
Abstract
BACKGROUND AND PURPOSE: Multiple sclerosis is an autoimmune disorder resulting in progressive neurologic disability. Our aim was to evaluate the associations between diffusional kurtosis imaging–derived metrics for the corticospinal tract and disability in multiple sclerosis.
MATERIALS AND METHODS: Forty patients with MS underwent brain MR imaging including diffusional kurtosis imaging. After we masked out T2 hyperintense lesions, the fractional anisotropy, mean diffusivity, radial diffusivity, axial diffusivity, mean kurtosis, radial kurtosis, and axial kurtosis were estimated for the corticospinal tract. Disability was quantified by using the Expanded Disability Status Scale at the time of MR imaging and 12 months post-MR imaging. The Pearson correlation coefficient and linear regression analyses were conducted to evaluate the associations between diffusion metrics and disability.
RESULTS: Significant correlations were found between the Expanded Disability Status Scale scores during the baseline visit and age (r = 0.47), T2 lesion volume (r = 0.38), corticospinal tract mean diffusivity (r = 0.41), radial diffusivity (r = 0.41), axial diffusivity (r = 0.34), fractional anisotropy (r = −0.36), and radial kurtosis (r = −0.42). Significant correlations were also found between the Expanded Disability Status Scale scores at 12-month follow-up and age (r = 0.38), mean diffusivity (r = 0.45), radial diffusivity (r = 0.41), axial diffusivity (r = 0.45), mean kurtosis (r = −0.42), radial kurtosis (r = −0.56), and axial kurtosis (r = −0.36). Linear regression analyses demonstrated significant associations among radial kurtosis, age, and Expanded Disability Status Scale score during the baseline visit, while radial kurtosis was the only variable associated with Expanded Disability Status Scale score for the 12-month follow-up.
CONCLUSIONS: Radial kurtosis of the corticospinal tract may have an association with neurologic disability in MS.
ABBREVIATIONS:
- CST
- corticospinal tract
- DKI
- diffusional kurtosis imaging
- EDSS
- Expanded Disability Status Scale
- EDSS12 m
- EDSS score at 12-month follow-up
- EDSS0
- EDSS at baseline visit
- FA
- fractional anisotropy
- K‖
- axial kurtosis
- K⊥
- radial kurtosis
- λ‖
- axial diffusivity
- λ⊥
- radial diffusivity
- MD
- mean diffusivity
- MK
- mean kurtosis
- NAWM
- normal-appearing white matter
- VIF
- variance inflation factor
Multiple sclerosis is an autoimmune disorder of the central nervous system characterized by recurrent episodes of inflammation, demyelination, edema, and axonal loss, which can result in a progressive accumulation of neurologic disability.1 MR imaging is routinely performed to assess the burden of disease in patients with MS to guide therapeutic decisions.2 Conventional MR imaging is widely used to evaluate macrostructural changes such as T2 hyperintense lesions, T1 black holes, gadolinium-enhancing lesions, and brain volume loss.3,4 Although conventional MR imaging analysis has been used for years to assess the disease burden, it cannot fully explain the degree of neurologic dysfunction. The lack of correlation between neurologic disability and conventional MR imaging measures is commonly described as the “clinicoradiologic paradox.”4
DTI has been previously used to assess the integrity of brain tissue and to probe specific white matter tracts.5⇓⇓⇓⇓⇓⇓–12 Prior studies have evaluated microstructural changes of the corticospinal tract (CST) in MS and the association between diffusivity of the CST and measures of neurologic disability.5,7,13⇓⇓⇓–17 However, a fundamental limitation of DTI is that the data analysis approximates the water diffusion dynamics within brain tissue as being a Gaussian process, though considerable non-Gaussian diffusion effects are observed throughout the brain. Hence, DTI does not fully characterize water diffusion in the brain. Diffusional kurtosis imaging (DKI)18 is a clinically feasible diffusion MR imaging method, which extends the DTI model to include non-Gaussian diffusion effects.18⇓–20 As a result, DKI has the potential to provide more sensitive biomarkers for probing microscopic structural changes occurring in the normal-appearing white matter (NAWM), which could lead to better predictive biomarkers for disease progression. Although DKI has been applied to MS in a few preliminary studies,18⇓⇓⇓–22 the potential of DKI to aid in the assessment of neurologic disability in MS is still not well-established.
