
Abstract
Summary: Idiopathic hypertrophic cranial pachymeningitis is a rare inflammatory disease with diffused involvement of the dura. Often, the definite diagnosis is made immediately with biopsy and the involved dura is removed surgically. Consequently, extensive preoperative imaging studies usually are not available. We reviewed a case of idiopathic hypertrophic cranial pachymeningitis and collectively summarized the interesting features from the 7 years preceding surgical treatment. These chronologic imaging findings with progressive intracranial involvement included dural thickening, dural mass, sinus thrombosis, and venous congestion constituted comprehensive pictures of idiopathic hypertrophic cranial pachymeningitis. The thickened dura may also at times mimic dural masses, such as en plaque meningioma.
Despite the upsurge of reported cases of idiopathic hypertrophic cranial pachymeningitis (IHCP) in recent years, there remains a lack of complete follow-up imaging studies throughout the progress of the disease. The reported imaging findings of IHCP include dural thickening, dural mass, sinus thrombosis, and venous congestion with white matter changes. These findings are extracted from different sporadic cases and probably represent only fragments of this disease during its active stage and do not depict the disease’s progression (1–3). The case reported herein illustrates the diversity of imaging findings associated with IHCP, ranging from isolated to widespread dural thickening and venous congestion caused by sinus thrombosis.
Case Report
This 23-year-old woman was first seen at the ophthalmology department in 1994. She suffered from decreased visual acuity of the right eye, pain sensation with ocular movement, and nonspecific headache. Mild ptosis, hyperemia, and decreased visual acuity of the right eye were present with no other cranial nerve involvement. CT revealed thickened right tentorium with attenuated homogeneous enhancement after the administration of contrast material. Increased enhancement at the right cavernous sinus was also seen (Fig 1). The cause of pachymeningitis, including sarcoidosis, tuberculosis meningitis, rheumatoid arthritis, syphilis, and occult malignancy, was sought and was excluded with negative laboratory results and absence of related clinical symptoms. With the impression of idiopathic pachymeningitis, the patient was given 20 mg of prednisolone daily. The patient was followed up in the outpatient clinic with remittent symptoms of headache, diplopia, and gradual loss of right vision after 1 year.

Contrast-enhanced CT scans show increased enhancement at the right cavernous sinus.
A, Contrast-enhanced CT scan obtained in 1994 shows that the right tentorium is thickened with homogeneous enhancement due to an inflammatory reaction of the pachymeninges.
B, Contrast-enhanced CT scan obtained at a more caudal level shows that involvement of the right cavernous sinus correlates with the patient’s symptom of optic neuropathy.
In May of 1994, the first series of MR imaging studies (Fig 2) showed similar lesions of the right tentorium thickening, as seen on CT scans obtained 1 year earlier. There was relative silence of disease progression until May of 1998 when the patient suffered from complete loss of right vision. The MR imaging study showed mild increasing thickness and enhancement of the left tentorium, with the right tentorium remaining unchanged with vivid involvement at the right cavernous sinus (Fig 3). Despite continuous prednisolone and azathioprine treatment, the patient suffered from rapid deterioration of left side vision, left tinnitus, and hearing loss in 6 months and development of right side tinnitus and hearing loss in 1.5 years, although the MR images obtained within 1 month showed regression of dural enhancement (Fig 4). Imaging studies performed within the next 1.5 years included two MR imaging examinations (Figs 5 and 6) of the brain. High resolution CT for bilateral temporal bones to monitor disease progression revealed evidence paralleling the clinical course, with findings of diffuse thickening of the posterior falx and the tentorium bilaterally, prominent bilateral cavernous sinus enhancement, and progressive change of bilateral mastoiditis (Table 1).

