
Abstract
BACKGROUND AND PURPOSE: Cavernous malformations occur most often in the brain but can occur in the spinal cord. Small studies of patients with familial cerebral cavernous malformations suggested a prevalence of spinal cord cavernous malformations of 20%–42%. We aimed to review our familial cohort and prospectively estimate the prevalence of spinal cord cavernous malformations.
MATERIALS AND METHODS: We initially reviewed our familial cerebral cavernous malformations cohort for spinal cord cavernous malformations and reviewed clinical spine MR imaging examinations for sequence sensitivity. We then prospectively performed research MR imaging of the spinal cord in 29 patients from the familial cohort to estimate the prevalence.
RESULTS: Gradient-based sequences identified the most spinal cord cavernous malformations on clinical MR images, forming the basis for developing our screening MR imaging. Screening spinal cord MR imaging demonstrated a prevalence of 72.4%, and a positive correlation with patient age and number of cerebral cavernous malformations.
CONCLUSIONS: Spinal cord cavernous malformations occur commonly in the familial cerebral cavernous malformation population. Gradient-based sequences are the most sensitive and should be used when spinal cord cavernous malformations are suspected. This study establishes the prevalence in the familial population at around 70% and supports the idea that this condition is a progressive systemic disease that affects the entire central nervous system.
ABBREVIATIONS:
- CM
- cavernous malformation
- CCM
- cerebral cavernous malformation
- SCCM
- spinal cord cavernous malformation
- MEDIC
- Multi-Echo Data Image Combination
Cavernous malformations (CMs) are dilated capillary-type low-flow vascular malformations, which are prone to repeated hemorrhage and growth over time.1⇓⇓⇓-5 Cerebral cavernous malformations (CCMs) occur with a prevalence of about 0.5% in the general population.1,2,6 About 80% of CCMs are sporadic, solitary, and often closely associated with a developmental venous anomaly, and about 20% of CCMs are familial/syndromic.1,2 Mutations that lead to familial CCM syndrome can occur in 3 genes (CCM1 or KRIT1, CCM2, and CCM3 or PDCD10) with an autosomal dominant transmission.2,4,7⇓-9 There is a particularly high prevalence of familial CCM syndrome (CCM1-common Hispanic mutation) in southwest North America due to a founder effect in early Hispanic settlers.1,2,4,9 Spinal cord cavernous malformations (SCCMs) are less common than CCMs and have been considered rare, with relatively less attention in the CCM literature and most reported cases being sporadic nonfamilial SCCMs.10⇓⇓⇓⇓⇓⇓⇓⇓-19 A 2009 report on a single Italian family with familial CCM found SCCMs in 5 of 12 patients (41.7%), 2 of which were discovered clinically and 3 of which were discovered with screening MR imaging (3 of 6 screened patients had SCCMs).20 An additional 2017 report on 13 patients with familial CCM found upper SCCMs in 3 patients (23.1%).21 Given these estimates of SCCM prevalence in small sample sizes, and what we had been encountering in our cohort, we aimed to systematically study SCCMs in our familial CCM1 cohort. We initially reviewed our familial CCM cohort retrospectively and evaluated the sensitivity of various MR imaging sequences for detecting SCCMs; we then prospectively imaged the spinal cord in 29 patients to estimate the prevalence of SCCMs in familial CCM. We expected to find a high prevalence of SCCMs in this patient population and that the number of SCCMs would positively correlate with the number of brain CCMs and age, supporting the idea of familial CCM as a progressive systemic disease that affects the entire central nervous system.
MATERIALS AND METHODS
The study was institutional review board compliant, and all subjects gave informed consent to participate. An overall outline of the study is demonstrated in Fig 1.

Flow chart of the study.
Initial Retrospective Review
Our research cohort consisted of 280 patients with familial CCM syndrome participating in a prospective longitudinal study. This cohort consists of patients with the CCM1 common Hispanic mutation. Patients must have a genetic diagnosis of CCM, or meet 2 of the 3 criteria of a clinical diagnosis of CCM, have evidence of multiple CMs on MR imaging, or a family member with a diagnosis of CCM1. We initially retrospectively reviewed the records of patients in this research cohort to identify patients with known SCCMs as an estimate of the lower bound of prevalence in our cohort.
