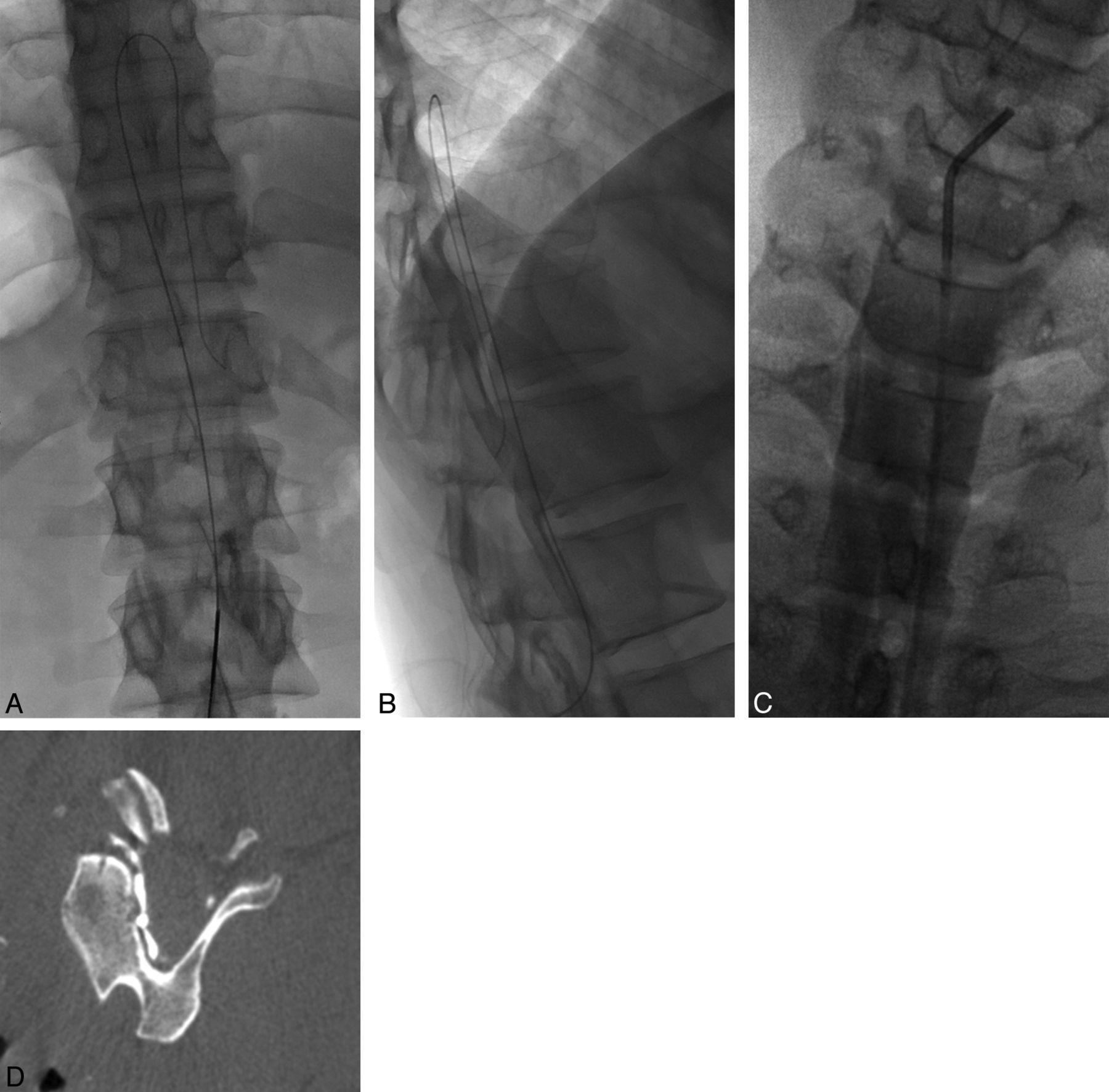
Patients were brought to the angiography suite and placed prone. The access site was prepped and draped in a sterile fashion. Local anesthesia was achieved by using a 2% lidocaine injection. Under fluoroscopic guidance, a 19-ga Tuohy needle was advanced into the epidural space at a spinal level (L3 was most commonly used) (Fig 1). Contrast was injected into the epidural space to confirm the position. An angled 0.035 Glidewire (Terumo, Tokyo, Japan) was advanced through the 19-gauge needle into the epidural space and extended superiorly into the midthoracic region and looped in the epidural space (Fig 2A, -B). The needle was removed. A 4F sheath (Terumo) was then placed over the wire into the epidural space, and a 4F vertebral catheter (Cordis Sheath Terumo, Miami Lakes, Florida) was advanced over the Glidewire (Terumo). The wire and catheter were advanced superiorly to the desired level within the midcervical spine (Fig 2C). The goal was to advance the catheter in the dorsal epidural space. The wire was removed, and contrast was injected through the catheter to confirm the position in the epidural space. DynaCT (Siemens, Erlangen, Germany) was performed to confirm the catheter position when the catheter was not definitely determined to be in the epidural space (Fig 2D), given that we were injecting a large volume of blood. At this time, an aliquot of autologous blood was obtained from a previously placed intravenous access site. DuraSeal (Covidien, Irvine, California) was mixed with autologous blood in cases that had recurrent symptoms following a prior large-volume blood patch procedure. The autologous blood was injected into the epidural space while we slowly withdrew the catheter to the access site (approximately 1–2.5 mL per vertebral body level). The 4F catheter and the sheath were removed, and hemostasis was achieved with manual pressure.