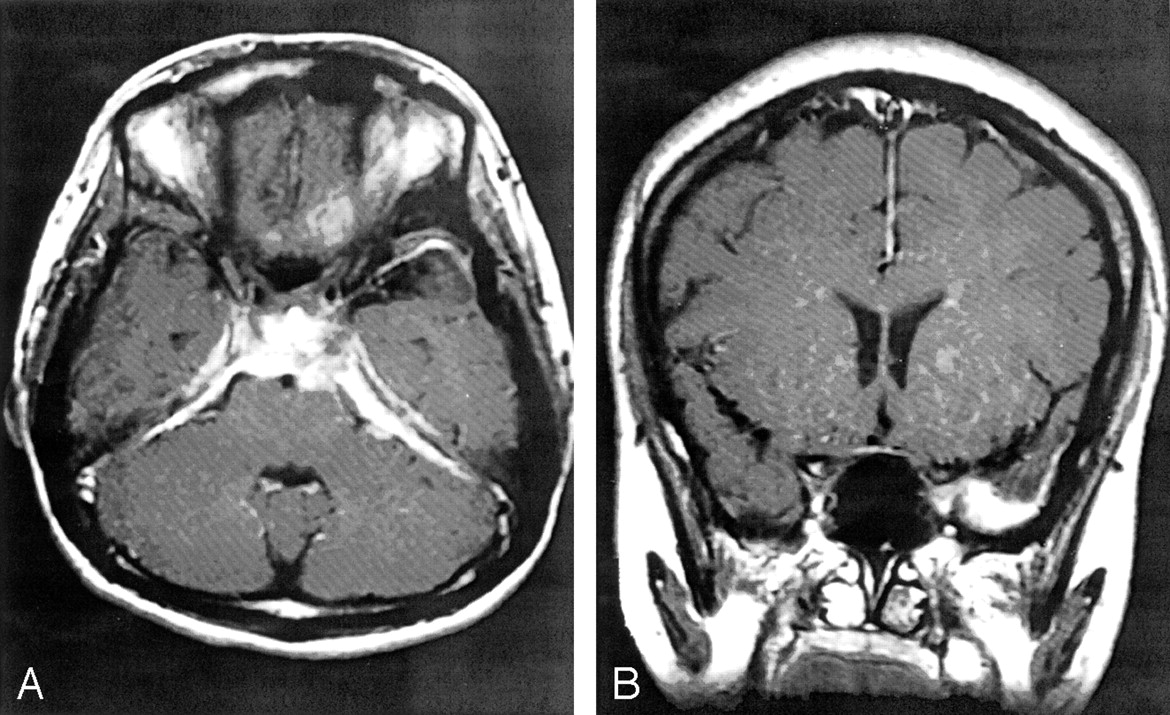
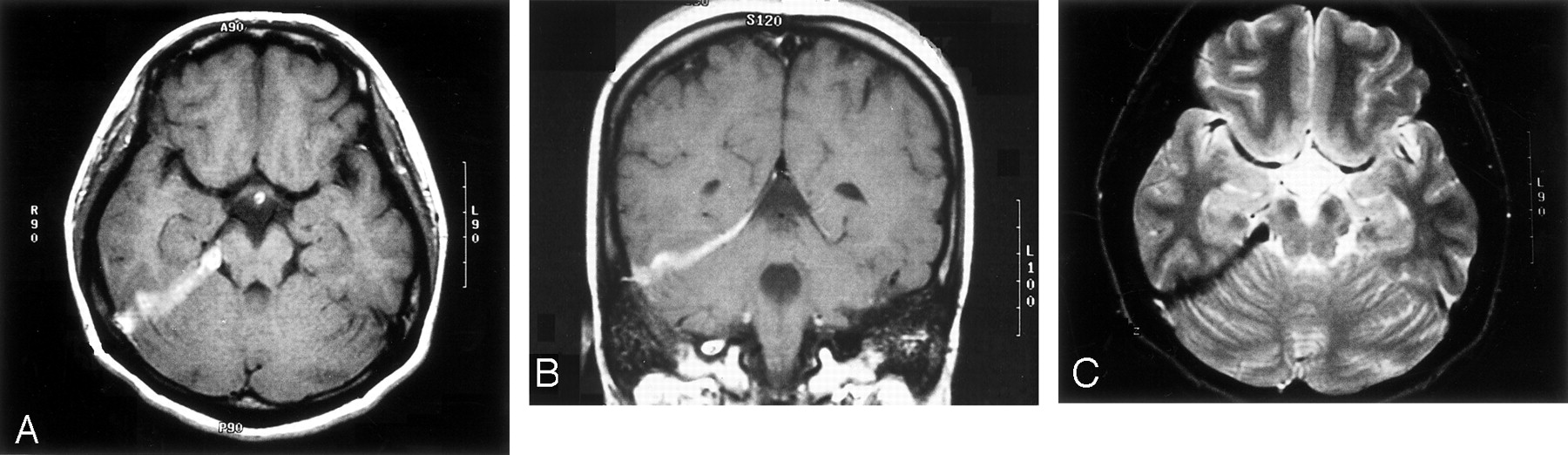
MR images obtained in 1995 show the thickened right tentorium. No significant progression of tentorium thickening or cavernous sinus enhancement is noted.
