
Abstract
BACKGROUND AND PURPOSE: CT-guided head and neck biopsies can be challenging due to the anatomy and adjacent critical structures but can often obviate the need for open biopsy. A few studies and review articles have described approaches to biopsy in the head and neck. This retrospective study evaluated technical considerations, histopathologic yield, and safety in CT-guided head and neck core needle biopsies.
MATERIALS AND METHODS: A retrospective review of head and neck biopsies performed from January 2013 through December 2019 was conducted. Clinical diagnosis and indication, patient demographics, mass location and size, biopsy needle type, technical approach, dose-length product, sedation details, complications, diagnostic histopathologic yield, and the use of iodinated contrast were recorded for each case.
RESULTS: A total of 27 CT-guided head and neck core needle biopsies were performed in 26 patients. The diagnostic sample rate was 100% (27/27). A concordant histopathologic diagnosis was obtained in 93% (25/27) of cases. There was a single complication of core needle biopsy, a small asymptomatic superficial hematoma.
CONCLUSIONS: Percutaneous CT-guided biopsy of deep masses in the head and neck is safe and effective with careful biopsy planning and has a high diagnostic yield that can obviate the need for open biopsy.
ABBREVIATION:
- CTCAE
- Common Terminology Criteria for Adverse Events
In the United States, >60,000 new cases of head and neck cancer will be diagnosed in 2020, comprising approximately 4% of new cancer cases in men.1 Many of these cancers that arise within the oropharynx are diagnosed by an otolaryngologist using direct visualization by laryngoscopy. Most of the superficial soft-tissue masses in the neck are biopsied either by palpation2 or sonographic guidance.3⇓⇓-6 The masses within the deep spaces of the neck are most commonly biopsied using CT guidance. In the past, many of these deep head and neck biopsies were performed using CT guidance and fine-needle aspiration techniques.7⇓⇓-10 More recent articles have described the use of CT guidance and spring-loaded core biopsy needles.11⇓⇓⇓-15
Compared with other biopsies, deep head and neck masses are difficult to biopsy safely and effectively due to the critical anatomy in the region of the biopsies, including nerves, vessels, and salivary glands. Despite the critical anatomy, there are few reported serious complications in head and neck soft-tissue biopsies.16
In general, the demand for percutaneous CT-guided biopsies continues to increase due to the evolving requirements of clinical treatment and study protocols. The well-published safety, efficacy, and high histopathologic yield obviates the need for open biopsies; however, there are relatively few publications addressing CT-guided soft-tissue core biopsies of the head and neck.
The purposes of this retrospective original research are to describe and expand technical considerations, including the use of CT angiography, and to demonstrate the high histopathologic yield and safety of CT-guided head and neck soft-tissue core biopsies.
MATERIALS AND METHODS
Patient Selection and Study Enrollment
Approval from the institutional review board was granted with a waiver of informed consent for this Health Insurance Portability and Accountability Act–compliant retrospective study. Correlating data were collected for all CT-guided head and neck biopsies performed at Washington University in St. Louis from January 2013 to December 2019 included in this study. These data were acquired by searching the radiology information system for neck biopsy cases using a combination of Current Procedural Terminology codes for neck/thorax biopsy (21550), soft-tissue mass biopsy (20206), and CT guidance (77012) and using the following search terms: “neck biopsy,” “parapharyngeal space,” “masticator space,” “carotid space,” and “paraspinal.” Inclusion criteria were CT guidance, suspicion of either benign or malignant tumor, soft-tissue mass, core needle biopsy, and follow-up available in the electronic medical record. CT-guided biopsies for infection or superficial neck lymph nodes were excluded. For each case, we collected and evaluated the following data: patient demographics, clinical diagnosis and indication, mass size and location, biopsy needle type/gauge, technical approach, number and length of each soft-tissue biopsy, CT dose-length product, sedation details, and diagnostic histopathologic yield. Procedural complications were documented according to the Common Terminology Criteria for Adverse Events (CTCAE), Version 5.0.17 Patients were clinically monitored for at least 1 hour after each procedure for evidence of acute complications such as hematoma formation or neurologic injury. A short-term follow-up phone call between 1 and 3 days following the procedure was used to document any additional short-term complications. The electronic medical records were also reviewed for evidence of delayed complications within 30 days of the biopsy.
