
Abstract
BACKGROUND AND PURPOSE: Age-dependent structural changes of the globes occur during gestation. The posterolateral globe margins bulge outward, and the eyes are conical in early gestation. Later, the globes are ellipsoid. The purpose of this study was to establish normal developmental fetal globe morphology.
MATERIALS AND METHODS: The fetal MR imaging data base at an academic children's hospital was queried for all brain MRIs performed during 8 years. Motion artifacts, brain/craniofacial/globe malformations, and chromosomal defects were exclusion criteria. Two board-certified neuroradiologists evaluated each examination for globe shape (elliptic/nonelliptic) and hyaloid visibility. Logistic regression was used to evaluate correlations among variables. Age-specific cut-points for globe shape and hyaloid visibility were chosen to optimize specificity.
RESULTS: We identified 1243 examinations from 1177 patients. Six hundred eighty-two examinations met the inclusion criteria (17–39 weeks). Receiver operating characteristic analysis showed that age was highly predictive of globe shape (area under the curve = 0.99) and fetal vasculature visibility (area under the curve = 0.94). Nonelliptic globes were universal up to 22 weeks. Thereafter, globes gradually assumed an elliptic shape, present in nearly all patients 29 weeks and older (sensitivity, 81%; 95% CI, 76%–85%; specificity, 99%; 95% CI, 98%–100%). The hyaloid vasculature was visible in most patients up to 19 weeks and occasionally in those at 20–24 weeks, but never in those 25 weeks and older (sensitivity, 69%; 95% CI, 65%–72%; specificity, 100%; 95% CI, 95%–100%).
CONCLUSIONS: Physiologic nonspheric globe shapes are normal up to 29 weeks' gestation and should not be misinterpreted as pathologic. Thereafter, globes are generally elliptic. The timing of this process coincides with the resolution of the primary vitreous and may be related.
The eyes are complex organs of sight. Primordial ocular tissue originates at the end of the first gestational month, just before neural tube closure, as paired projections from the basal forebrain. Ectoderm, mesoderm, and neural crest cells all contribute to the formation of the mature globe and related orbital components.1 During gestation, the globes undergo progressive enlargement, corresponding best to a quadratic curve.2⇓–4 The composition of the largest segment of the eye, the vitreous chamber, changes during gestation as well. The primary vitreous transmits primitive vasculature called the “hyaloid artery,” which supports the developing vitreous and lens. Then, the primary vitreous is replaced with secondary (mature) vitreous in normal situations. Meanwhile, the hyaloid vasculature regresses contemporaneously for weeks, sometime during the second and third trimesters.5⇓⇓⇓–9
As the ocular globes grow and develop, their shapes evolve from asymmetric elongated/conical toward a nearly spheric, elliptical morphology. Ellipsoid globe shape is not typically achieved until late in gestation. On fetal MR imaging, the developing globes display a focal convexity along their posterolateral margins in the axial plane and a conical, keel shape in the sagittal plane. Knowledge of age-specific fetal globe anatomy is necessary to distinguish normal development from structural pathology as can be seen in diseases such as microphthalmia, coloboma, and persistent fetal vasculature, all of which may be occasionally associated with various syndromes and chromosomal defects.2,10 The purpose of this study was to establish the normal morphologic appearance of the developing globes at different gestational ages.
Materials and Methods
This Health Insurance Portability and Accountability Act–compliant retrospective study was performed after institutional review board approval. The fetal MR imaging data base at a single academic children's hospital was queried for all fetal brain MR imaging examinations performed during an 8-year period (February 2007 to February 2015). Examinations with excessive motion artifacts, structural brain and craniofacial malformations, brain growth retardation, and overt globe malformations were excluded. Gestational age at the time of imaging was extracted from each patient's medical record. Gestational age was established by the clinicians caring for the patient on the basis of the last menstrual period and sonographic data.