MR Imaging Sequence Sensitivity
Based on this initial retrospective analysis, we set out to determine the sensitivity of sequences to determine our protocol for screening the spinal cord for SCCMs. Fifteen of the patients had clinically performed cervical spine MR images available, for which the number of SCCMs visible on each sequence was analyzed. Sequences consisted of sagittal T1 TSE, sagittal T2 TSE, and axial T2 Multi-Echo Data Image Combination (MEDIC; Siemens). A sagittal 3D MEDIC was also performed in 8 of the patients. SWI was performed in 2 cases, but proved significantly limited by artifact and was not analyzed for sequence sensitivity. Anonymized and randomized MR imaging sequences were presented to 2 attending neuroradiologists, who separately recorded the number of SCCMs seen on each individual sequence. This was followed by a consensus review to agree upon the number of SCCMs detected for each sequence. The proportion of SCCMs detected for each sequence was calculated compared with the total number detected across all sequences, and the sensitivity of detecting SCCMs was calculated relative to the total number of SCCMs.
Screening Spinal Cord MR Imaging
After the initial review of our cohort and using what we had learned about sequence sensitivity, we prospectively screened the spinal cord with MR imaging in 29 of the patients in the study. We offered research MR imaging of the cervical and thoracic spine to consecutive patients who were returning for research brain MR imaging; 30 patients were scheduled for cervical and thoracic spine MR imaging and 29 patients completed the MR imaging. Four patients in the prospective screening group were also in the group of 34 patients found to have SCCMs on retrospective review. Research MR imaging was performed on a 3T Skyra scanner (Siemens) and was set up as sagittal T1 TSE (TE, 10 ms; TR, 647), sagittal T2 TSE (TE, 110 ms; TR, 2500 ms), and sagittal 3D MEDIC (TE, 11 ms; TR, 28 ms) performed in 2 segments (cervical spine through upper thoracic spine with a field of view of 280 mm, and upper thoracic spine through the conus with a field of view of 340 mm) (Fig 2). The 3D MEDIC sequence was reformatted into 1 -mm axial images for review.

Sagittal T1 TSE (A), sagittal T2 TSE (B), sagittal 3D MEDIC (C), and axial reformat of the 3D MEDIC (D), from spinal cord screening research MR imaging and corresponding SWI from brain research MR imaging done on the same day (E). On sagittal 3D MEDIC (C), arrowsdenote small SCCM. D, Axial reformat shows small CM in the right aspect of the spinal cord (arrow), corresponding to the more inferior of the 2 lesions. E, SWI of the brain shows multiple CMs which are typical of familial CCM syndrome.
An attending neuroradiologist reviewed the research MR imaging examinations, and SCCMs were characterized by number, size, and imaging appearance. We also recorded and characterized any vertebral intraosseous vascular malformations on screening MR imaging as these have recently been reported to be of high prevalence in patients with CCM.22 We tested whether SCCM counts were associated with age and total brain CCM count by using the Spearman rank correlation.
RESULTS
In the overall cohort study of 280 patients, 61.4% of the patients enrolled were female, and 72.4% of the spine MR imaging screened patients were female, which was not statistically significantly different (P = .14). The mean age for the 280 patients enrolled in the overall cohort study was 39.0 years (SD 19.7); the mean age for the 29 patients prospectively screened with spine MR imaging was higher at 47.4 years (SD 18.4) (P = .009).