Biopsy Procedure
All procedures were performed by 1 of 4 board-certified fellowship-trained musculoskeletal radiologists with 12, 10, 7, and 6 years of experience. Twenty-three of the 27 procedures were performed with conscious sedation; 2/27, with general anesthesia; and 2/27, with local anesthetic only. In most cases, a 1:1 mixture of bupivacaine 0.25% and lidocaine 1% was first administered for subcutaneous and deep anesthesia. The average sedation time for the conscious sedation cases was 43 minutes. The average intravenous fentanyl and midazolam dosages for the conscious sedation cases were 159.8 µg and 2.6 mg, respectively. For the biopsies, Bard Mission (Bard Peripheral Vascular) or Achieve (CareFusion) spring-loaded coaxial biopsy needle systems were used. The choice of needle gauge was based on the relative proximity of the lesion to important neurovascular structures, the space available to avoid those structures, and the ability to maneuver the needle into the lesion without injuring those structures. For lesions with minimal clearance between the needle path and a critical neurovascular structure, a smaller gauge needle was chosen, either 18 or 20 ga. The outer introducer needle was placed just proximal to the target mass followed by the coaxial placement of the spring-loaded biopsy needle into the mass. In 2 cases, the Arrow OnControl battery-powered bone biopsy system (Teleflex) was used to access the soft-tissue lesions. Table 1 describes in detail the different biopsy needles used for lesion biopsy. The most common needle used was 14 gauge in 14/27 biopsy procedures. The average number of biopsy cores acquired was 4.4 (range, 2–9). Patient positioning on the table was dependent on the location of the head and neck lesion and the approach used to perform the biopsy.
Biopsy needles by size and brand used for 27 biopsies
There are multiple described approaches for biopsies in the head and neck, depending on the locations of the masses.18⇓⇓-21 A brief description and the approximate needle course for the different biopsy approaches are presented in Fig 1. Biopsy approaches for the patients in our group included the following: anterior 7/27, paramaxillary 2/27, posterior 5/27, retromandibular 2/27, submastoid 8/27, and subzygomatic/sigmoid notch 3/27 (Table 2). The anterior approach was used for lesions in the perivertebral, anterior cervical, prevertebral, visceral (Fig 2), and pharyngeal spaces. The paramaxillary approach was used for lesions in the masticator and parapharyngeal spaces (Fig 3). The posterior approach was used for posterior perivertebral lesions. The retromandibular approach was used for parapharyngeal space lesions (Fig 4). The submastoid approach was used for lesions in the perivertebral, parapharyngeal, and carotid spaces (Fig 5). The subzygomatic approach was used for lesions in the masticator space.