A, Thickened right tentorium is hypertense on axial T1-weighted image.
B, Thickened right tentorium is hypertense on coronal T1-weighted image.
C, Thickened right tentorium is hypointense on coronal T2-weighted image.
MR images show mild increasing thickness and enhancement of the left tentorium.
A, Axial T1-weighted contrast-enhanced MR image obtained in May of 1998, at the onset of blindness in the right eye and decreased left visual acuity, shows increased right cavernous sinus enhancement and more diffuse involvement of the tentorium bilaterally and of the posterior falx. Prominent dura enhancement can also be seen at the prepontine area, with mild compression of the brain stem.
B, Coronal T1-weighted contrast-enhanced MR image shows a focus of nodular dural enhancement at left temporal area, with minimal perifocal edema.

Coronal T1-weighted contrast-enhanced MR image obtained in June of 1998 shows regression of dural enhancement and the left temporal nodular mass with minimal dural thickening and edema.
Coronal T1-weighted contrast-enhanced MR image obtained in January of 1999 at the onset of right hearing impairment shows increased enhancement of the right mastoid area, although decrease in the tentorium and falx enhancement can be seen.

Coronal T1-weighted contrast-enhanced MR image obtained in December of 1999 shows increased intensity of the left mastoid at the onset of left hearing impairment.
Chronologic imaging findings with clinical correlations
The patient refused surgery and was regularly seen at the outpatient department with occasional flare-ups of symptoms. In July of 2001, the patient was hospitalized with new onset of delirium and confusion. An enhanced dural mass at the left temporal area with perifocal edema was shown on CT scans and MR images (Fig 7). Cerebral angiography (Fig 8), performed to exclude the possibility of en plaque meningioma, revealed poor filling of the straight sinus and a scanty stain on an angiogram of the left external carotid artery at the expected left temporal area. No hypervascular tumor stain was found; the faint stains noted were evidence of acute flare-up of pachymeningitis. Narrowed straight sinus, which correlates with dural sinus thrombosis, was also noted on MR venograms (Fig 9). Left temporal craniotomy was performed, with partial excision of brain and meningeal tissue to decompress the mass effect. The pathology slide of meninges showed thickened dura infiltrated by inflammatory lymphocytes, foamy histiocytes and plasma cells, and vascular proliferation (Fig 10). The accompanied brain tissue revealed only areas of necrosis and gliosis caused by venous congestion.