Studies were performed on a 1.5T MR imaging scanner (GE Healthcare, Milwaukee, Wisconsin; or Siemens, Erlangen, Germany). Sequences included multiplanar single-shot fast spin-echo T2-weighted images (flip angle, 90°; TR/TE, 910–1090/60–160 ms; 2- to 5-mm section spacing with no gap; NEX, 0.53; echo-train length, 1); multiplanar heavily T2WI (“hydrography” or “fetography”) (flip angle, 90°; TR/TE, 5000/163 ms; 2- to 5-mm section spacing with no gap; NEX, 0.54; echo-train length, 1) (GE Healthcare); or multiplanar half-Fourier acquisition single-shot turbo spin-echo images (flip angle, 150°; TR/TE, 1270/80 ms; 3- to 5-mm section spacing with no gap; NEX, 1; echo-train length, 250) (Siemens).
A qualitative structural analysis of bilateral fetal globes was undertaken by 2 fellowship-trained neuroradiologists with American Board of Radiology subspecialty certificates in neuroradiology. Gestational ages were not provided to the reviewers before interpretation. Both readers had >4 years of clinical experience after subspecialty board certification. Although the entire imaging dataset included visibility of the brain and globes, reviewers were careful to focus on the appearance of the globes and ignored the brain to the extent possible. Each reader reviewed 200 cases independently with excellent interreader reliability (Cohen κ coefficient = 0.98). The few initial discrepancies between readers were resolved in consensus. A consensus reading was also reached in all other cases.
Ocular globes were assessed in axial, sagittal, and coronal planes. Ocular globe shape was recorded either as “elliptic,” “nonelliptic,” or “transitional.” All intermediate, ambiguous, and mild cases of nonellipsoid globe morphology in ≥1 imaging plane were considered “transitional.” For statistical simplicity, transitional and definitively nonelliptic cases were grouped together and considered “nonelliptic.” Hyaloid vasculature was noted to be either present or absent on the basis of whether tubular/linear hypointense signal was seen extending from the posterior globe margin to the lens.