Spot fluoroscopic image shows a 19-ga Tuohy needle at the L3 vertebral body with contrast opacifying the epidural space.
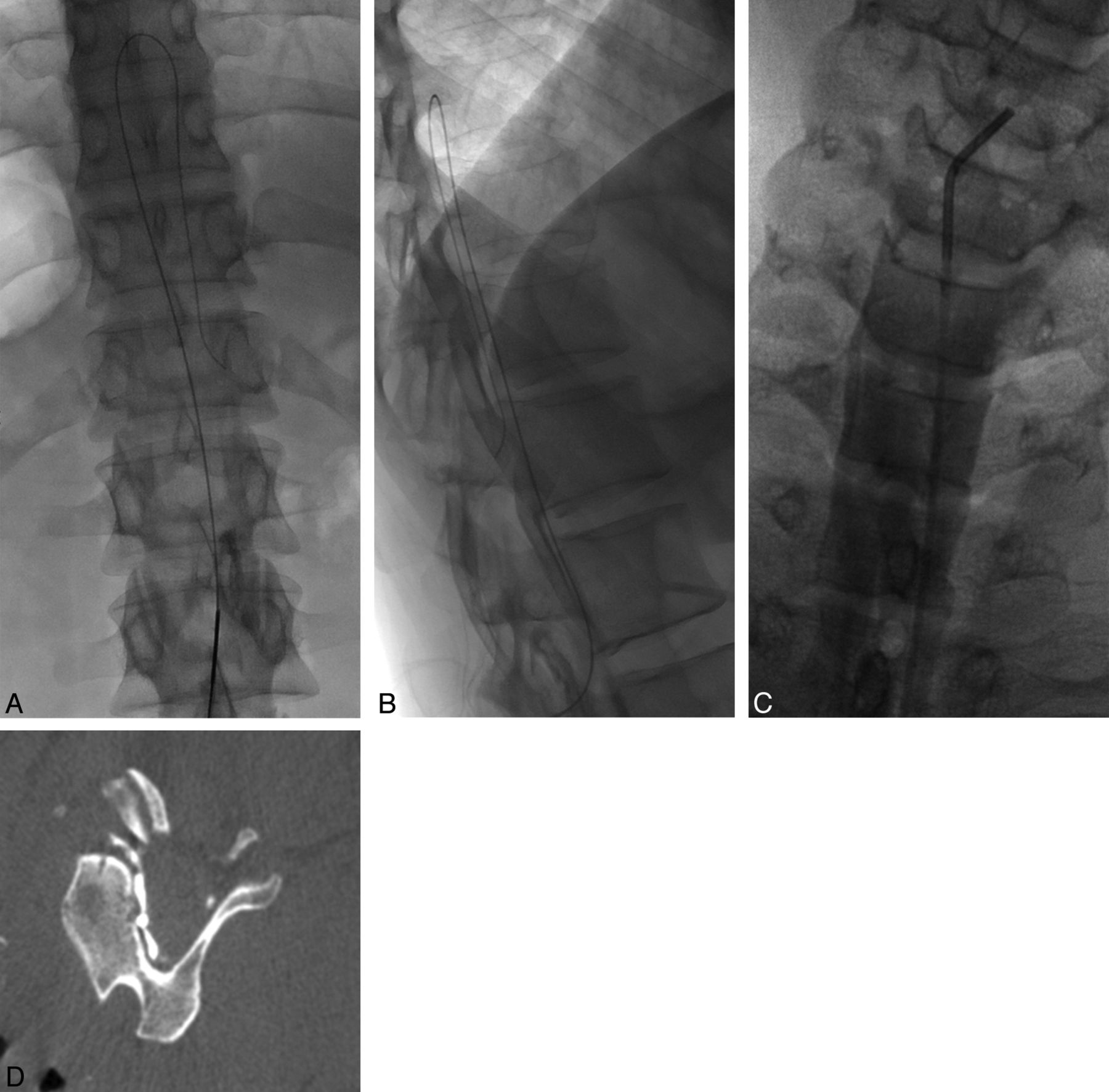
A and B, Frontal and lateral spot fluoroscopic images show a needle in the epidural space at L2 and a Glidewire curled in the epidural space in the lower thoracic spine. C, Frontal spot fluoroscopic image shows a 4F vertebral catheter that has been advanced over the wire in the epidural space from the L2 vertebral body to C4, with contrast opacifying the epidural space. D, Axial DynaCT shows the catheter and contrast opacifying the cervical epidural space.
An additional access site in the epidural space of the lower lumbar spine by using a 19-gauge spinal needle was obtained if either epidural scarring from a prior patch procedure prevented catheter advancement or if a blood patch was needed to target the lower lumbar and/or sacral regions. In these cases, a single-catheter access site was still obtained above the level of scarring to allow large-volume administration cranial to the scarring site.
Results
Nine patients were identified. Twenty large-volume blood patches to multiple sites in the epidural space through a single-catheter access site were performed for the treatment of SIH. The average patient age at the time of the first procedure was 33.5 years. There were 6 women and 3 men. All patients had an orthostatic headache as one of their presenting symptoms. Twenty-two percent (2/9) of patients presented with neurocognitive decline; 56% (5/9) had undergone prior blood patch procedures with a single-site-directed