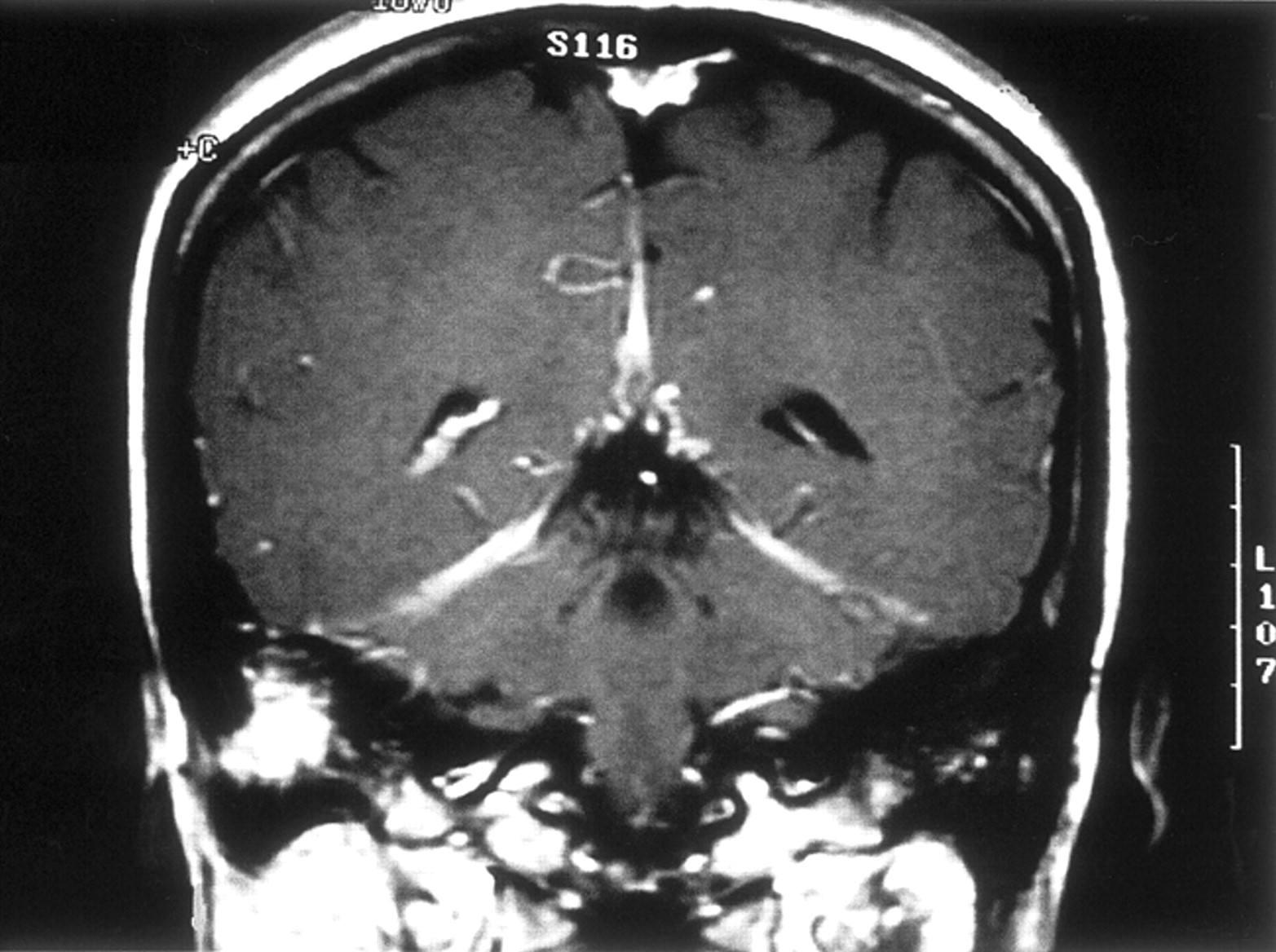
In July of 2001, the patient suffered from delirium and confusion. CT scan and MR image show enhanced dural mass at the left temporal area, with perifocal edema.
A, Contrast-enhanced CT scan shows an irregularly enhanced left temporal mass, with compression of the left temporal horn.
B, Coronal T1-weighted contrast-enhanced MR image shows an enhanced dural-based mass of the left tentorium, with an edematous change of the left temporal lobe. The mass is located in the same area as that revealed in Figure 3B.

Cerebral angiogram of the left internal carotid artery shows nonopacification of the straight sinus.