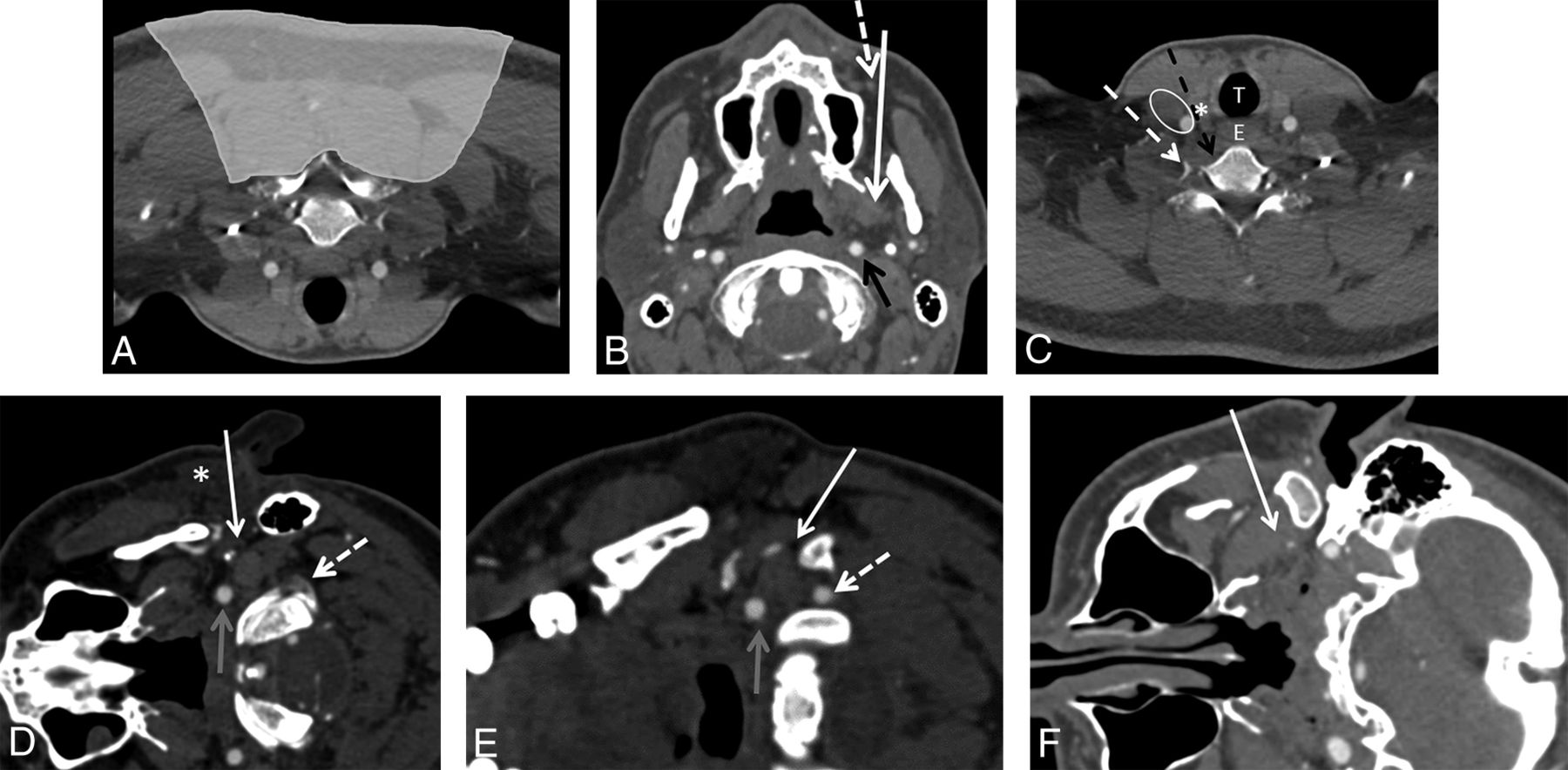
CT-guided neck biopsies can be performed using multiple different approaches depending on the location of the lesion. In almost all approaches, there are critical neural and vascular structures adjacent to the needle tract. A, CT angiogram of the neck flipped vertically to depict prone positioning for a posterior-approach neck biopsy. Neck biopsies in the shaded region would commonly be performed using a posterior approach. In the shaded region, there are no critical neurovascular structures. B, CT angiogram soft-tissue-windowed image of the neck with the patient in a supine position for the paramaxillary approach (white arrow). The needle course is between the maxillary sinus and the mandible adjacent to the facial artery (dashed arrow) through the buccal space. This approach can be used for lesions in the buccal, masticator, parapharyngeal, retropharyngeal, and carotid sheath spaces. The critical structures to avoid include the facial artery (dashed arrow) and the internal carotid artery (black arrow). C, CT angiogram of the neck with the patient in a supine position for anterior-approach biopsies, which can be either medial (black dashed arrow) or lateral (dashed white arrow) to the carotid and jugular vasculature (white oval). These approaches can be used for lesions in the infrahyoid neck and lower cervical vertebrae. The critical structures to avoid include the carotid artery, jugular vein, and vagus nerve (white oval); the trachea (white T); the esophagus (white E); and the thyroid gland (white asterisk). CT angiograms of the neck with the patient in a decubitus position: This positioning will be used for the retromandibular (D), submastoid (E), and subzygomatic (F) approaches denoted by white arrows. Note that the needle will sometimes pass through a portion of the parotid gland for the retromandibular approach (white asterisk). Critical structures to avoid include the carotid (gray arrows) and vertebral arteries (dashed white arrows) with the retromandibular and submastoid approaches and the retromandibular vein in the retromandibular approach because of its proximity to the facial nerve. These approaches can be used for lesions in the deep parotid, parapharyngeal, pharyngeal, and retropharyngeal spaces.