injection; and all of these had either progressed back to baseline or had not improved at all. These patients were referred for our procedure because of their persistent symptoms and their desire for further management. Forty-four percent (4/9) of patients had not undergone prior traditional therapeutic measures and were referred because of an ambiguous leak site or suspicion of multiple leak sites; 78% (7/9) of patients did not have an identifiable event that caused their intracranial hypotension and symptoms. Preprocedural data for all patients are presented in Table 1.
The average number of large-volume multisite blood patch procedures per patient was 2.2 (range = 1–5). Average follow-up time after the final procedure was 2.3 months (median = 2 months; range = 0.25–7 months). The mean amount of total autologous blood injected per procedure was 54.1 mL (median = 55 mL; range = 38–70 mL). DuraSeal was used in 35% of cases (8/20). There were no significant procedural complications. Eighty-nine percent (8/9) of patients had improvement of their symptoms. One patient improved transiently but then worsened back to her baseline headache. No patients had worsening of their symptoms after the immediate postprocedural period. Eighty percent (4/5) of patients who initially did not respond to a conventional blood patch procedure improved with the multisite epidural blood patch technique. One hundred percent of patients who had failed conventional therapy required >1 multisite epidural blood patch procedure (5/5). Patient 7 had improved mental status after 2 procedures but had persistent encephalopathy and elected to undergo experimental therapy at another institution. Procedural and outcome data for all patients are presented in Table 2.