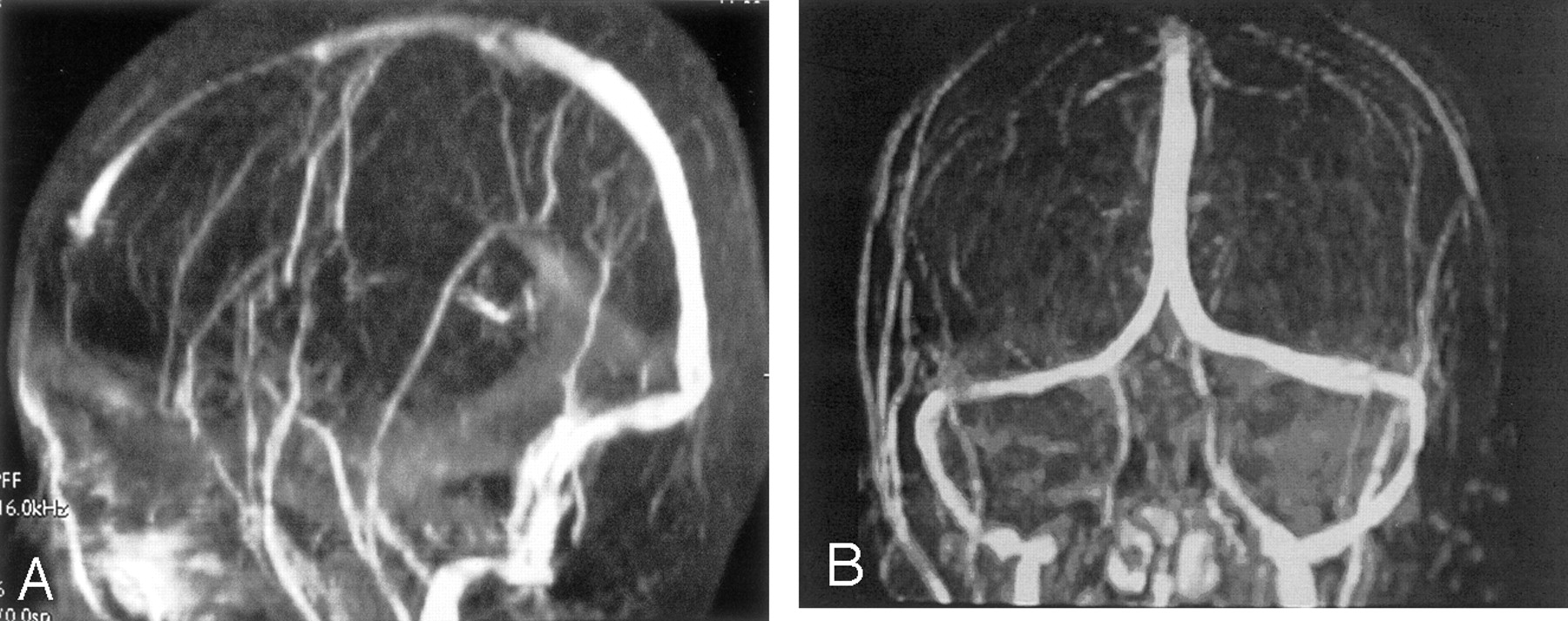
Narrowed straight sinus, which correlates with dural sinus thrombosis, was noted on MR venograms.
A, Sagittal MR venogram shows nonopacification of the straight sinus and indicates thrombosis.
B, Coronal view.