The aim of this study was to examine the associations between DKI-derived diffusion metrics of the corticospinal tract and physical disability in patients affected by MS, as measured by the Extended Disability Status Scale (EDSS).23 Our hypothesis was that DKI-derived metrics have stronger associations with neurologic dysfunction than DTI metrics.
Materials and Methods
Participants
The study was approved by the institutional review board, who exempted the study from requiring individual patient consent. We retrospectively reviewed the PACS for all patients with multiple sclerosis who underwent brain MR imaging during an 18-month period. Inclusion criteria were the following: 1) age between 18 and 70 years; 2) diagnosis of multiple sclerosis according to established diagnostic criteria2; 3) brain MR imaging performed according to our standard multiple sclerosis protocol, including DKI; and 4) neurologic evaluation within 1 month of the MR imaging available in the electronic medical record (baseline visit). On the basis of the clinical phenotype, patients were categorized as having clinically isolated syndrome, relapsing-remitting MS, primary-progressive MS, secondary-progressive MS, or unknown type of MS.24 We excluded patients with history of neurologic disorders other than multiple sclerosis. We also excluded all imaging datasets degraded by bulk head motion or other artifacts. The degree of neurologic impairment was assessed by using the Kurtzke EDSS during the baseline visit (EDSS0). If subsequent clinical neurologic encounters were documented in the electronic medical record, then we recorded the EDSS score for the neurologic visit 12 months after brain MR imaging (EDSS12 m).
MR Imaging
Brain MRIs were performed on a 1.5T Avanto MR imaging scanner (Siemens, Erlangen, Germany). A sagittal T1-weighted MPRAGE (TR/TE/TI = 1900/2.91/1100 ms, flip angle = 15°, acquisition matrix = 225 × 199, FOV = 256 × 256 mm2, section thickness = 1 mm) and an axial FLAIR sequence (TR/TE/TI = 8000/88/2372 ms, flip angle = 180°, matrix = 424 × 512, FOV = 220 × 220 mm2, section thickness = 5 mm) were performed. Axial diffusion-weighted images were acquired with 3 b-values (0, 1000, and 2000 s/mm2) along 30 diffusion-encoding directions with a single-shot twice-refocused spin-echo EPI sequence with NEX = 1 (NEX = 10 for b=0). Imaging parameters of the diffusion sequence were the following: voxel size = 3 × 3 ×3 mm3, number of sections = 40, TR/TE = 5500/99 ms, FOV = 222 × 222 mm2, acquisition matrix = 74 × 74, bandwidth/pixel = 1325 Hz, acceleration factor = 2, acquisition time ≈ 7 minutes.
Data Processing
The Lesion Segmentation Tool toolbox (http://www.applied-statistics.de/lst.html), an open-source toolbox for SPM8 (http://www.fil.ion.ucl.ac.uk/spm/software/spm12), specifically the lesion-growth algorithm, was used to segment T2 hyperintense lesions from the MPRAGE and FLAIR images (κ value = 0.2).25 Then, a neuroradiologist blinded to all clinical information inspected each lesion mask to ensure accurate lesion segmentation. With MRIcron software (http://www.nitrc.org/projects/mricron/),26 we calculated total white matter lesion volume for each patient.
With Diffusional Kurtosis Estimator software27 (Version 2.6, https://www.nitrc.org/projects/dke/) implemented in Matlab (MathWorks, Natick, Massachusetts), we calculated the diffusion and kurtosis tensors on a voxel-by-voxel basis. Parametric maps for the following metrics were obtained from the DKI dataset: 1) diffusivity metrics: fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (λ‖), and radial diffusivity (λ⊥) diffusivity; 2) kurtosis metrics: mean kurtosis (MK), axial (K‖) and radial (K⊥) kurtosis. MK is the average kurtosis over all diffusion directions, K‖ is the kurtosis in the direction of the diffusion tensor eigenvector with the largest diffusion eigenvalue (typically along the direction of the axons), and K⊥ is the average kurtosis over all directions perpendicular to the diffusion eigenvector with the largest eigenvalue (typically all directions perpendicular to the axons).18 FA maps were normalized to the Montreal Neurological Institute standard space FA template, a high-resolution average of 58 well-aligned good-quality FA images from healthy male and female subjects between 20 and 50 years of age, at 1 × 1 × 1 mm3 resolution. The resulting normalization parameters were then applied to the remaining diffusion maps and to the lesion masks. The white matter skeleton was obtained by using Tract-Based Spatial Statistics (TBSS; http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/TBSS) in FSL (FA threshold, ≥0.4).28 The corticospinal tract volumes of interest were obtained from the WM skeleton with the Johns Hopkins University White Matter Tractography Atlas,29 after masking out T2 hyperintense areas of individual patients (Fig 1). As a result, the CST VOI only included the NAWM of the CST. Then, average diffusion values of the CST VOIs were computed for all diffusion metrics and subjects by using Matlab.