Illustrative Case
A 22-year-old woman (patient 8 from Tables 1 and 2) with a long-standing history of migraines presented with new onset of disabling orthostatic headaches for 1 month. These headaches were described as a pressure sensation of severe intensity (10/10) and located over the entire cranium. The patient also noted nausea and neck stiffness. She denied any trauma or chiropractic manipulation. She was started on caffeine and theophylline, which did not alleviate her headaches. She was later prescribed ketorolac (Toradol) and corticosteroids, which still did not provide headache relief.
Findings of initial CT of the head were unremarkable. MR imaging of the head showed findings consistent with intracranial hypotension (Fig 3A, -B). MR imaging myelography showed multiple areas of possible CSF leak throughout the thoracic spine. The patient underwent a blood patch procedure with 20 mL of autologous blood injected into the epidural space at L4. A 4F vertebral catheter was advanced over a Glidewire from T12 to C5, and 25 mL of autologous blood was injected through the catheter via a pullback technique from C5–T12. The patient's headaches decreased to 2/10 postprocedure but began to worsen again after 2 weeks. The patient underwent a second blood patch procedure with injection of 20 mL of autologous blood at L3 (Fig 1), a 4F vertebral catheter advanced over a Glidewire from L2 to C3, and 28 mL of autologous blood injected through the catheter by using a pullback method from C3–L2 (Fig 2A–D). In both procedures, a separate lumbar access site was used to allow increased blood patch coverage in the more caudal epidural space.
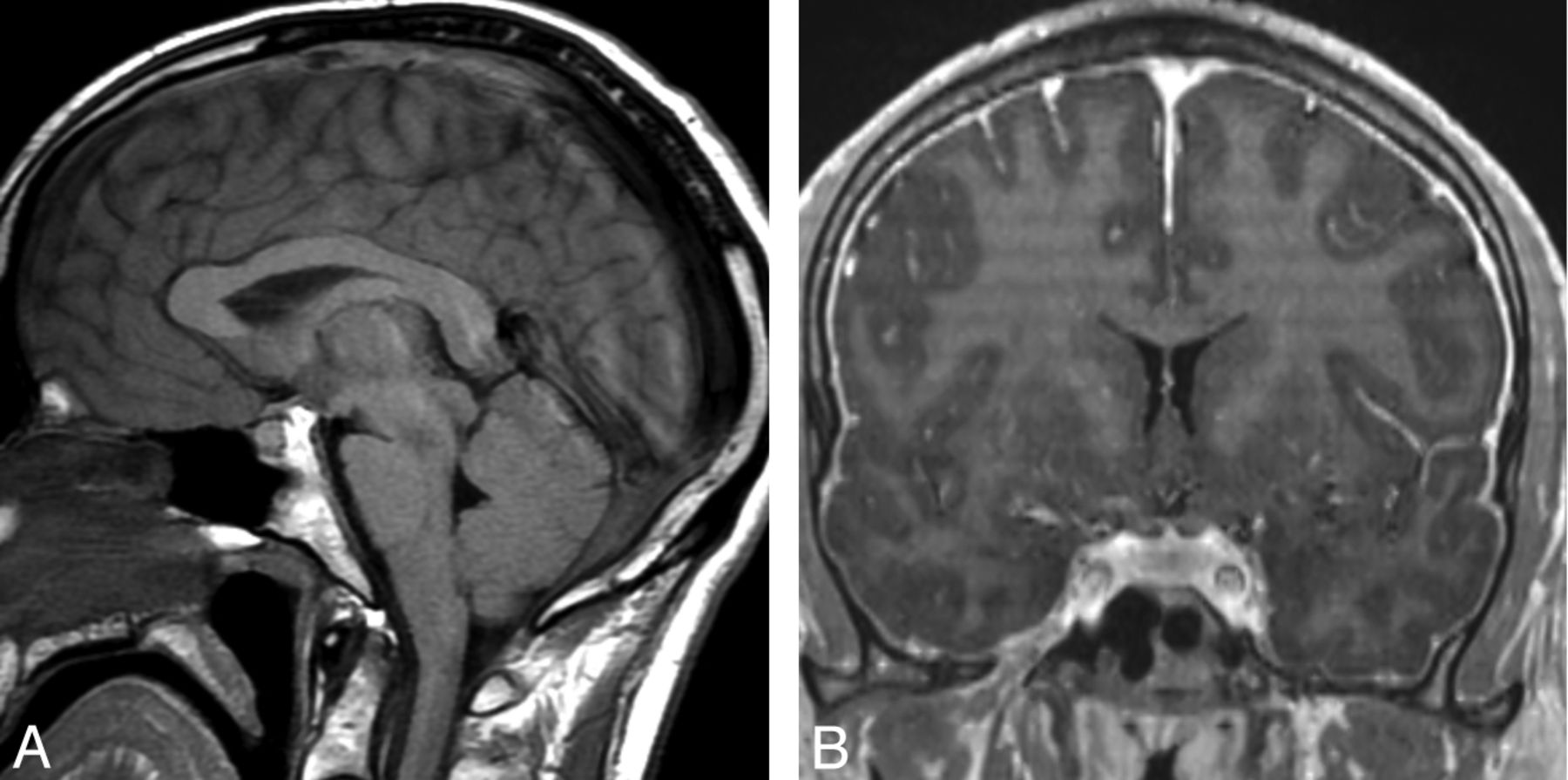
A, Sagittal T1-weighted MR image shows descent (“sagging” or “sinking”) of brain, enlargement of the pituitary gland, and obliteration of the cisterns. B, Coronal postcontrast T1-weighted MR image of the same patient shows diffuse pachymeningeal enhancement.
Her headaches completely resolved postprocedure and have not recurred at 3-month follow-up. MR imaging of the brain showed complete resolution of the diffuse pachymeningeal enhancement, descent (“sagging” or “sinking”) of the brain, enlargement of the pituitary gland, and engorgement of the cerebral venous sinuses (Fig 4A, -B).

A, Sagittal T1-weighted MR image 6 weeks after treatment shows an image of the brain with normal findings. B, Coronal postcontrast T1-weighted MR image after treatment shows resolution of the diffuse pachymeningeal enhancement.