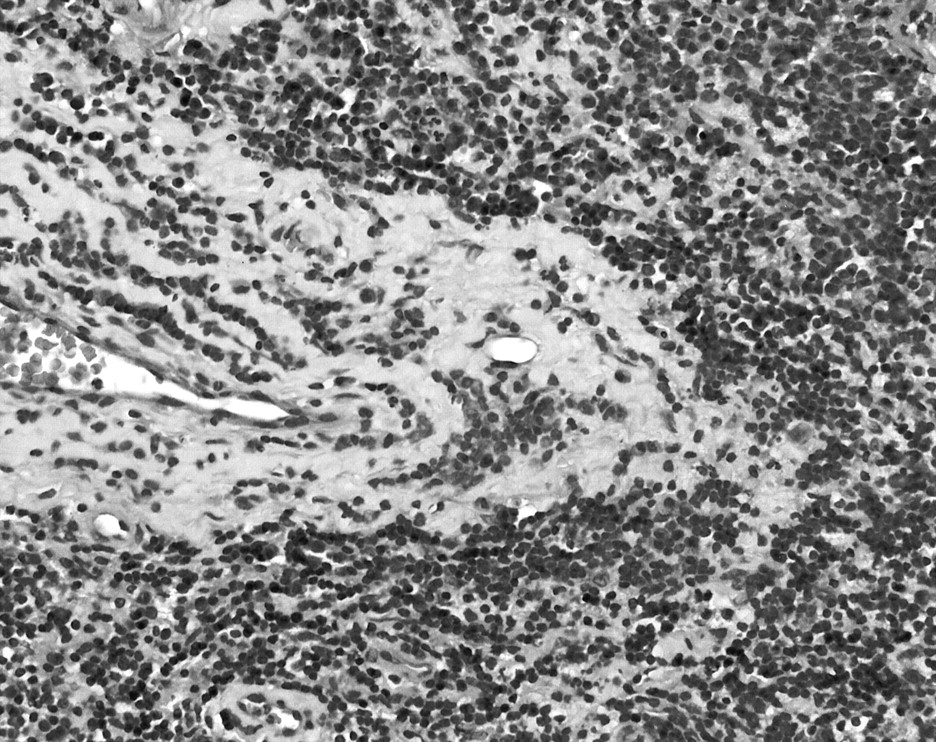
Pathology slide of the meningeal tissue from a left temporal craniotomy shows inflammatory cells with lymphoplasmacytic infiltration, foamy histiocytes, and vascular proliferation (hematoxylin and eosin; original magnification, ×150).
Discussion
We reviewed 12 cases of IHCP from three series of studies (1–3). None of these reports elaborated on long-term serial imaging studies of IHCP, although most patients experienced recurrent symptoms. Based on these reports, nonspecific symptoms of headache, nausea, and vomiting at the onset of the disease are the most common clinical presentations or are secondarily manifested with serous otitis and retro-orbital pain with later development of vision loss and hearing impairment. Cranial nerve VIII is the most frequently involved cranial nerve, and the next most frequently involved are cranial nerves V, VII, IX, X, and XII, with equal frequency (1). Three cases of monocular visual deterioration as a significant manifestation of the disease progression and two cases of optic neuropathy, which developed late in the course, have been reported (2). Visual deterioration or blindness has also been described in a few reports (4–8). Other clinical presentations include diabetic insipidus with hypophysitis, cerebellar ataxia, and sinus thrombosis. None of the reported cases show progress of IHCP with additional cranial nerve neuropathy or dural sinus thrombosis years after a lengthy quiescent period.
In the previously reported cases (3), tentorial involvement with variable extension to the neighboring dura mater was the common radiologic feature of pachymeningitis. With thickened dura mater composed of fibrosis and chronic inflammatory cells, inflammatory dura is usually hyperattenuated on unenhanced CT, strongly enhancing after contrast administration on both CT scans and MR images, and it is iso- to hypointense on T1-weighted MR images and hypointense on T2-weighted MR images with or without a hyperintense border (1, 2). The image study of IHCP can remain negative for ≤2 years before there is any significant finding (1). Linear thickening of the falx and tentorium is the most common finding, and the next most common finding is focal nodular thickening that simulates a dural mass. Other associated findings include mastoid effusion, sinus abnormality, cavernous sinus involvement, white matter edema, and hydrocephalus. As was seen in our case, enhancing cavernous sinus caused by local dural involvement parallels clinical worsening of visual acuity attributed to optic neuritis. The appearance of mastoiditis corresponding to the clinically manifested site of hearing loss may also be attributed to adjacent dura mater changes. Whether the causes of mastoiditis were the result of contiguous spread of the inflammatory process, local irritation of dura thickening, or direct invasion of cranial nerve VIII remains unclear. Additionally, a report of IHCP with localized cerebral or cerebellar white mater ischemic change has been presented; as seen in our case, it was speculated to be venous congestion due to poor sinus drainage. The diffuse left temporal lobe white matter change can be attributed to the venous congestion or compression of the cortical surface by tight, thickened, adherent pachymeninges (1, 9). We think that in this case, it was probably caused by the latter because both cerebral angiography and MR venography revealed only nonopacification of the straight sinus; the cerebral edema in the temporal lobe is more likely related to obliteration of the transverse sinus by a tightened tentorium.