Initial Retrospective Review
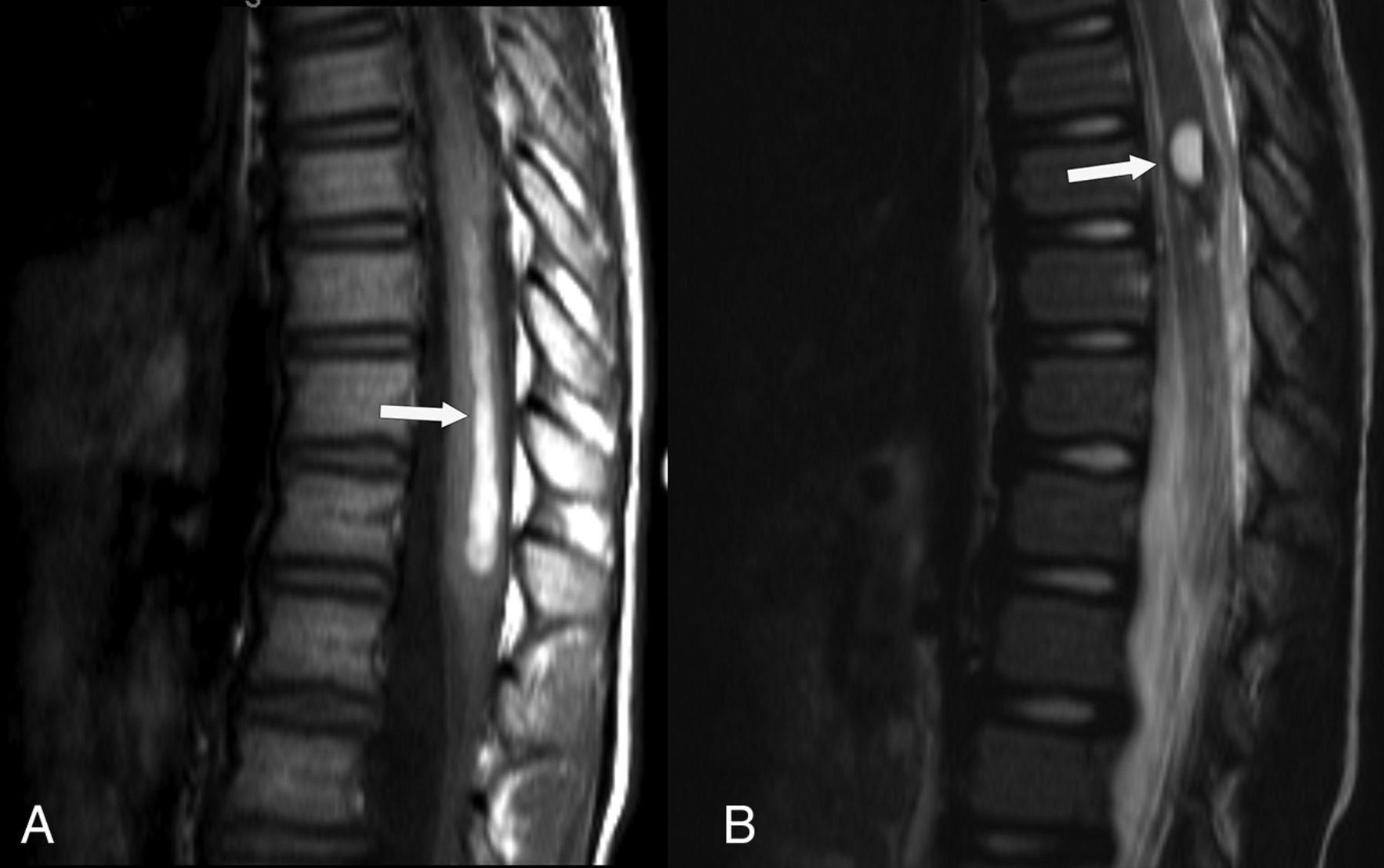
On retrospective review of the familial CCM cohort, we found that 34 patients (12.1%; 95% CI, 8.6%–16.6%) had SCCMs: 17 were identified in the upper cervical spinal cord on research brain MR imaging, and 23 were found on clinical spine MR imaging (6 in both groups). Seven of the 23 showed findings of acute spinal cord hemorrhage on MR imaging (Fig 3). Seven patients had surgery to remove the SCCM, 4 of whom had spinal cord hemorrhage. Nineteen patients were deemed to have clinical symptoms referable to the SCCM.