Discussion
In this study, we evaluated our experience with administration of a large-volume blood patch to multiple sites in the epidural space by using a single-catheter access site for the treatment of spontaneous intracranial hypotension. SIH is a multifactorial process associated with CSF leak. The hallmark symptom of SIH is an orthostatic headache, which was present in all of our patients.2 Additional possible symptoms include nausea, vomiting, dizziness, tinnitus, neck pain, or radiculopathies.2,3 Two patients in our series presented with neurocognitive decline and behavioral changes. This presentation is rarer but has also been reported.4,5
Clinical suspicion for SIH can be confirmed by demonstrating low opening pressure on lumbar puncture or with imaging.6 Brain MR imaging findings include diffuse pachymeningeal enhancement, descent (“sagging” or “sinking”) of the brain, subdural fluid collections, enlargement of the pituitary gland, engorged cerebral venous sinuses, and a decrease in size of the ventricles.6⇓–8 Spinal imaging with CT or MR imaging can show extra-arachnoid fluid collections, extradural extravasation of fluid, meningeal diverticula, spinal dural enhancement, and engorgement of the spinal epidural venous plexus.6⇓–8 In some cases, however, no definite leak site or other abnormality is identified.
Cases in which a definite leak site is not identified or those in which multiple sites are found present a therapeutic challenge. Most interesting, it is believed that spontaneous CSF leaks occur most often at the cervicothoracic junction or in the thoracic spine.9 Prior authors have reported symptomatic improvement rates ranging from 50% to 100% with site-directed epidural blood/fibrin patch procedures by using CT or fluoroscopic guidance.10⇓⇓⇓⇓–15 These treatment options, however, often require epidural punctures in the upper thoracic and cervical spine. Epidural puncture in these regions is technically more challenging due the anatomy and the epidural space becoming smaller as you ascend from the lumbar to the cervical region. Also, in cases with multiple leak sites, multiple punctures in the thoracic and cervical spine may be required. To address this shortcoming, Ohtonari et al1 recently reported their experience with multiple-site epidural blood patch through a single-catheter access site in 5 patients. All their patients improved, with an average injection of 45 mL of autologous blood at multiple levels in the epidural space.