Data Collection and Statistics
Data were stored and analyzed by using an Excel 2011 spreadsheet (Microsoft, Redmond, Washington). Logistic regression analyses were used to evaluate the relationship between age and globe shape as well as age and visibility of hyaloid vasculature. Receiver operating curve characteristics were subsequently calculated. Sensitivity and specificity at each gestational week data-point were calculated to determine the optimal cut-points for visibility of fetal vasculature and ellipsoid globe morphology. Cut-points were chosen to optimize specificity at the expense of sensitivity. P values < .05 were considered significant.
Results
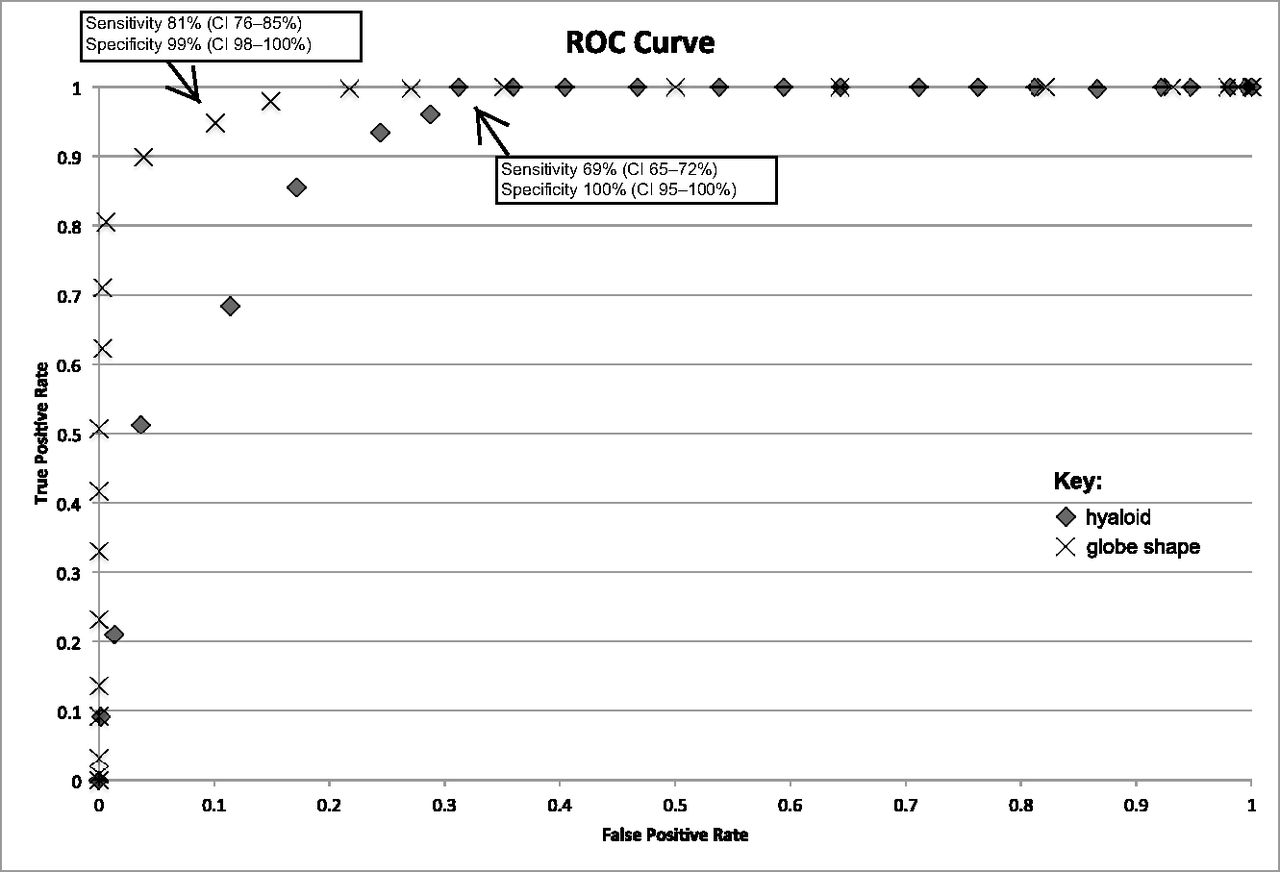
We reviewed 1243 examinations from 1177 patients; 561 examinations were excluded. Six hundred eighty-two examinations from patients of 17–39 weeks' gestational age met the inclusion criteria (mean, 27 ± 0.4 weeks' gestation). Receiver operating characteristic analysis showed that age was highly predictive of globe shape (area under the curve = 0.99) and visibility of the fetal vasculature (area under the curve = 0.94) (Fig 1). Gestational age cut-points were determined to be 29 weeks (sensitivity, 81%; 95% CI, 76%–85%; specificity, 99%; 95% CI, 98%–100%) and 25 weeks (sensitivity, 69%; 95% CI, 65%–72%; specificity, 100%; 95% CI, 95%–100%) for the presence of elliptic globes and the absence of fetal vasculature, respectively (Fig 1). Globe morphology and internal signal corresponding to the presence or absence of hyaloid vasculature changed during gestation (Table and Fig 2).