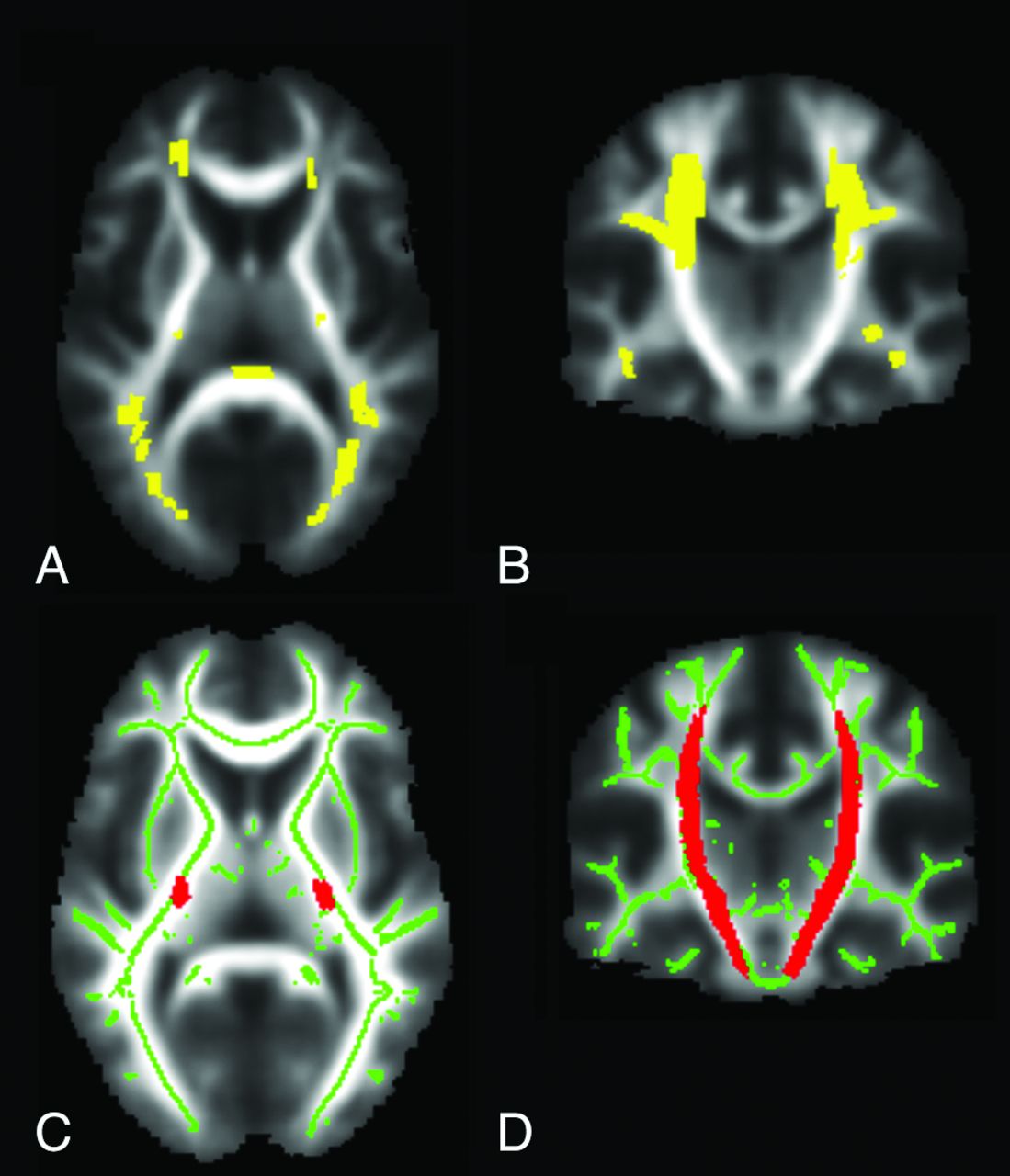
White matter lesion mask (yellow) of a representative patient with multiple sclerosis overlaid on axial (A) and coronal (B) mean fractional anisotropy images. The mean fractional anisotropy skeleton (green) and the Johns Hopkins University White Matter Tractography Atlas corticospinal tract (red) are overlaid onto the mean axial (C) and coronal (A) fractional anisotropy images. The white matter skeleton was obtained with FSL Tract-Based Spatial Statistics. The corticospinal tract VOIs were obtained from the white matter skeleton with the Johns Hopkins University White Matter Tractography Atlas, after masking out T2 hyperintense areas of individual patients. All images are in the Montreal Neurological Institute standard space.
