
Abstract
Summary: CT of a patient with conductive hearing loss showed a small vascular structure leaving the carotid canal and passing through the stapes to join the facial nerve canal. The small bony channel paralleled the anterior tympanic segment of the facial nerve, continuing beyond the geniculate ganglion into the middle cranial fossa. Otoendoscopic photography documented the presence of a persistent stapedial artery.
A persistent stapedial artery (PSA) is a rare vascular anomaly with a prevalence calculated to be 0.48% in a histopathologic study of 1000 temporal bones (1). The PSA can occur as an isolated anomaly or in association with an aberrant carotid artery.
Case Report
A 7-year-old girl presented with mild conductive hearing loss. A temporal bone CT (Fig 1 and 2) revealed a small channel leaving the intratemporal carotid canal, proximal to the turn from the vertical-to-horizontal segment. This presumed vascular structure continued along the promontory to the stapes. The vessel entered a separate channel along the inferior margin of the anterior tympanic segment of the facial nerve canal (Fig 2). This channel could be followed beyond the geniculate ganglion curving laterally to the floor of the middle cranial fossa. There was absence of foramen spinosum. There were no other anomalies of the internal carotid artery (ICA) or facial nerve. Otoendoscopic examination revealed a pulsatile vessel running vertically over the promontory and passing between the stapedial crura, consistent with a persistent stapedial artery (Fig 3).

Axial Images (A–H), from superior to inferior. The small vascular channel can be seen leaving the vertical carotid at G (arrow), and can be followed along the lower medial wall of the middle ear (D–F) (arrows). Level C is at the plane of the stapedial crura. The vessel cannot be clearly separated from the anterior crus of the stapes. After following the facial nerve canal, the small vascular channel reaches the middle cranial fossa at level B (arrowhead). Level A represents the position of the geniculate ganglion turn of the facial nerve canal

Coronal images (A–D), from posterior to anterior. The narrow presumed vascular structure is seen at B (arrowheads), coursing along the promontory. At level A, the small vascular structure (arrows) crosses the oval window niche, to end in the lower inferomedial aspect of the tympanic segment of the facial nerve canal. This small channel is also seen at B (arrow). More anteriorly (C and D), the small canal (arrows) courses just inferior to the tympanic segment of the facial nerve canal in a separate channel as it passes toward the floor of the middle cranial fossa. The small soft-tissue structure immediately inferior to this canal is the tensor tympani muscle within its semicanal
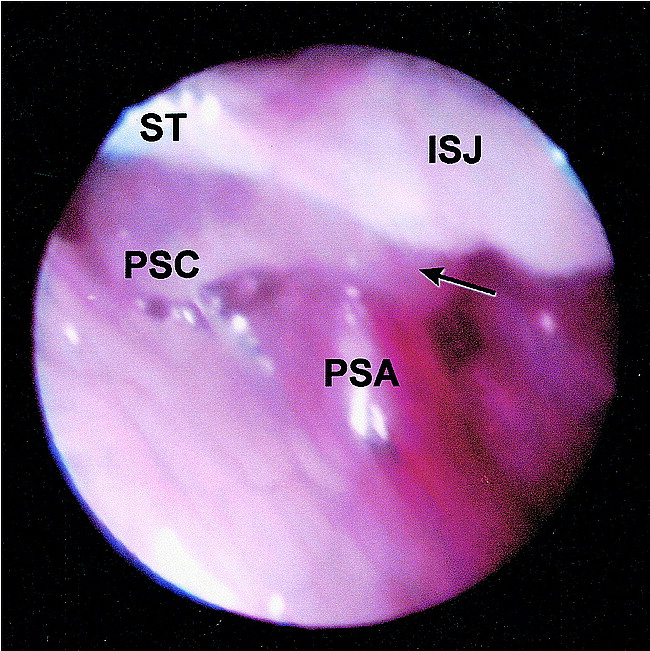
Otoendoscopic view of the right tympanic cavity.The PSA passes between the stapes crura. (Anterior stapedial crus [arrow]. Posterior stapedial crus [PSC]; stapedial tendon [ST]; incudostapedial joint [ISJ]. Reprinted with permission. from: Bhattacharyya N, Poe DS. Otoendoscopic view of a persistent stapedial artery. Otolaryngol Head Neck Surg 1999;120:923
Discussion
In the embryo, a series of branchial arches develops. Each of these arches has, at least transiently, an embryonic vascular arch crossing from the ventral to the dorsal aorta on each side of the midline. Most of the upper embryonic aortic arch segments are transient, disappearing along with much of the ventral and dorsal embryonic aortic system. The second arterial arch (also called the hyoid artery) is one of the remnants of these structures that partially persists and contributes to the definitive arterial system. As this arch regresses, the stapedial artery originates from its anterior portion. The stapedial artery normally penetrates the stapedial anlage, and its distal branches form precursors of the external carotid artery system supplying the orbit, meninges, and lower face (2). Progressive atrophy of the stapedial artery leaves the small caroticotympanic artery inferiorly, and possibly the superior tympanic artery superiorly (3).
The posterior division of the upper branch of the stapedial artery forms the middle meningeal artery (MMA). With the normal atrophic process, the distal portion of the MMA becomes irrigated by the internal maxillary artery through the foramen spinosum. If this transition fails to occur, the arterial bed of the middle meningeal artery will be supplied by communication with the ophthalmic artery or by a PSA. In both cases, absence of the foramen spinosum is expected (4).
The inferior segment of the PSA is probably formed by enlargement of either the caroticotympanic or the inferior tympanic artery. The superior continuation of the PSA eventually reaches the MMA, and its precise course beyond the crura of the stapes has been described in several ways. Both the superficial petrosal artery and the superior tympanic artery normally leave the MMA just inside the foramen spinosum. Reversal of flow and enlargement of either could represent the superior continuation of the PSA.
The superficial petrosal artery normally enters and follows along the facial nerve canal. In the case where it constitutes the superior continuation of the PSA, an enlargement of the facial canal would be expected.
The superior tympanic artery normally enters the temporal bone via a small canaliculus close to the facial hiatus, following the course of the lesser petrosal nerve. Descriptions indicate that the stapedial artery passes in a channel parallel to the facial nerve or actually may extend into the canal for a brief part of its course. It then enters the middle ear and continues toward the stapes.
In the current case, it is probable that the inferior portion of the PSA was formed by enlargement of the caroticotympanic artery. Since the PSA was contained in a channel at least partially separated from the facial canal, the stapedial artery would be the probable connection to the intracranial MMA (Fig 4B).