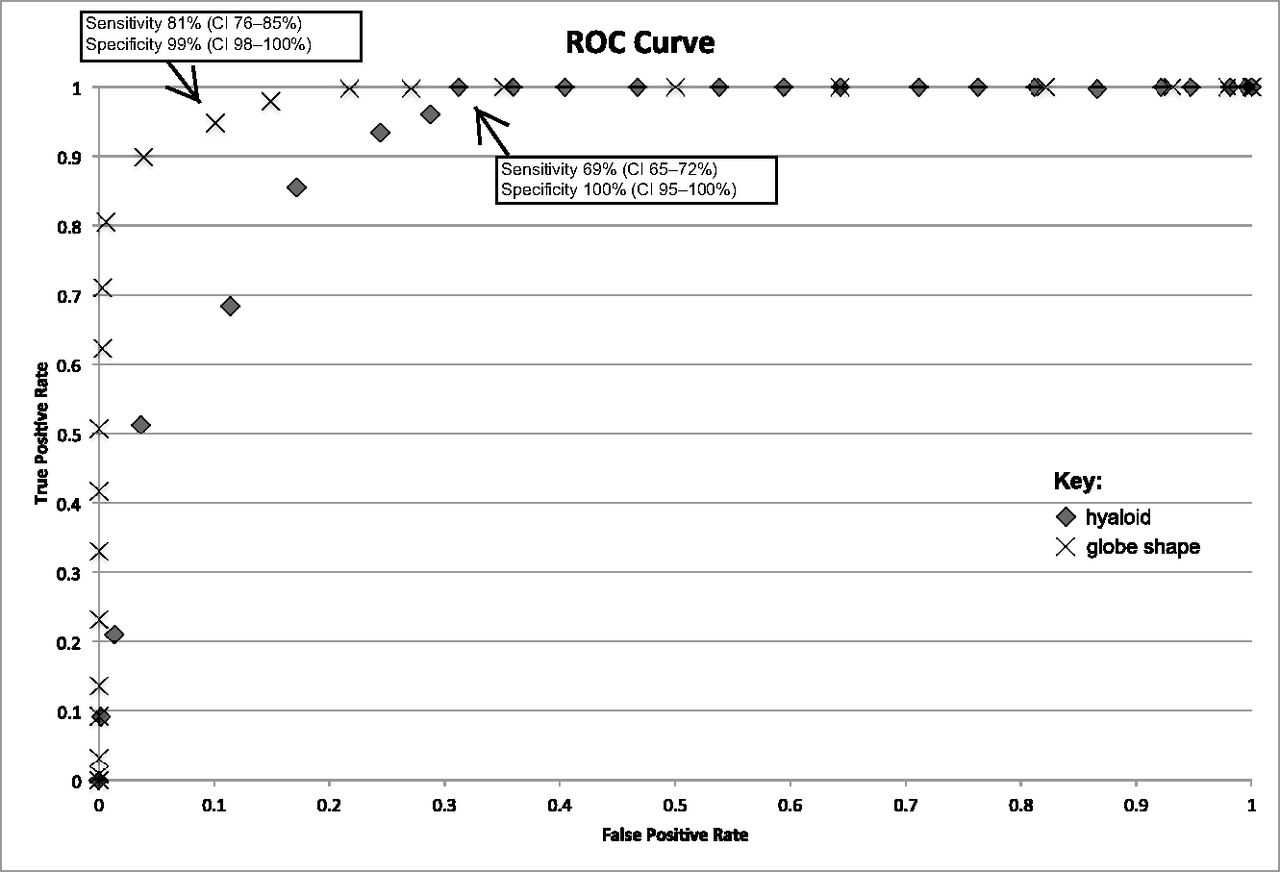
Receiver operating characteristic curves demonstrate sensitivity (true-positive) versus 1-specificity (false-positive) of MR imaging of the fetal brain for elliptic globe shape (X) and hyaloid vasculature visibility (diamond) as a function of age.
Frequency of hyaloid visibility and elliptic, transitional, nonelliptic, and combined transitional and noneliptic globe morphology at various gestational ages (16–39 weeks)

Age-related changes in globe morphology and hyaloid vasculature visibility from 17 to 39 weeks' gestation.
All globes were generally symmetric to one another in shape bilaterally. Nonelliptic globe morphology (focal convexity of the posterolateral margins) was universal until 22 weeks' gestation in both the axial and sagittal planes (Figs 3 and 4A, -B). Thereafter, globe morphology gradually changed. At 22–24 weeks, most patients had nonelliptic globes (sagittal and axial planes), and a few were transitional, approaching an elliptic shape (abnormal only on axial images). At 25–28 weeks, noticeably milder changes occurred, with minor nonelliptic globe morphology generally only visible in the axial plane in most patients. At 29 weeks and beyond, almost all patients demonstrated elliptic globe morphology with no more than minimal contour deformity noted (Fig 4 and Table). All patients with follow-up fetal MR imaging examinations (n = 25) had progression of globe morphology toward an elliptic shape in accordance with this timeline.