Statistical analyses were conducted with SPSS (Version 22; IBM, Armonk, New York). Due to the small number of men in the study, sex differences in EDSS were examined with an independent-samples Mann-Whitney U test. Pearson correlations were examined between CST diffusion metrics and EDSS at baseline and at the 12-month follow-up to characterize basic relations among variables. Results of the Pearson correlations were considered statistically significant with P < .05, corrected for multiple comparisons with the false discovery rate method.30 A linear regression equation with the stepwise method was calculated to evaluate the relationships among EDSS at baseline, the dependent variable, and the independent variables entered in the following order: age, white matter lesion volume, and CST diffusion parameters. Additional linear regressions were also calculated to evaluate the associations between the same independent variables and EDSS at the 12-month follow-up and changes in the EDSS score between baseline and 12-month follow-up. Before the linear regression equation calculation, multicollinearity among independent variables was assessed with the variance inflation factor (VIF). Independent variables were excluded from the analysis when the VIF was >10.31 The results of the linear regression analyses were considered statistically significant at P < .05.
Results
Demographic and Clinical Characteristics
Forty patients with MS were included in this study. Table 1 shows demographic, clinical, and conventional MR imaging characteristics of the entire cohort and of the subgroup of 28 patients with 12-month follow-up. There was no significant difference in EDSS scores between men and women at baseline (women: median = 3, range = 1–8, n = 33; men: median = 3, range = 1–3.5, n = 7; U = 138.5, P = .421) and at the 12-month follow-up (women: median = 3, range = 0–9, n = 24; men: median = 6, range = 1–6, n = 4; U = 39.5, P = .590). Patients had a disease duration of at least 1 year since their first symptom before the brain MR imaging. The exact duration of disease was not documented in the chart for 3 patients. Of the 40 patients, 25 were receiving disease-modifying treatments, which included interferon β (n = 13), glatiramer acetate (n = 8), natalizumab (n = 3), and fingolimod (n = 1).
Patient clinical characteristics and imaging metrics
Imaging Data
Table 2 demonstrates the correlations among age, T2 lesion volume, CST diffusion metrics, EDSS0, and EDSS12 m (Fig 2). Analyses of the multicollinearity among independent variables resulted in inclusion in the regression model of the following independent variables with a VIF of <10: age (VIF = 1.30), T2 white matter lesion volume (VIF = 1.42), CST MK (VIF = 5.89), CST K‖ (VIF = 2.21), and CST K⊥ (VIF = 5.43). FA, MD, λ⊥, and λ‖ were excluded from the analyses due to a VIF of >10. Then, a linear regression analysis was performed to evaluate the relationship between EDSS0 and the following variables: age, T2 white matter lesion volume, MK, K‖, and K⊥. A significant regression equation was found (F [2,37] = 8.875, P = .001) with an R2 of 0.324. K⊥ (β= −0.329, P = .023) and age (β = 0.399, P = .007) were the only variables significantly associated with EDSS0 (Table 3). A linear regression analysis was performed to evaluate the relationship between EDSS12 m and the same variables (age, T2 lesion load, and CST diffusion metrics obtained at baseline). A significant regression equation was found (F [1,26] = 12.014, P = .002) with an R2 of 0.316. K⊥ (β = −0.562, P = .002) was the only variable to have a significant association with EDSS12 m (Table 3). A linear regression analysis was also performed to evaluate the relationship between change in the EDSS score (baseline EDSS versus 12-month follow-up EDSS) and the same independent variables. None of the variables had significant associations with change in the EDSS score.