A, Schematic representation of the normal anatomy of the ICA and part of the tympanic arterial plexus.
B, Schematic representation of a persistent stapedial artery not associated with an aberrant ICA. There is enlargement of the caroticotympanic artery, as in our reported case. Alternatively, the inferior tympanic artery may form the inferior segment of the PSA. In the latter case, enlargement of the inferior tympanic canaliculus is expected. There is no foramen spinosum in either situation.
C, Schematic representation of a PSA associated with an aberrant ICA. There is absence of the vertical portion of the ICA. The inferior tympanic artery and canaliculus are enlarged. In this theory, there is reversal of the direction of flow and enlargement of the caroticotympanic artery. There is no foramen spinosum. (Modified from reference 3).
A PSA may be an isolated anomaly or may occur in association with an aberrant ICA (Fig 4C). When associated with an aberrant carotid artery, there is apparent absence of the vertical intrapetrosal portion of the ICA, and the “aberrant carotid” is formed by enlargement of both inferior tympanic and caroticotympanic arteries (3). The inferior tympanic artery becomes the proximal portion of the carotid, anastomosing with the more distal caroticotympanic artery. Flow is reversed in the caroticotympanic artery, completing the connection with the horizontal portion of the intrapetrosal ICA. In this case, the PSA leaves the carotid from the aberrant segment and continues superiorly to supply the MMA (3).
A PSA can cause conductive hearing loss and has been described as a cause of pulsatile tinnitus. Although no ill effects have been reported from ligation of the PSA (4), experience is limited. If ligation is considered, an arteriogram is obtained to ensure that the artery does not represent an end artery or to provide a substantial supply to sensitive tissue. In the present case, a conductive loss on the opposite side had been corrected by release of an ossified mallear ligament, and resection of the aberrant artery on the right side was not planned.
This vascular anomaly can be associated with other middle ear abnormalities, most commonly involving the stapes, facial nerve, or ICA. A PSA may also be present in trisomy 13, 15, and 21, as well as in Paget's disease, otosclerosis, thalidomide deformities, anencephaly, congenital immunodeficiency, and neurofibromatosis (2, 5).
Intraoperative diagnosis of a PSA is the rule. This report demonstrates that temporal bone CT can predict the anomalous vessel prior to tympanotomy.
The imaging findings of a PSA are: 1) a small canaliculus leaving the carotid canal; 2) a linear structure crossing the middle ear over the promontory; 3) an enlarged facial nerve canal or a separate canal parallel to the facial nerve; and 4) absence of the foramen spinosum.
Footnotes
↵1 Address reprint requests to Hugh D. Curtin, MD, Chief of Radiology, Massachusetts Eye and Ear Infirmary, 243 Charles Street, Boston, MA 02114.
- Received November 29, 1999.
- Accepted after revision March 10, 2000.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}
{kind=link}
{kind=link}