A 74-year-old woman with a previously excised papillary thyroid carcinoma also treated with radioactive iodine who has a new mass in the right visceral space of the neck adjacent to the thyroidectomy bed. Axial contrast-enhanced CT image (A) from a neck CT demonstrates an enhancing mass (black asterisk) in the right visceral space abutting the trachea (white asterisk), the esophagus (white oval), and the right internal jugular vein (dashed white arrow). Intraprocedural axial CT soft-tissue-windowed image (B) with the core biopsy needle in place. An anterior approach was chosen to pass just medial to the internal jugular vein (dashed white arrow), just lateral to the trachea (white asterisk), and stopping short of the esophagus (white oval). The histopathology from the biopsy was recurrent papillary thyroid carcinoma.

A 75-year-old woman with previously excised and re-excised left base-of-tongue and retromolar squamous cell carcinoma. Axial contrast-enhanced neck CT (A) and fused PET/CT (B) images demonstrate an enhancing FDG avid mass (black asterisk) in the left masticator space. A paramaxillary approach was chosen to perform the biopsy (C). The histopathology from the biopsy was recurrent squamous cell carcinoma. With this biopsy, the facial artery is medial to the needle-entry site just anterior to the maxilla and is not problematic for the needle path.

A 69-year-old woman with an incidentally found right-neck mass on a cervical spine MR imaging. Axial T2-weighted MR image (A) from a cervical spine MR imaging demonstrates an indeterminate T2-hyperintense mass (white asterisk) at the deep margin of the parotid gland, centered within the parapharyngeal space posterior to the masticator space. Intraprocedural contrast-enhanced soft-tissue-windowed CT image (B) with the patient in the left lateral decubitus position. Note the internal carotid artery (white arrow) and other vascular structures including the retromandibular vessels adjacent to the mandibular ramus (white dashed arrow). Intraprocedural axial CT bone-windowed image (C) with the core biopsy needle in place (black arrow). A retromandibular course with the entry point posterior to the ear was chosen to access the mass. The needle path is to avoid the vascular structures adjacent to the mandibular ramus, including the retromandibular vein, but anterior to the styloid process (black dashed arrow) and internal carotid artery (approximately at the site of the black asterisk but occult on noncontrast CT). The pathology was adenoid cystic carcinoma.

A 25-year-old man with neurofibromatosis type 1, new vagus nerve–related symptoms, and a enlarging painful left carotid space mass. Axial T1-weighted fat-suppressed postcontrast MR image (A) from a neck MR imaging demonstrates an enhancing carotid space mass (black asterisk). Intraprocedural contrast-enhanced soft-tissue-windowed CT image (B) with the patient supine but with the head turned to the right. Note that the mass (white asterisk) is located between the internal carotid (black arrow) and vertebral (black dashed) arteries and is pushing the carotid artery anteriorly. Intraprocedural axial CT soft-tissue-windowed image (C) with the core biopsy needle in place (white arrow). A submastoid approach was chosen to avoid the carotid and vertebral arteries. The histopathology from the biopsy was neurofibroma. Given the progressive symptoms, concern for sampling error, and the high risk given the diagnosis of type neurofibromatosis 1, the mass was excised and final pathology was plexiform neurofibroma containing focal areas of low-grade malignant peripheral nerve sheath tumor.
Neck biopsy approach
CT angiography was performed immediately before the biopsy when the pathway to the soft-tissue mass included important vascular structures, to better delineate the vascular anatomy and plan the safest biopsy route while minimizing the risk of vascular injury. Of the 27 biopsy procedures, 10 had corresponding CT angiograms with a dose average of 80 mL of ioversol contrast (Optiray 350; Mallinckrodt) given intravenously (Figs 4 and 5).