Correlations between EDSS and age, T2 lesion volume, and diffusion metrics

Scatterplots for the Expanded Disability Status Scale at the time of the brain MR imaging versus radial diffusivity (A) and radial kurtosis (C) of the corticospinal tracts, and EDSS at the follow-up visit 12 months after the brain MR imaging versus radial diffusivity (B) and radial kurtosis (D) of the corticospinal tracts in patients with MS.
Linear regression analyses: coefficients table
Discussion
We conducted a retrospective study designed to explore the hypothesis that DKI-derived metrics of the CST have stronger associations with physical disability than DTI-derived metrics in patients with MS. We have preliminarily found that K⊥ of the CST has an association with physical disability. Associations were found between DKI-derived metrics and neurologic disability at the time of brain MR imaging, as well as with the degree of disability at 12-month follow-up. Due to the retrospective nature of our study, however, our results will require validation with future prospective studies. If our preliminary observations are confirmed, DKI-derived metrics may play an important role in improving our understanding of physical disability and prognosis, as well as in guiding treatment considerations in multiple sclerosis.
The correlations between DTI-derived measures of CST integrity and functional disability in MS have been previously evaluated.7,9,10,13,16,32 Lin et al13 found greater MD and radial diffusivity in the normal-appearing CST in patients with MS than in healthy controls. Prior studies found significant associations between DTI-derived measures of CST integrity and functional disability. Bergsland et al32 found significant correlations between the EDSS and diffusivity measures, including FA, MD, λ⊥, and λ‖ for the NAWM CST. Tovar-Moll et al5 found an inverse association between CST FA and EDSS when correcting for lesion volume. Other authors found only trends for an inverse correlation between EDSS and CST FA in MS14,15 or found weak correlations between EDSS and DTI metrics of the CST (MD, λ⊥, and λ‖).9 Reich et al16 did not find significant differences in FA, MD, λ⊥, and λ‖ for the CST among patients with various degrees of ankle dorsiflexion impairment. Harrison et al33 found that DTI indices of the CST were not able to predict EDSS scores. Overall, prior study results demonstrated that conventional DTI measures may have an association with physical disability, but this relationship has not been consistently demonstrated in the literature. Here, we report associations of conventional DTI metrics for the CST with EDSS, which confirm prior studies, and extend prior investigations by demonstrating significant correlations between kurtosis metrics, especially K⊥, and EDSS.
The diffusional kurtosis metrics are complementary to the diffusion tensor metrics and provide microstructural information that more comprehensively characterizes brain tissue microstructure.18 A few studies have previously evaluated the use of DKI-derived metrics in the characterization of demyelinating disease in animal models and in patients affected by MS. Using the cuprizone mouse model of CNS demyelination, Falangola et al34 evaluated the associations between DKI-derived metrics in cuprizone-induced chronic demyelination of the corpus callosum and morphologic WM alterations associated with myelin pathology. DKI-derived metrics were found to have greater sensitivity than conventional DTI parameters in the detection of cuprizone-induced demyelination of the anterior corpus callosum. Guglielmetti et al35 found that MK and K⊥, but not DTI-derived parameters, were sensitive to cuprizone-induced cortical alterations. Yoshida et al19 have conducted ROI-based quantitative analyses of MK for 24 cerebral NAWM regions in 11 patients with MS. The average MK for the NAWM was found to be lower in patients with MS than in healthy controls. Raz et al21 evaluated the signal characteristics of the spinal cord by using DKI and found that MK was lower in patients with MS than in healthy controls. Abnormal DKI-derived metrics of the NAWM were found in patients with MS but not in individuals with neuromyelitis optica.22 Bester et al20 applied DKI to the evaluation of cortical gray matter microstructural changes and found that decreased cortical MK was associated with poor performance on the Delis-Kaplan Executive Function System test (r = 0.66). De Kouchkovsky et al17 assessed white matter integrity in MS by using DKI-derived white matter integrity metrics, specifically axonal water fraction, intra-axonal diffusivity, radial and axial extra-axonal diffusivity, and tortuosity of the extra-axonal space. The authors found a moderate association between axonal water fraction in the corpus callosum and the EDSS score (ρ = −0.39). Our study design differs from the methodology used by de Kouchkovsky et al. In fact, our approach was to study the associations between physical disability and pure diffusion metrics of the CST, such as mean kurtosis and radial kurtosis, as opposed to model-dependent quantities such as axonal water fraction.