In our series, we injected an average of 54 mL of autologous blood at multiple sites in the epidural space and had an outcome similar to that of Ohtonari et al.1 Eighty-nine percent of patients in our series had improvement or resolution of their symptoms. Furthermore, 80% (4/5) of patients in our series who had previously failed therapy with a site-directed blood and/or fibrin glue patch improved with our large-blood-volume catheter-based procedure, without recurrence to their baseline symptoms. This outcome suggests a role for this procedure in challenging or refractory cases of SIH. In 35% of our cases, we used DuraSeal in addition to the blood patch for possible added sealant properties. DuraSeal was used at the discretion of the operator, mostly in those cases that had recurred or had severe residual symptoms after large-volume blood patch. Additionally, it was used in those deemed to have an extensive CSF leak. In patients improving with large-volume blood patch and less severe residual symptoms, DuraSeal was considered unnecessary.
Because our procedure is relatively novel, the risk profile is unknown. We did not experience any significant complications in our patient population. Hypothetic complications include persistent epidural hematoma and epidural abscess with or without neurologic sequela. The authors suspect that the occurrence of these complications would be low, as evidenced in patients instrumented with epidural pain catheters. In these cases, epidural hematoma is rare, being reported in approximately 1:150,000.16 Clinically symptomatic hematoma rates are expected to be even lower.16 Similarly, epidural abscesses are rare with epidural pain catheters, reported in 1:1930 cases.17 Additionally, epidural abscesses are noted only in patients in whom the catheter remains for >3 days.17 To further decrease the rates of these complications, we recommend proper sterile technique, minimizing procedural length, and avoidance of anticoagulants in the periprocedural period. Also, looping the wire and catheter in the epidural space (as displayed in the figures) before advancing them cranially should limit epidural vessel injury by avoiding a relatively sharp leading edge. Similarly, by only placing the catheter in the dorsal epidural space, more lateral nerve root sleeves and ventral vascular structures such as the artery of Adamkiewicz and the epidural venous plexus can be avoided. An additional risk consideration is damage to suspensory ligaments of the dural sac. These play a role in supporting the spinal cord in the canal. Damage to the dorsal suspensory ligaments could cause dural leaks and has been shown to cause flexion myelopathy in animal models.18 Care should be taken to gently advance the catheter and wire and to cautiously redirect them if there is any evidence of difficulty advancing the wire or catheter in the epidural space.
Our results suggest that multisite epidural blood patch through a single catheter access site is a safe alternative to traditional site-directed epidural blood patch in patients with multiple suspected CSF leak sites or in those in whom no definite leak site is identified. In addition, our procedure may improve outcomes in patients who are refractory to traditional techniques. Our procedure provides the treating physician with an additional technique for this challenging pathology and may be technically less challenging with practice than is site-directed epidural blood patch in the thoracic and cervical spine.
Our experience is limited by the small cohort size and retrospective nature. In addition, our average follow-up was relatively short at 2.3 months. Future studies should include larger patient cohorts and longer follow-up periods.
Conclusions
Our experience supports the use of a large-volume blood patch to multiple sites in the epidural space through a single-catheter access site for the treatment of SIH, where no definite or multiple CSF leak sites are identified. Additionally, our results indicate a role for this procedure in SIH, which is refractory to traditional directed epidural patch procedures. Future studies should evaluate outcomes in larger patient populations with a particular focus on outcomes in patients who have failed prior lumbar epidural puncture procedures or leak-site-directed procedures.
Footnotes
Disclosures: Aditya S. Pandey—UNRELATED: Grants/Grants Pending: Covidien,* MicroVention,* Comments: industry grant support for research unrelated to the current manuscript. *Money paid to the institution.
REFERENCES
- Received January 2, 2014.
- Accepted after revision February 18, 2014.
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}