RESULTS
Patient Characteristics
A total of 26 patients underwent 27 CT-guided head and neck soft-tissue biopsies. Fifty-four percent of the patients were men, and 46% were women. The age range of the patients was from 3 months to 77 years of age, with an average age of 54.7 years. The clinical concern in these cases was for primary tumor in 52% (14/27), locoregional recurrent disease in 33% (9/27), or metastatic disease in 15% (4/27). One complication of core needle biopsy occurred. This was a small intraprocedural hematoma (CTCAE grade 1), which was asymptomatic and required no further treatment or follow-up. Additionally, there was an adverse event in which the patient developed new asymptomatic atrial fibrillation with a rapid ventricular response (CTCAE grade 3) during positioning and the initial contrast-enhanced CT scan for localization of tumor. This was before administration of sedation medications and beginning the biopsy procedure. This patient was transported to the emergency department for heart rate control, and the biopsy was performed at a later date without complications.
Lesion Characteristics and Histopathology
The average size of the biopsied masses measured in the longest axis of each lesion was 33 mm, ranging between 14 and 71 mm. The locations of the lesions were the following: the anterior cervical space, 11% (3/27); carotid space, 11% (3/27); masticator space, 19% (5/27); parapharyngeal space, 22% (6/27); perivertebral space, 26% (7/27); pharyngeal space, 4% (1/27); prevertebral space, 4% (1/27); and visceral space, 4% (1/27) (Table 3).
Anatomic location of the target mass in 27 biopsy procedures
A sufficient sample was obtained for histopathologic diagnosis in 100% (27/27) of the biopsies. The pathology obtained was malignant in 16/27 biopsies and benign in 11/27 biopsies. Two of the 11 benign biopsies were found to be discordant with the clinical impression and repeat biopsy results were subsequently found to be malignant. One was initially diagnosed as fibrosis with a foreign body giant cell reaction and was later found to be recurrent squamous cell carcinoma on a repeat CT-guided biopsy 6 weeks later. The second was initially diagnosed as benign neurofibroma, but at excision, it was found to have areas of malignant peripheral nerve sheath tumor within the lesion. The remaining 9 benign lesion biopsies either demonstrated no concerning change on imaging follow-up in 56% (5/9) or were confirmed benign by excision in the remaining 44% (4/9). The most common malignant lesion was squamous cell carcinoma, found in 8 patients (Table 4). The overall concordance of the biopsies was 93%.
Histopathologic results of CT-guided head and neck biopsies
CT Radiation Dose
The dose-length product ranged from 76 to 2790 mGy × cm, with an average of 533 mGy × cm. When we considered the most recent biopsies, specifically from January 2015 to December 2019, which account for 89% (24/27) of all biopsies performed, there was a decreased average dose-length product of 455 mGy × cm. The highest dose-length product recorded was 2790 mGy × cm. This was performed before increased awareness of scanning parameters, advanced scanner technology, as well as institutional emphasis on decreasing diagnostic and procedural radiation doses.
DISCUSSION
Masses in the head and neck arise in multiple different anatomic spaces and have a wide variety of tumor histopathologies. Diagnosis and treatment require a multidisciplinary approach, which is constantly evolving.22⇓-24 Often, the tissue required for diagnosis is acquired by a subspecialty-trained radiologist, particularly when the mass is located within a deep neck space requiring CT guidance for biopsy access.