Sagittal (A) and axial (B) “fetography” T2WI (TR/TE, 5000/163 ms) of a normal fetal brain at 20 weeks' gestational age. The globe morphology is conical, with angulation of its posterior (arrows, A) and posterolateral (arrows, B) margins.

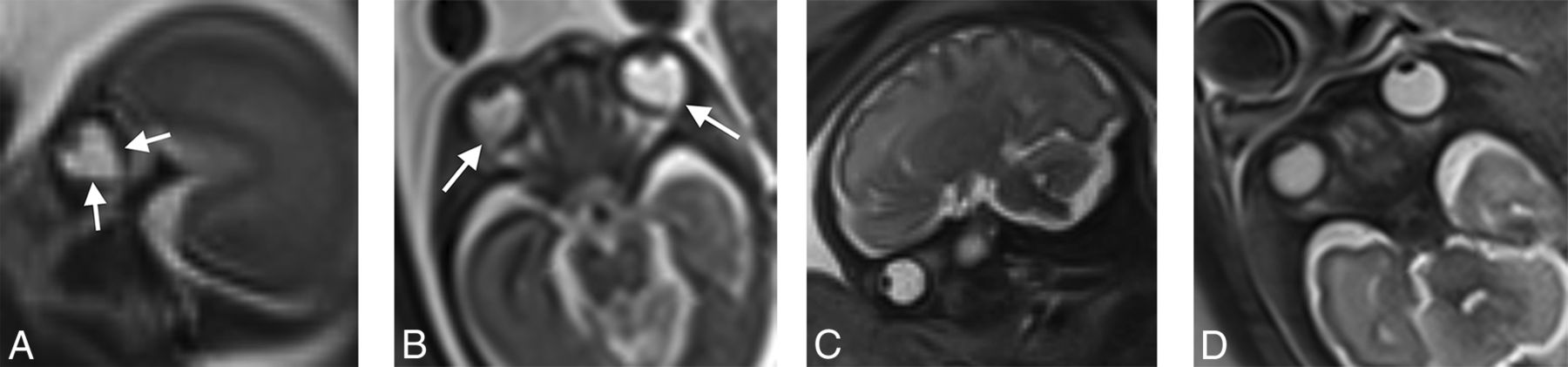
Sagittal (A) and axial (B) T2 HASTE (TR/TE, 1270/80 ms) of a normal fetal brain at 18 weeks' gestational age. The globe morphology is conical with angulation of its posterior (arrows, A) and posterolateral (arrows, B) margins. Follow-up sagittal (C) and axial (D) T2 HASTE (TR/TE, 1270/81 ms) of a normal fetal brain from imaging performed on the same patient at 30 weeks' gestational age. Ocular globe morphology is round/elliptic in the axial and sagittal planes. Fetal vasculature is not visible.
The hyaloid vasculature was visible in most patients up to 19 weeks, then occasionally up to 24 weeks (Fig 5). After that, the hyaloid vasculature system was no longer detectable.

Sagittal single-shot fast spin-echo T2WI (TR/TE, 1087/56 ms) of a normal fetal brain at 19 weeks' gestation. Linear hypointense signal extending from the posterior margin of the lens through the vitreous toward the apex represents the hyaloid vasculature (arrow).
Discussion
The embryologic origin of the ocular globe and its components is varied and complex. Multiple cell types contribute to ocular formation, including neuroectoderm, surface ectoderm, mesoderm, and neural crest cells. Thus, globe malformations can be seen in conjunction with craniofacial and brain malformations and as part of a number of syndromes. On imaging, eye abnormalities may take the form of alterations in size and/or shape of the ocular globes, either symmetric or asymmetric, underscoring the importance of in utero globe structure assessment. Size and shape asymmetries can be found in both acquired diseases (eg, infectious, inflammatory, or ischemic injury) and congenital processes (eg, microphthalmia, colobomas, persistent fetal vasculature, chromosomal abnormalities, and dystroglycanopathies).2,10 Furthermore, abnormalities of globe structure may impart valuable information regarding the integrity of the brain and surrounding craniofacial structures.