Most patients experience recurrence after treatment, but most imaging studies are performed within 1 year with little or no discernible difference observed during follow-up. Our case shows the comprehensive imaging findings during various stages of the disease. For instance, the focal nodular thickening at the left temporal lobe with little cerebral edema was first recognized in May of 1998 (Fig 3B) but with remission changes shown on the following MR images (Fig 4) obtained 1 month later with proper treatment. Reappearance of the dural mass at the same location with overwhelming clinical symptoms was noted almost 3 years later.
The pattern of dura involvement can be divided into two subgroups with good clinical and imaging correlation. Cranial nerve II, III, IV, V, and VI neuropathy is well correlated with involvement of cavernous sinus to optic canal and superior orbital fissure involvement. On the other hand, thickening of falcotentorial dura was usually associated with cranial nerve V, VII, VIII, IX, and X palsies. There is no published proposed staging of IHCP on the basis of clinical symptoms or based on imaging features, probably because of the limited number of reported cases. The classification of these two major patterns of dura involvement probably has more significant importance radiographically than clinically. As can be inferred from our case, the clinical symptoms worsened with gradual bilateral cranial nerve II and VIII involvements; the sequential imaging studies showed gradual diffuse involvement of tentorium, falx, and cavernous sinus, ultimately causing ischemic change of white matter from tightened pachymeninges. The dura involvement in most reported cases of IHCP can probably show progression to involve both hemispheres and from middle to posterior cranial fossa, or vice versa, without a rigid boundary, if followed for an extended period.
The cause of IHCP is still speculative at this moment, from infectious agent, mucopolysaccharidosis, and intrathecal toxin to fibrosclerotic disease (1). The diagnosis of IHCP relies on the exclusion of other possible causes of pachymeningitis, from granulomatous disease, such as neurosarcoidosis, neurosyphyllis, tuberculosis, and rheumatoid pachymeningitis, and Wegener’s granulomatosis to primary tumor of the meninx, en plaque meningioma, or dural carcinomatosis (10). The pathologic finding of a biopsy specimen is also diagnostic because it shows proof of chronic inflammatory response.
Corticosteroid therapy has shown effectiveness in alleviating symptoms and in arrest of clinical progression of IHCP (2, 4). In refractory cases, immunomodulators such as azathioprine have been used on the assumption that IHCP is an autoimmune disease (3). Reports of up to 50% and 66% of patients failing to respond to corticosteroid therapy or becoming dependent have also been presented. Unfortunately, in our case, treatment with corticosteroid and azathioprine had failed and surgical exploration for decompression was required. The patient recovered after surgery, but the disease progression was still uncertain at the time of this writing. It is possible that the patient may suffer from further deterioration if additional dura thickening is found at a different site.
Footnotes
Presented in part at the Nycomed Amersham Intercontinental Continuing Education in Radiology program held in Taipei, Taiwan, on September 29–30, 2001.
References
- Received March 7, 2002.
- Accepted after revision July 3, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Idiopathic hypertrophic pachymeningitis in a patient with a history of diffuse large B cell lymphoma
- Hypertrophic pachymeningoencephalitis associated with temporal giant cell arteritis
- Imaging Features of Meningeal Inflammatory Myofibroblastic Tumor
- Imaging Lesions of the Cavernous Sinus
- Idiopathic hypertrophic pachymeningitis