A, Sagittal T1 TSE and sagittal T2 TSE (B), from clinical MR imaging of the thoracic spine demonstrates spinal cord hemorrhage from a SCCM. On sagittal T1 TSE (A), there are T1 hyperintense blood products tracking down the thoracic spinal cord (arrow) toward the conus medularis. On sagittal T2 TSE (B), there are mixed-signal blood products (arrow) at the site of the spinal cord cavernous malformation.
MR Imaging Sequence Sensitivity on Clinical Cervical Spine MRI
Some SCCMs were visible on routine TSE sequences, but gradient-based techniques were more sensitive for detecting SCCMs (Table 1). Of the 15 patients with cervical spine MR imaging, we detected more of the 21 total SCCMs with the gradient-based MEDIC sequences than traditional T1 and T2 sequences (Table 1). Sagittal T1 TSE detected 14.3% (of total SCCMs), sagittal T2 TSE detected 28.6%, axial T2 TSE detected 23.8%, and axial T2 MEDIC detected 81.0% (including 4 of 8 SCCMs seen by 3D MEDIC) of the total SCCMs. 3D MEDIC, when performed, had detected the most SCCMs and had an advantage over 2D MEDIC in spatial resolution and permitted multiplanar reconstruction. Thus, 3D MEDIC was selected for use in our screening MR imaging of the spinal cord.
Analysis of sequence sensitivity for SCCM, retrospectively performed on 15 clinically performed cervical spine MR imaging studies
Screening MR Imaging of the Spinal Cord
In the prospective group of 29, the mean age was 46.3 (SD 18.8) and 21 (72.4%) were female. We found SCCMs in 21 of 29 patients (72.4%; 95% CI, 52.8%–87.3%) screened with the dedicated research spinal cord MR imaging (Table 2). The mean number of SCCMs per patient was 3.2 (SD 3.9, median 2, range 0–17). SCCMs were small with a mean axial diameter of 2.5 mm (SD 1.3, median 2, range 1–8 mm) (Fig 2) on the axial reformat of the 3D MEDIC. Only 2 of the larger SCCMs showed mixed T2 signal intensity (type II CMs), the rest showed only dark hemosiderin signal (type IV CMs).3 Only 20 of the 29 patients (69.0%; 95% CI, 49.2%–84.7%) had any vertebral intraosseous vascular malformation; while 11 of the 29 (37.9%; 95% CI, 20.7%–57.7%) had an atypical (T1 hypointense) intraosseous vascular malformation, and 16 of the 29 (55.2%; 95% CI, 35.7%–73.6%) had a typical (T1 hyperintense) intraosseous vascular malformation (Table 2). There was a strong, positive correlation between number of SCCMs and age (ρ = 0.748, P < .001) and between number of SCCMs and number of brain CMs (ρ = 0.649, P < .001). There was not a statistically significant correlation between the number of SCCMs and intraosseous vascular malformations.
Results of prospective screening MR imaging of the spinal cord
DISCUSSION
With prospective imaging to screen the spinal cord, we found SCCMs in 21 of 29 patients with familial CCM1, a prevalence of 72.4% (95% CI, 52.8%–87.3%). Prior reports of 5 of 12 patients (41.7%, 3 discovered with screening MRI), and 3 of 13 patients (23.1%) were higher than what was initially known in our cohort, but lower than what we found with screening MR imaging.20,21 Our study establishes an estimated prevalence of SCCMs in the familial CCM1 population of approximately 70%.