Multiple publications have demonstrated the safety and utility of soft-tissue biopsies in general, but few have focused specifically on the deep head and neck.7⇓⇓⇓⇓⇓⇓⇓-15 Most complications reported in the literature in these studies are minor, including small hematoma, pain, vasovagal reaction, and minor infection.7⇓⇓⇓⇓⇓⇓⇓-15 Another more rarely described complication is seeding of tumor along the biopsy needle tract. A MEDLINE data base search between 1970 and 2014 found 7 reported cases of tumor seeding, 5 with fine-needle aspiration and 2 with core needle biopsy, in the 610 articles reviewed.25 These findings are similar to those in our study in which we report 1 minor complication of the biopsy procedure, no tumor seeding complications, and 1 adverse event before beginning the biopsy procedure, which was unlikely related to the procedure, given that this occurred before a needle was placed in the neck. The only reported major complication related to a CT-guided head and neck biopsy in the literature was an internal maxillary artery pseudoaneurysm presenting 3 months after the CT-guided fine-needle aspiration. This was thought to be due to an increased risk from prior radical neck surgery and radiation therapy, leading to abnormal neoangiogenic vascularity or large-vessel vasculopathy.16
Given the relatively high-stakes anatomy in the head and neck, choosing the appropriate anatomic approach to safely perform the biopsy is of the utmost importance. There are multiple described approaches to head and neck masses, with some overlap in the ability to access a deep neck space.18⇓⇓–21 For example, pathways to reach the parapharyngeal, masticator, and pharyngeal spaces may include paramaxillary, retromandibular, submastoid, and subzygomatic approaches. Thus, it is important to fully evaluate the preprocedural imaging for the location of vessels, nerves, salivary glands, and salivary ducts to find the safest and most direct needle course. The CT angiography technique increases the certainty and safety of the needle path chosen for the procedure, particularly when positioning for the procedure is different from the standard supine position typically used for CT imaging and when there are arteries in or directly adjacent to the targeted mass. This technique has been previously described in cervical spine biopsies,26 but not in biopsies of head and neck masses. All except 2 of the 27 cases were performed with either conscious sedation or local anesthesia, increasing the safety of the biopsy in this patient population, which is typically considered at higher risk for general anesthesia.
The choice of biopsy technique, fine-needle aspiration versus core needle biopsy, is often dependent on the institution. At our institution, core needle biopsies are preferred by the pathologist when feasible for increased diagnostic certainty. In previous clinical series, the yield of both CT-guided fine-needle aspiration and core biopsy of the head and neck soft tissues is varied. In the largest study of 216 patients who underwent CT-guided fine-needle aspiration, a diagnostic sample was obtained in 90% of patients, with a concordant diagnosis in 88% of cases.9 Studies of CT-guided core biopsies have reported diagnostic yields ranging from 73% to 96%.12⇓⇓-15 Compared with these prior CT-guided soft-tissue mass biopsy series, our diagnostic yield is similar-to-slightly higher, with 100% of samples sufficient for histopathologic diagnosis and a concordant diagnosis in 93% (25/27) of all biopsies. This result may be due to the larger average needle gauge used in our study, most commonly 14 gauge, and the higher average number of core specimens obtained of 4.4.
CONCLUSIONS
This original research demonstrates the safety and efficacy of CT-guided percutaneous core biopsy for deep soft-tissue masses in the head and neck, obviating the need for open biopsies and their associated risks in locations not easily accessible by palpation, sonography, or laryngoscopy. It also describes the use of CT angiography for vessel localization and mapping before needle placement following patient positioning on the procedural table to reduce the risk of vascular injury.
Footnotes
Disclosures: Travis J. Hillen—UNRELATED: Consultancy: Medtronic, SI BONE, Ultragenyx Pharmaceutical, ERT, Comments: paid consultant for studies not related to published work. Jack W. Jennings—RELATED: Consulting Fee or Honorarium: Bard/BD and Stryker, Comments: Both are for consultation for the bone biopsy system and nothing to do with this article; UNRELATED: Consultancy: Merit, Medtronic, Comments: Merit contract ended June 30, 2020, Medtronic monitoring for OPuS 1 spine ablation trial.
References
- Received April 30, 2020.
- Accepted after revision July 7, 2020.
- © 2020 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Ultrasound Fusion-Guided Core Needle Biopsy for Deep Head and Neck Space Lesions: Technical Feasibility, Histopathologic Yield, and Safety
- Percutaneous CT-Guided Core Needle Biopsies of Head and Neck Masses: Review of 184 Cases at a Single Academic Institution, Common and Special Techniques, Diagnostic Yield, and Safety