These prior studies have shown that kurtosis parameters provide more comprehensive information about brain tissue microstructure than that available with conventional DTI.18 It is important to determine whether this enhanced sensitivity to microstructural changes provided by DKI translates into improved disability prediction. Our work demonstrates promising relations between DKI-derived diffusion metrics for the CST and clinical disability. In this retrospective cohort, age and K⊥ were associated with neurologic disability and accounted for approximately 32% of the variability of EDSS scores at baseline. We also found that K⊥ was the only parameter significantly associated with disability at the 12-month follow-up examination and accounted for about 32% of the variability of EDSS scores. If the associations between K⊥ and disability are validated in future larger prospective studies, these metrics may ultimately prove to be powerful adjuncts to the clinical assessment of patients with MS.
Histopathology and MR imaging studies have shown that the NAWM is affected, to a lesser extent, by the same pathologic processes that are found in MS lesions, specifically inflammation, demyelination, microglial activation, axonal injury, Wallerian degeneration, and macrophage infiltration.36⇓⇓–39 The pathologic basis of the stronger association between K⊥ and physical disability in MS requires further determination. K⊥ is the average kurtosis over all directions perpendicular to the diffusion eigenvector with the largest eigenvalue (typically all directions perpendicular to the axons). We hypothesized that the stronger association between physical disability and K⊥ than between other diffusion metrics may reflect a greater sensitivity of K⊥ to early pathologic changes of the NAWM, possibly myelin breakdown resulting in demyelination or hypomyelination or an increase of membrane barriers due to microgliosis.34,35 Unfortunately, pathologic findings for the NAWM are not available for this patient cohort. Future studies on the correlations between DKI parameters and pathologic findings for the NAWM in MS will help clarify the histopathologic basis of our preliminary observations.
An alternative approach to DKI for quantifying diffusional non-Gaussianity is to fit the diffusion MR imaging signal to a stretched exponential model.40 However, this model does not allow the estimation of kurtosis,18 and it is less appropriate for white matter because incorporating the effects of diffusion anisotropy is challenging.41 Biexponential fitting of the diffusion MR imaging signal is also feasible. This is fully consistent with DKI but requires the acquisition of more diffusion-weighted data than the truncated cumulant expansion signal model conventionally used with DKI (as in the present study).18
This study has limitations. First, it was a retrospective study that evaluated a relatively limited number of 40 patients, which precluded analysis of data in patients with relapsing-remitting, primary-progressive, and secondary-progressive MS separately. Twelve-month clinical follow-up information was available for only 28/40 patients (70%). We also did not evaluate the subsequent temporal evolution of the observed CST diffusion measures. Finally, while the EDSS is an effective tool widely used in clinical trials to assess the severity of MS, it is heavily weighted toward ambulation, and the multiple sclerosis functional composite may be a more sensitive method to evaluate disease progression.28
Conclusions
We have found significant associations between the K⊥ of the CST and disability in MS. DKI metrics were found to have stronger associations than DTI metrics with measures of disability in MS. It is important that this work be validated in future prospective studies with larger sample sizes.
Acknowledgments
The authors gratefully acknowledge Ali Tabesh for his contributions to study design, image postprocessing, and data analysis and Dr. Aljoeson Walker for performing the neurologic examinations.
Footnotes
Disclosures: Jens H. Jensen—OTHER RELATIONSHIPS: I am a coinventor on US Patent 8811706 that covers one of the imaging methods investigated in this article (DKI). The patent is owned by a former employer (New York University), but I could be entitled to a share of any royalties at some point. To date, I have not received royalties from this patent. Joseph A. Helpern—UNRELATED: Grant: The Litwin Foundation*. Neal U. Hatch—UNRELATED: Support for Travel to Meetings for the Study or Other Purposes: partial reimbursement of travel expenses provided by the department. *Money paid to the institution.
Paper previously presented in part at: Annual Meeting of the International Society for Magnetic Resonance in Medicine and European Society for Magnetic Resonance in Medicine, May 10–16, 2014; Milan, Italy; Annual Meeting of the American Society of Neuroradiology and the Foundation of the ASNR Symposium, May 17–22, 2014; Montreal, Quebec, Canada; and Annual Meeting of the American Society of Neuroradiology and the Foundation of the ASNR Symposium, May-18–23, 2013; San Diego, California.
REFERENCES
- Received December 28, 2016.
- Accepted after revision March 14, 2017.
- © 2017 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.