The primary vitreous appears in the first gestational month, begins to regress at the end of the first trimester, and is nearly completely replaced by the secondary vitreous by 30 weeks.1,6,9⇓–11 The hyaloid vasculature is a marker for the primary vitreous; it involutes in conjunction with the primary vitreous but may persist until the 34th gestational week.12 The hyaloid artery and canal are small structures that challenge the resolution of imaging. On sonography, the hyaloid artery is normally seen up to the beginning of the third trimester and can be seen up to 28–30 gestational weeks.6,8,9 Sonographic visibility of the hyaloid vascular system after 30 weeks is abnormal and indicates residual primary vitreous or persistent fetal vasculature. Persistent fetal vasculature is generally unilateral. Bilateral persistent fetal vasculature should raise a differential diagnosis of Walker-Warburg syndrome, Norrie disease, and chromosomal trisomies.6,10,13
Sparse literature exists regarding the regression of the hyaloid system on fetal MR imaging; however, hyaloid vasculature is not generally visible after 20 weeks.10 Our findings are in general agreement in that most examinations performed after 20 weeks had homogeneous vitreous signal; however, we did identify anteroposteriorly oriented linear hypointense signal traversing the vitreous in several patients of 17–24 weeks' gestational age, more commonly in younger patients, consistent with components of the hyaloid vascular system. The hyaloid vasculature is not normally visible in patients 25 weeks or older on MR imaging, assuming an identical imaging technique. Hyaloid visibility beyond this time should raise suspicion of persistent fetal vasculature.
Mature fetal globe shapes are generally described as round or spheric. However, Li et al3 reported that the normal fetal globe shape is better classified as elliptic because globes are consistently larger in the transverse than the anteroposterior dimension throughout gestation. Our study demonstrates that elliptic ocular globe morphology is not fully achieved until the third trimester. Convexity of the posterolateral globe margins in the axial plane and conical, keel-shaped globes in the sagittal plane are transient and normal in the early developing eyes. This morphology may persist until around 29 weeks. Thereafter, the globes assume a nearly round or elliptic shape. Nonelliptic globes in patients older than 29 weeks' gestational age should raise suspicion of possible structural pathology. Most important, our study also shows that ocular globe morphology is symmetric on fetal MR imaging in the second and third trimesters (17–39 weeks) under normal circumstances. All apparent asymmetries between the ocular globes should be closely inspected; definitive asymmetries should be considered pathologic unless proved otherwise.
Limitations of this study include its retrospective design and the inability to ensure that each patient's ocular globes were entirely normal. However, globe morphology differences were consistent among patients during gestation. Motion artifacts could have caused apparent shape alterations and ghosting artifacts that simulated the hyaloid vascular system. Some degree of patient motion artifacts was an inevitable limitation; however, examinations with excessive motion artifacts were excluded. Although gestational ages were not provided to the readers during assessment and the brain was ignored to the extent possible when assessing the globes, images of the brain were visible to the reader in each study, potentially introducing an interpretation bias. However, between 23 and 28 weeks of gestation, when globe shapes transition from nonelliptic to elliptic, the extent of brain sulcation and gyration changes only modestly, whereas anterior frontal lobe sulcation near the orbits does not. Therefore, it was relatively easy for the readers to remain uninformed as to the gestational age during these critical weeks.
Conclusions
Physiologic nonelliptic globe shapes are normal up to 29 weeks' gestation and should not be misinterpreted as pathologic. Thereafter, the ocular globes assume an elliptic morphology. Transient symmetric, nonelliptic globes with convexity of the posterolateral margins are a normal developmental phenomenon. The timing of this process coincides with the resolution of the primary vitreous and hyaloid vasculature and may be related. Any major morphologic asymmetry between the ocular globes should be considered pathologic.
References
- Received November 3, 2015.
- Accepted after revision February 8, 2016.
- © 2016 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}