Our study demonstrates that SCCMs are indeed a common finding in patients with familial CCM and supports the idea of familial CCM syndrome as a progressive systemic disease that affects the entire central nervous system. We found an expected positive correlation of number of SCCMs with both patient age and number of intracranial CCMs. We also found a high prevalence of vertebral intraosseous vascular malformations (69%), including atypical (T1 hypointense) intraosseous vascular malformation in approximately 38% of the patients who underwent MR imaging screening, supporting the recent finding that these are common in patients with familial CCM.22
Many of the SCCMs that we found with screening were quite small (mean diameter of 2.52 mm) and we would not expect them to currently alter patient management. SCCMs were not commonly clinically discovered in our larger cohort (23/280 patients, 8.2%), and presenting with spinal cord hemorrhage (n = 7) and being operated on for SCCM (n = 7) were even rarer in our cohort. Currently, there are no guidelines to suggest screening the spinal cord for SCCMs in patients with familial CCM; if that were performed, we would expect that many, mostly small, SCCMs would be found as was the case in this study.2
Gradient-based MEDIC sequences were found to be more sensitive to the detection of SCCMs compared with T1 and T2 sequences (which detected only 14.3–28.6% of the SCCMs compared with the MEDIC sequences). Additionally, 3D MEDIC was more sensitive for SCCM detection compared with 2D MEDIC, which detected only 4/8 SCCMs in patients with both 2D and 3D imaging. Many SCCMs were visible only as small foci of susceptibility, accounting for the limited visibility on T2 and T1 sequences. SWI, of proved superiority for detection of CMs in the brain as compared with T2 or GRE sequences, was limited in the spine by artifact.23,24 3D MEDIC is an isotropic, high-resolution gradient-based technique that can quickly image a long section of the spine in a single, narrow, sagittal acquisition with multiplanar reconstructions, which we found to be ideal for identifying SCCMs, and thus we utilized this sequence in our screening spinal cord research MR imaging. When there is suspicion for CMs, using sensitive sequences in the spine and brain is necessary because the identification of a second CM changes the presumptive diagnosis from sporadic to genetic disease. This distinction has important implications for the individual, their family, and for genetic counseling.
Limitations of this study include the mix of clinically and incidentally discovered SCCMs in the baseline part of the study, the varied imaging techniques used for clinical and research imaging, and the limited collected clinical data. Also, because our cohort is patients with CCM1 and does not include patients with CCM2 and CCM3, we are thus unable to extrapolate our results to patients with CCM2 and CCM3 familial CCM. Screening of the spinal cord as we did with our spinal cord research MR imaging by using only sagittal imaging would potentially be impractical in clinical practice where other spinal pathology may also be important to adequately image. However, if imaging is performed primarily to identify SCCMs, then performing a sequence sensitive to small foci of susceptibility as we did with our 3D MEDIC sequence, provides a highly sensitive evaluation.
CONCLUSIONS
SCCMs are a common feature of familial CCM syndrome. We have established an estimate of the prevalence of SCCMs in the familial CCM1 cohort at approximately 70%. SCCMs can present clinically, including with hemorrhage, or can be found incidentally in these patients. Optimal technique, including gradient-based sequences such as 3D MEDIC, should be used for spinal cord imaging if SCCMs are suspected. This study supports the idea of familial CCM as progressive systemic disease that affects the entire central nervous system.
Footnotes
Grant funding from the National Institute of Health-National Institute of Neurological Disorders and Stroke (grant number U54 NS065705), Radiology Department Seed Grant, and the Cody Unser First Step Foundation.
Disclosures: Marc Mabray—RELATED: Grant: NIH NINDS.* Jeffrey Nelson—RELATED: Grant: NIH.* Atif Zafar—RELATED: Grant: National Institute of Health–National Institute of Neurological Disorders and Stroke, Comments: National Institute of Health–National Institute of Neurological Disorders and Stroke (grant number U54 NS065705), Radiology Department Seed Grant, and the Cody Unser First Step Foundation. UNRELATED: Employment: UNM Hospital. Helen Kim—RELATED: Grant: NIH*; UNRELATED: Consultancy: Recursion Pharmaceuticals, Comments: Consulting services for clinical advisory board; Grants/Grants Pending: NIH.* Leslie Morrison—RELATED: Grant: NINDS. Blaine Hart—RELATED: Grant: NIH.* *Money paid to institution.
Portions of this research previously presented at: Annual Meetings of the American Society of Neuroradiology Annual Meeting, May 23–26, 2016, Washington, DC; American Society of Spine Radiology Annual Symposium, February 18–21, 2016, Bonita Springs, Florida; Western Neuroradiological Society Annual Meeting October 11–14, 2018, Dana Point, California; and Annual Angioma Alliance Cerebral Cavernous Malformations Scientific Meeting, November 8–9, 2018, Silver Spring, Maryland.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received February 27, 2020.
- Accepted after revision March 19, 2020.
- © 2020 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.